
Transoesophageal echocardiography (TOE) has become a useful diagnostic and monitoring tool in critical care settings, especially when transthoracic echocardiography is difficult to perform. It provides valuable information regarding mechanical ventilation, in obese patients, and in patients with surgical dressings and chest tubes. It is also feasible to perform TOE in a prone positioning [1, 2]. It allows visualization of deep cardiac structures and certain pathologies, including valve morphology, endocarditis, and patent foramen ovale, with better sensitivity than transthoracic echocardiography (TTE). It also makes it possible to visualize the superior vena cava, which can be useful in predicting fluid responsiveness in mechanically ventilated patients [1, 3, 4]. In addition, it is superior to TTE for the diagnosis of aortic dissection [1, 5], left atrial thrombus, and extracorporeal membrane oxygenation (ECMO) canula position [1, 6].
Critical care TOE is said to have extensive diagnostic implications. In a review of 20 studies in 2508 patients, TOE had a diagnostic impact in 67.2% of cases [1, 7]. It also has a substantial therapeutic impact leading to treatment changes in between 38% [8] and 79% of cases [9]. TOE is also safe to perform in critically ill patients, with a complication rate of 2.6% [7] reported in 2508 patients. No major complications were reported in a series of 152 TOE exasiminations performed by fellows [7, 10].
This article describes a systematic approach to critical care TOE examination with a detailed description of views necessary for rapid haemodynamic assessment in intensive care patients. It is concordant with the European Diploma in Advanced Echocardiography (EDEC) requirements, and its structural approach is based on the author’s experience acquired in the EDEC examination process.
EDEC is part of an educational program endorsed by the European Society of Intensive Care Medicine (ESICM). It is a curriculum in Echocardiography offered by ESICM to practitioners who have acquired a basic level of competence in critical care echocardiography (CCE) and would like to extend their competences to an advanced level.
According to the American Society of Echocardiography, there are 28 standard views often accompanied by Doppler measurements [10, 11]. TOE examination in critically ill patients has not yet been formally standardized. An extended TOE protocol (including non-standard views) in comprehensive TOE examinations carried out by cardiologists is not essential to achieve the goals defined by intensivists. The purpose of critical care TOE is to evaluate haemodynamically unstable patients [10]. The key is to develop a systematic approach to TOE examination and perform it in a repeatable sequence. The TOE examination presented in this article is based on “international consensus statement on training standards for advanced critical care echocardiography” (Expert Round Table on Echocardiography in ICU) [12]. When performed for the first time, it consists of all views essential to diagnose the patient and, when performed at subsequent examinations, it encompasses views necessary to monitor changes in the patient’s status. The figures presented in the following paragraph were selected due to their value for haemodynamic monitoring in patients in shock states.
CRITICAL CARE TRANSOESOPHAGEAL ECHOCARDIOGRAPHY VIEWS
We present critical care TOE examination in Tables 1 and 2. Table 1 is divided into 3 sections: how to obtain the view, exemplary findings and pathologies, and how we can use these views for haemodynamic assessment. Table 2 describes aorta visualization.
TABLE 1
Transthoracic echocardiography (TTE) views based on Expert Round Table on Echocardiography in ICU. International consensus statement on training standards for advanced critical care echocardiography [12]
[i] MO – mid oesophagus, TG – trasgastric, 4CH – 4-chamber view, 5Ch – 5-chamber view, LV – left ventricle, RV – right ventricle, SVC – superior vena cava, IVC – inferior vena cava, AV – aortic valve, MV – mitral valve, TV – tricuspid valve, PV – pulmonic valve, AS – atrial septum, VS – ventricle septum, PFO – patent foramen ovale, VTI – volume time integral, RVOT – right ventricle outflow track, LVOT – left ventricle outflow track, RWMA – regional wall motion abnormality
TABLE 2
Aorta visualisation in critical care transoesophageal echocardiography
FIGURE 1
Mid-oesophageal ascending aorta short-axis view (SAX). Anatomic structures indicated by arrows: SVC – superior vena cava, PA – pulmonary artery, RPA – right pulmonary artery, AscAo – ascending aorta
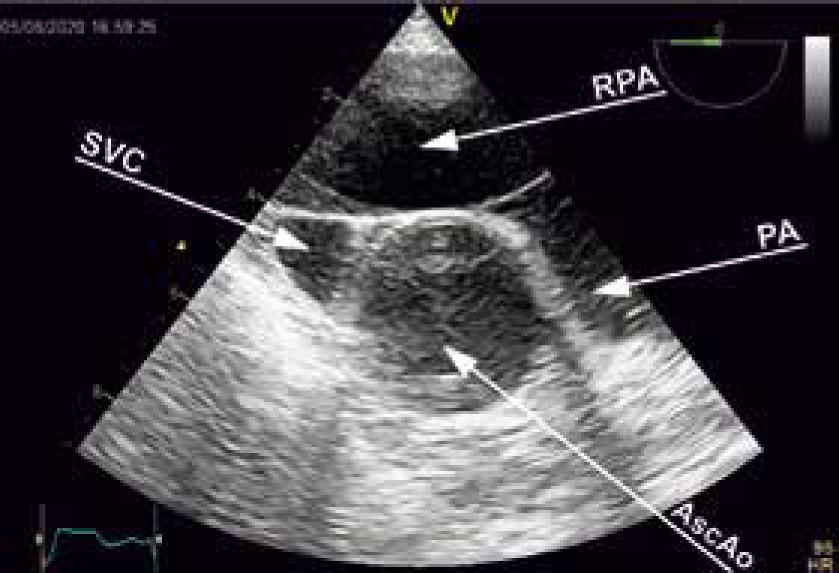
FIGURE 2
M-mode assessment of SVC collapsibility. Anatomic structures indicated by arrows: SVC – superior vena cava, RPA – right pulmonary artery
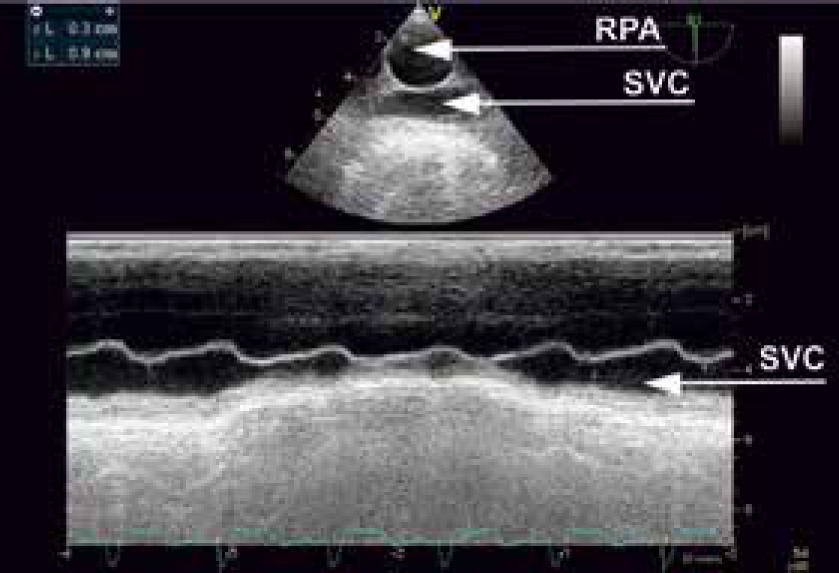
FIGURE 3
Mid-oesophageal 4-chamber view. Anatomic structures indicated by arrows: LA – left atrium, RA – right atrium, RV – right ventricle, LV – left ventricle
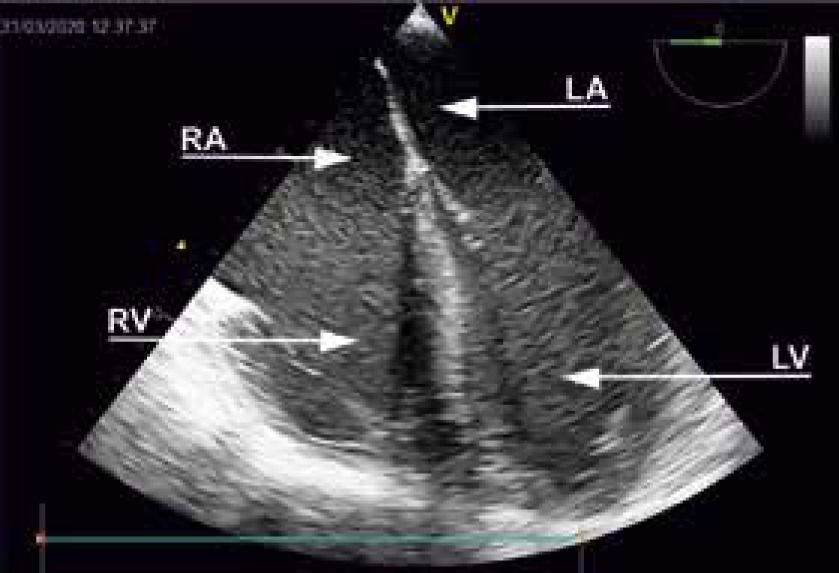
FIGURE 4
Mid-oesophageal aortic valve long-axis (LAX). Anatomic structures indicated by arrows: LA – left atrium, LV – left ventricle, RV – right ventricle, AscAo – ascending aorta

FIGURE 5
Transgastric mid SAX. Anatomic structures indicated by arrows: LV – left ventricle, RV – right ventricle
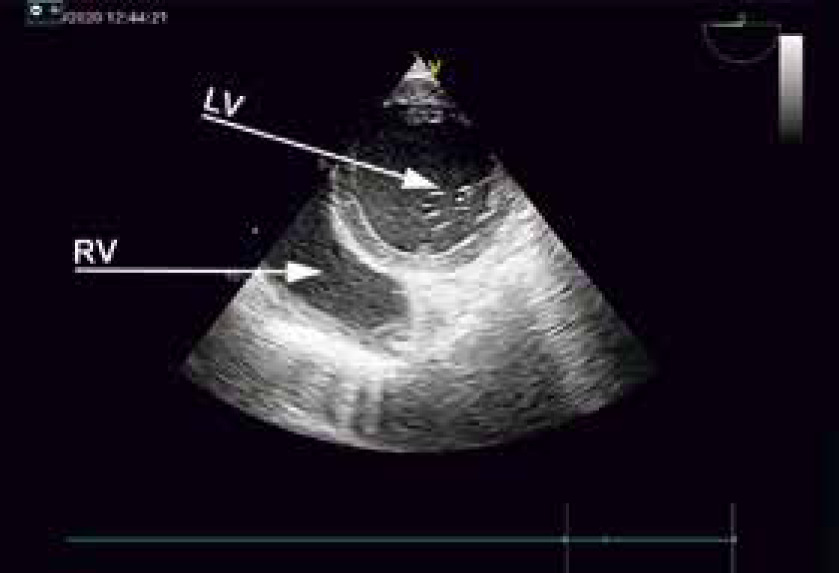
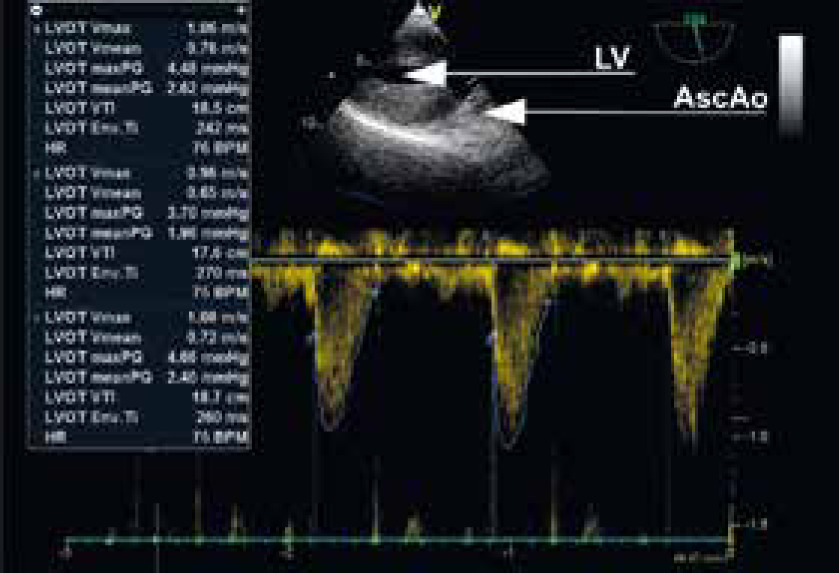
FIGURE 6
Transgastric LAX. PW – doppler through LVOT for VTI assessment. Anatomic structures indicated by arrows: LV – left ventricle, Ao – ascending aorta
Critical care TOE has evolved to become one of the most versatile modalities for diagnosing and guiding the treatment of critically ill patients [7]. It is less frequently performed in the ICU settings [13] compared to TTE. Nevertheless, TOE possesses many unique properties of an “ideal” haemodynamic tool [6, 14]. Vignon et al. [6] described 10 reasons to perform TOE in the ICU setting. It allows good visualization of heart structures and vessels not hampered by some TTE limitations (e.g. emphysema, high PEEP level in mechanically ventilated patients, obesity, fluid overload, dressings, and drains). TOE is a reliable source of information on the mechanism of circulatory failure (e.g. cardiac tamponade, thrombus in the proximal pulmonary arteries consistent with massive pulmonary embolism, etc.). In septic shock, it provides information on the main mechanism of circulatory failure, such as hypovolaemia, vasoplegia, and left or right ventricular systolic failure [6, 14]. TOE allows reproducible and sequential haemodynamic assessments and helps to predict fluid responsiveness [6]. Haemodynamic assessment, predicting fluid responsiveness, and finding the cause of shock are the main domains of critical care echocardiography. A clinician has to assess the patient quickly and decide on the treatment process; thus, goal-directed critical care TOE is often applied. Benjamin et al. [16] described goal-directed TOE with the use of 4 views. Vieillard-Baron et al. [17] described septic shock patients who had daily therapy guided by TOE. The typical views were as follows: mid-oesophageal 4-chamber view, transgastric midpapillary muscle view, and mid-oesophageal bicaval view for SVC assessment. This limited approach is especially useful for haemodynamic assessment and response to treatment [10]. The views described in this article are based on the “international consensus statement on training standards for advanced critical care echocardiography” [12]. The clinician can use any combination of views to answer the clinical question. We present critical care TOE in a table, with a short description of how to acquire the view, how to use it, and what views are most helpful for haemodynamic assessment. It is not our goal to describe all the pathologies found when performing TOE examination. Clinicians interested in the subject of pathologies assessed in TOE are referred to detailed articles [7, 10, 18]. We present only 1 method of view acquisition that we found to be easy and reproducible. At times, it is necessary to use different views or omniplanes to identify a cardiac structure or to make reliable measurements. Because critical care patients have multiple cardiac problems, cooperation with the cardiology department is very important in the field of valvular assessment, regional wall motion abnormalities, and qualification for invasive procedures. Establishing close relations with cardiology, cardiac surgery, and cardiac anaesthesia departments improves the diagnostic and treatment process of critically ill patients [6]. This article is dedicated to critical care physicians who possess some knowledge in echocardiography and who want to get ready for the EDEC examination. It is constructed as a brief curriculum and cannot be used as the sole source of information required for the exam. Acquiring competence in this technique has become part of the critical care training curriculum and is recommended by critical care societies [12].
Critical care TOE has a lot in common with critical care TTE. Many image planes are similar, but the only difference is the presentation on the screen. The manner of conducting the cardiac evaluation is the same, and haemodynamic assessment is based on Doppler measurements. The complete discussion on both methods is presented in a 2-part series in CHEST [10, 19, 20].
The main difference between these techniques is the method of image acquisition. In critical care TOE, the intensivist learns how to handle the probe introduced into the oesophagus or stomach [10]. In general, in TOE, the transducer is closer to the heart structures and thus produces a better image resolution. One consistent failure of TOE is the measurement of tricuspid regurgitation with Doppler due to the difficulty in achieving a Doppler angle. In the measurement of TR, TTE is recommended [10]. TOE is chosen over TTE when the physician cannot acquire good image quality with TTE, especially in mechanically ventilated patients – when there is an urgent need to determine the cause of haemodynamic instability. TOE can be performed in less than 15 minutes, it is less operator dependent than TTE [6, 21], and probe manipulation is actually easier with TOE than with TTE because the probe is well-positioned simply by being in the oesophagus [10]. Although it might be easier to perform TOE after a certain level of training, competence in TTE should precede the competence in TOE.
There are different data regarding the number of studies required to achieve competence in critical care TOE. Charron et al. [22] state that 31 studies under supervision are sufficient for competent acquisition [10]. The advanced critical care statement [12] requires a minimum of 35 studies of good quality. It also states that more studies might be required if the quality is not optimal [10]. Thirty-five TOE examinations are also required to fulfil the criteria for the European Diploma in Advanced Echocardiography (EDEC) examination process. EDEC requires the trainee to be supervised by a cardiologist and intensivist who have mastered the knowledge of advanced critical care echocardiography. As far as TTE is concerned, a minimum of 100 studies is required to achieve a sufficient level of competence to perform TTE without supervision [12]. It is optimal for an intensivist to work with a cardiologist during training. This provides expert assistance in image acquisition and interpretation.
Critical care TOE is a minimally invasive procedure and can be safely performed in the ICU setting. Critical care patients are very often sedated and mechanically ventilated so that the introduction of a probe can be safely performed with a laryngoscope. The patient is well-monitored, and any change in their condition can be quickly identified. Critical care TOE is safe with a low complication rate (2.6%). The most commonly reported complications were circulatory disturbances, such as hypo- or hypertension, superficial mucous lesions, hypoxaemia, arrhythmias, and dislodgement of nasogastric or nasojejunal tubes [7, 18]. However, complications of TOE performed in the emergency department were more frequent than in the ICU. In one series of 142 emergency department TOEs, there were 18 complications (12.6%): respiratory insufficiency/failure (7), emesis (4), hypotension (3), agitation (2), death (1), and cardiac dysrhythmia (1) [23].
Critical care TOE is contraindicated in active gastrointestinal (GI) bleeding, perforated viscus, and oesophageal pathologies: laceration, perforation, stricture, tumour, and diverticulum. Relative contraindications encompass the following: history of neck and mediastinum radiation, previous GI surgery and bleeding, Barrett’s oesophagus, history of dysphagia, restriction of neck motility, symptomatic hiatal hernia, oesophageal varices, coagulopathy, thrombocytopaenia, active oesophagitis, and active peptic ulcer disease [10, 17]. We strongly encourage intensivists to perform critical care TOE on a regular basis, keeping in mind its limitations and contraindications. Advances in technology, such as miniaturized probes, 3D-ultrasound, and automatic flow measurement, will expand the role of TOE in critical care. It does not replace other techniques of advanced haemodynamic monitoring. It provides different information compared to pulmonary artery catheter or thermodilution indicator technique, and thus the methods are not competitive but complementary [18].
The systematic approach to critical care TOE examination presented in this article can be helpful in acquiring basic skills to learn this technique.
CONCLUSIONS
We present a structural approach to TOE exa-mination in critically ill patients. Performing TOE in an organized fashion will help to pinpoint most of the pathologies and monitor the treatment process. TOE is a quick, easy, and operator-independent dia-gnostic method, which can be successfully taught in any intensive care unit.