
Neuromuscular monitoring is proposed to be part of standard anaesthetic monitoring to objectively assess the effects of non-depolarising neuromuscular blocking agents (NMBA) [1, 2]. NMBA’s use during anaesthesia induction enables the optimisation of intubation conditions during conventional laryngoscopy [3]. The current clinical standard for neuromuscular monitoring is acceleromyography [4]. In most cases, an electrical stimulus is passed through adhesive electrodes that are placed over the ulnar nerve on the medial lower arm to stimulate the nerve (e.g., TOF-Scan, TOF-Watch). The stimulated motor response is then measured in the form of acceleration. The most commonly applied pattern is the train-of-four (TOF), in which the motor responses from the fourth and first stimuli are compared and expressed as a percentage, also known as the TOF ratio. With the increasing effect of NMBA, less than four responses will be recorded; the remaining ones are reported as the TOF count (4 to 0). These measurements are recorded between a TOF ratio of 100% (i.e., no measurable neuromuscular block) and a TOF count of 0 (i.e., no measurable muscle response) [1, 2].
A new type of neuromuscular monitor, TOF-Cuff (RGB Medical, Spain), requires no additional electrodes for stimulation [5]. Instead, it offers an integrated system in which electrodes are built directly into a blood pressure monitoring cuff. While stimulation is applied to the plexus brachialis, integrated sensors measure the response of activity in the muscles of the upper arm by quantifying the resulting pressure changes in the cuff. The potential advantages of such a system include ease of application and use, no prerequisite of “ideal positioning” of the lower arm, and the elimination of expensive components sometimes required by standard monitors. The use of this newly released device has been described, but its merits, when compared to standard devices, have not been tested extensively [5].
This study compared a current clinical standard acceleromyography device (TOF-Scan (Dräger, Germany)) with the more recently developed TOF-Cuff. The primary endpoint was the time required from the administration of a neuromuscular blocking agent to a TOF ratio response of 0%. We hypothesised that the time required would not vary significantly between the two devices.
METHODS
This prospective, controlled, observational study was conducted after approval from the Ethics Committee East Switzerland (Ethikkommission Ostschweiz, EKOS; BASEC-nr. 2016-02044) was granted, and it was registered with the German Clinical Trials Register (www.DRKS.de, DRKS00012373). Written informed consent from patients was obtained before inclusion.
As a preliminary step, we collected baseline data on the intra-patient variability when performing neuromuscular monitoring with the standard clinical device used at our hospital (TOF-Scan). Measurements were done with TOF-Scan devices simultaneously applied to each of the patients’ arms. For the comparison of TOF-Cuff to TOF-Scan, we measured train-of-four ratios by simultaneously applying the TOF-Scan and TOF-Cuff to opposite arms. The primary endpoint for both the pre-study and the study was the time required to reach a TOF ratio of 0% after the administration of a non-depolarising neuromuscular blocking agent during anaesthetic induction. Patients were grouped according to their body mass index (BMI).
The primary inclusion criteria were patients undergoing surgery at the Cantonal Hospital in Frauenfeld (Kantonsspital Frauenfeld) who required both general anaesthesia and the administration of non-depolarising neuromuscular blocking agents for anaesthetic induction according to institutional protocols. For the baseline group, we included patients with a BMI of < 30 kg m−2 (Group SS). For inter-device comparisons, we included additional patients with a BMI of < 30 kg m−2 (Group SC) and a second group with a BMI of ≥ 30 kg m−2 (Group SC-BMI). Exclusion criteria for all study groups were: emergency cases, pregnant patients, those with a neuromuscular disease, those with a contraindication to atracurium, and patients already enrolled in this or another study.
The TOF-Scan was used as the control device. It is a three-dimensional acceleromyography device that assesses the movement of the thumb in multiple planes while the thumb is placed in a specially designed hand stabilizer with integrated piezoelectric sensors. TOF-Scan was recently established as a standard monitoring device for clinical studies and was rated as a clinically sufficient neuromuscular monitor [4, 6, 7]. The pre-programmed impulse for stimulation of the ulnar nerve is 60 mA. The minimum time between TOF measurements is 15 seconds (s).
As the investigative device, we used the TOF-Cuff, which is designed to act as both a typical non-invasive blood pressure and neuromuscular monitor. It offers the same stimulation patterns as TOF-Scan, namely the train-of-four. TOF-Cuff includes integrated electrodes within the blood pressure cuff to stimulate the brachial plexus of the upper arm (standard current 40 mA). The muscular response is then measured using integrated sensors within the same cuff. The minimum time between measurements is 12 s. There are different cuff sizes available, according to upper arm circumference.
Following institutional protocols, patients were pre-medicated orally with 7.5 mg midazolam 30 minutes before induction. While in the induction room, patients underwent standard monitoring (i.e., ECG, NIBP, SpO2), as well as modified EEG monitoring using the bispectral index (BIS) before peripheral intravenous access was attained. The TOF-Scan was applied to the infusion arm using the supplied hand stabiliser, while the recommended TOF-Cuff cuff size was fitted on the opposite arm using upper arm circumference as a guide. Both arms were allowed to lie unrestrained during the anaesthetic induction.
Patients received pre-oxygenation and 1.5 μg kg−1 fentanyl prior to induction with propofol target-controlled infusion (TCI) using an effect-compartment concentration (ce) of 6 μg mL−1. In order to reduce the pain associated with the propofol injection, patients received a 20 mg lidocaine intravenous injection. Our study protocol allowed for dose variation, as well as an additional 0.15 μg kg−1 min−1 of remifentanil by the attending anaesthetist. After loss-of-consciousness – defined as BIS < 60 – both neuromuscular monitors were simultaneously started. For the TOF-Scan, reference values (normalisation) were obtained before the administration of the NMBA. Only after the establishment of a stable baseline measurement (i.e., 3 × TOF = 100%) was 0.5 mg kg−1 atracurium intravenously administered. Anaesthesia was maintained using propofol-based TCI. The anaesthesia induction protocol was aligned with the existing institutional standard.
Both demographic data and details of the anaesthesia procedures were collected. Specifically, we noted the sides to which the TOF-Cuff and TOF-Scan were applied, whether the patient was left- or right-handed, and which TOF-Cuff cuff size was appropriate. We recorded the values of the TOF measurements every 15 s. In the event that a measurement was ongoing, the value was recorded immediately after measurement. The values from both devices were recorded until both monitors showed a TOF ratio = 0%. The number of attempts at successful tracheal intubation and technical problems relating to both devices were recorded. At the end of the anaesthetic course, patients were examined for any lesions or adverse reactions relating to either device.
Continuous data were assessed for normality distribution and, accordingly, were presented as either mean (± SD) or median (interquartile range). Categorical data were presented as absolute numbers and percentages, and were then compared with χ2 or Fisher’s exact test. Bias and limits of agreement were calculated, and Bland-Altman plots were created for all three groups. In addition, Lin’s concordance correlation coefficient (LCCC) was measured for all 50 patients. The intragroup comparison of onset time from the administration of the NMBA until TOF ratio = 0% measured by both monitors was compared using the Wilcoxon signed rank test. The difference between both neuromuscular monitors obtained in Group SC was compared with Group SC-BMI using the Mann-Whitney U test. For all comparisons, P < 0.05 was considered statistically significant.
For all subgroups, the predictive accuracy of TOF-Cuff was determined. We used the TOF-Scan (specifically, the slower TOF-Scan in Group SS) as a clinical standard and calculated how often TOF-Cuff (and the faster TOF-Scan in group SS) indicated readiness for tracheal intubation when the standard did not [8]. Data analysis was performed using Stata version 15.1 (StataCorp, College Station, Texas, USA).
RESULTS
A total of 70 patients were assessed for inclusion in one of the three study groups. Twenty patients were assigned to bilateral neuromuscular monitoring by TOF-Scan (Group SS). For the comparison of the TOF-Cuff with TOF-Scan, 25 patients were included in the < 30 kg m−2 BMI group (Group SC), and 25 obese patients were in the ≥ 30 kg m−2 BMI group (Group SC-BMI). Demographic data, according to the patient groups, are presented in Table 1.
TABLE 1
Demographic data of patients according to study group
| Characteristic | Group SC (n = 25) | Group SC-BMI (n = 25) | P-value (SC vs. SC-BMI) | Group SS (n = 20) |
|---|---|---|---|---|
| Agea (years) | 56 (± 18) | 50 (± 17) | 0.1798c | 58 (± 16) |
| Gender (female), n (%) | 16 (64) | 17 (68) | 0.0891 | 15 (75) |
| ASA physical statusb I–IV | 2 (2–3) | 3 (2–3) | 0.0349d | 2 (2–2) |
| Heightb (m) | 1.65 (1.6–1.8) | 1.64 (1.6–1.7) | – | 1.66 (1.6–1.7) |
| Weightb (kg) | 67 (65–76) | 100 (91–120) | – | 70 (66–75) |
| Body mass indexb (kg m−2) | 26 (24–27) | 36 (33–42) | – | 25 (23–28) |
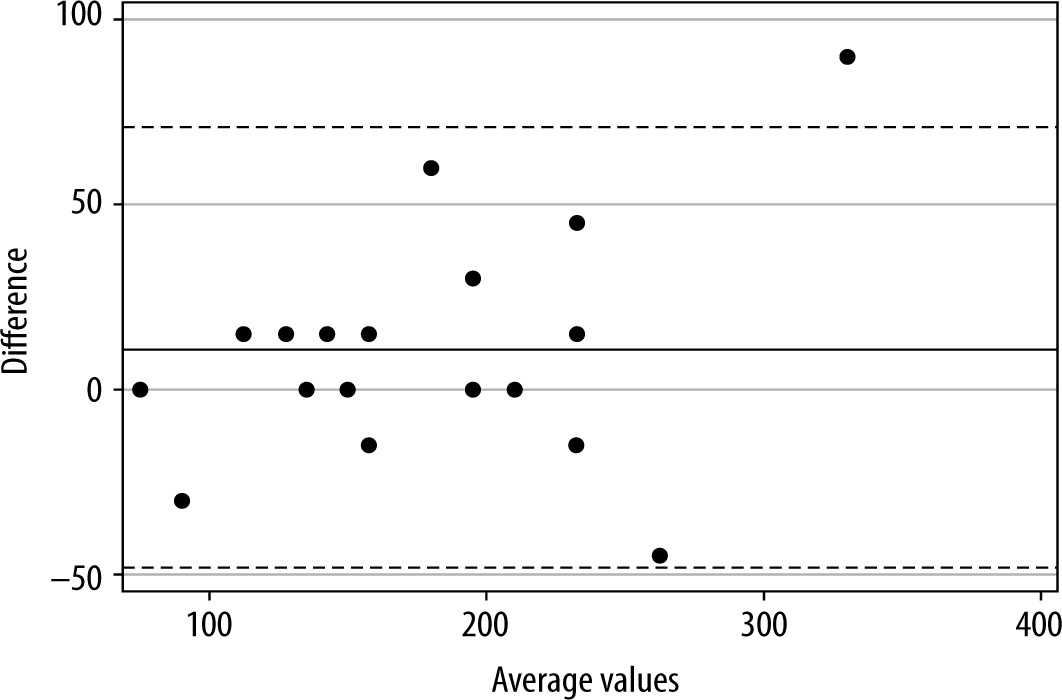
For the baseline group of bilateral comparisons using the TOF-Scan (Group SS), the mean time (± standard deviation) from the administration of the neuromuscular blocking agent to TOF ratio = 0% was 180 s (± 69) on the left side, and 172 s (± 58) on the right side (P = 0.1137). TOF-Scan was faster to show TOF = 0% in 4 cases (20%) on the left side, 10 cases (50%) on the right side, and the remaining 6 (30%) were equal. Bias for Group SS (left vs. right) was 11 s (± 30) with limits of agreement of −48 to +71 s. Figure 1 shows the Bland-Altman plot for Group SS.
Overall, the TOF-Cuff was mounted on the upper right arm in 39% of the cases. All patients in the study were right-handed. The standard adult size TOF-Cuff was used on all but eight patients (32% had a large cuff) in Group SC-BMI. All patients underwent intravenous anaesthetic induction by propofol and fentanyl (TCI 6.0 μg mL and 0.12 ± 0.04 mg, respectively). Forty-six percent of the study patients also received remifentanil for anaesthetic induction. Patients in groups SS, SC and SC-BMI received 0.5 ± 0.04 mg, 0.5 ± 0.03 mg, and 0.5 ± 0.1 mg atracurium per kg body mass intravenously, respectively.
When comparing TOF-Scan with TOF-Cuff in the entire cohort (n = 50), the bias was −7.7 s (± 54.1) with limits of agreement of −113.7 to +98.4 s. Table 2 presents the results of the intra- and intergroup comparisons between the TOF-Scan and TOF-Cuff. The onset time from administration of neuromuscular blocking agent to TOF ratio = 0% was significantly different between the TOF-Scan and TOF-Cuff in Group SC-BMI but not in Group SC (Wilcoxon signed rank sum test). With both measurement devices, Group SC-BMI reached TOF ratio = 0% faster than Group SC. However, this intergroup difference was most notable in the TOF-Cuff. Lin’s concordance correlation coefficient was 0.81 (95% CI: 0.68–0.89) for TOF-Cuff versus TOF-Scan (all patients).
TABLE 2
Intra- and intergroup comparisons of onset time, in seconds, from administration of neuromuscular blocking agent to TOF ratio = 0%
| Device type | Group SC | Group SC-BMI | Intergroup comparisonb |
|---|---|---|---|
| TOF-Scan® | 165 (IQR 120–180) | 143 (IQR 105–180) | P = 0.2548 |
| TOF-Cuff® | 150 (IQR 120–180) | 120 (IQR 90–165) | P = 0.0474 |
| Intragroup comparisona | P = 0.702 | P = 0.0139 |
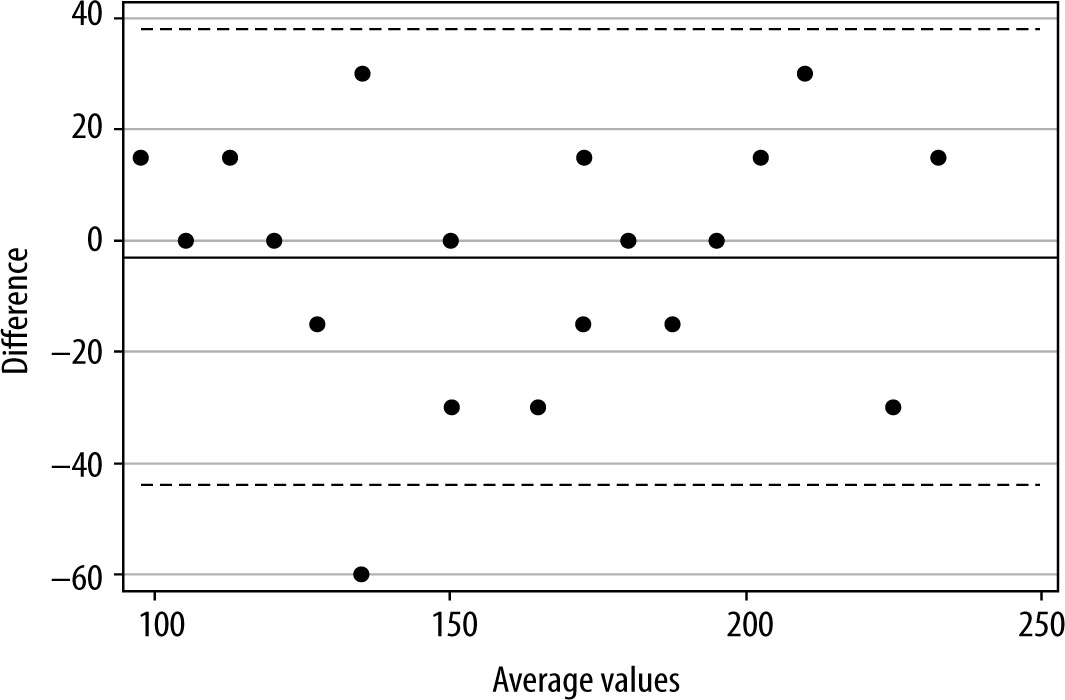
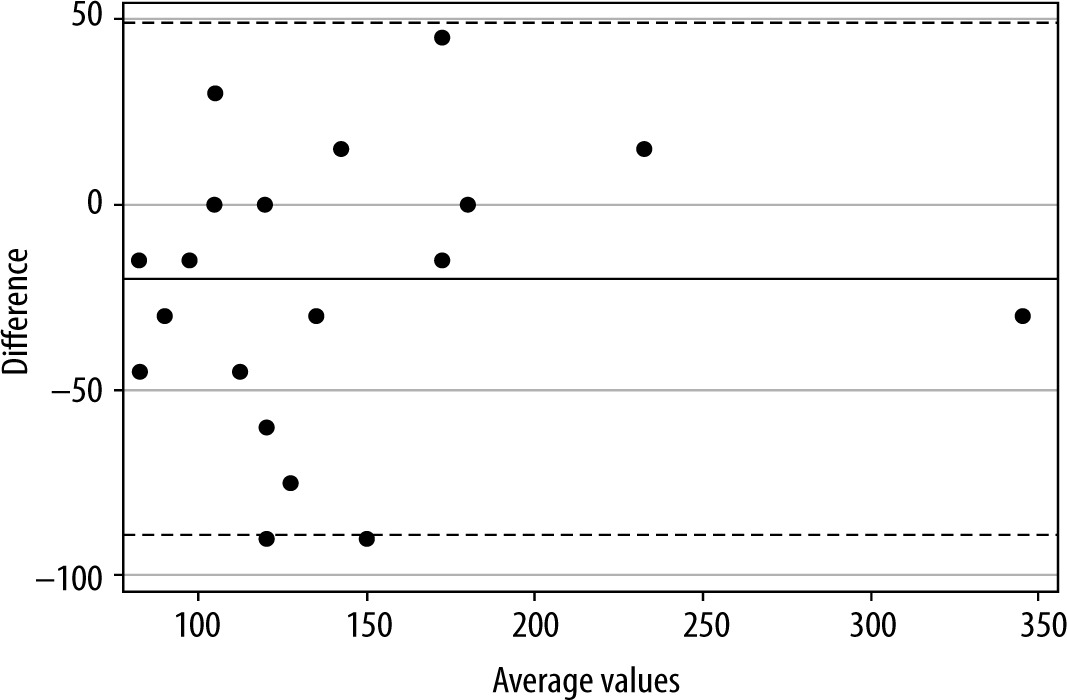
Bias for Group SC was −3 s (± 21.2) and limits of agreement were −44.7 to +38.4 s. Bias for Group SC-BMI was −20 s (± 35) with limits of agreement of −88.6 to +48.6 s. Figures 2 and 3 show the Bland-Altman plots for groups SC and SC-BMI, respectively. The predictive accuracy for the faster versus slower TOF-Scan in group SS was 30%. More precisely, in 14 of 20 cases the faster device indicated readiness for tracheal intubation when the slower device did not (maximum TOF-ratio still at 70%). For groups SC and SC-BMI, when TOF-Scan was used as the clinical standard, the corresponding cases that did not match were 11 of 25 (56%) and 12 of 25 (52%), respectively – with maximum TOF ratios still shown by the standard exceeding 90%.
All patients were successfully intubated on the first attempt. Twenty-two percent (11/50) of the patients had at least one technical problem (defined as “no result” or “error message”) with a TOF-Cuff measurement, and 18% (9/50) had at least one problem with a TOF-Scan measurement. Of the 11 patients with TOF-Cuff problems, 7 (64%) were in the obese group. However, the frequency of problematic readings did not differ significantly among the groups. Finally, none of the patients experienced an adverse reaction at neuromuscular monitoring sites after the measurements.
DISCUSSION
We compared the onset time to TOF ratio of 0% after the administration of a commonly used neuromuscular blocking agent in conventional dosing by using two neuromuscular monitoring devices during anaesthetic induction under routine clinical conditions. In contrast to findings among the obese patients, there was no significant systematic difference between the onset times measured by the two devices in non-obese patients. However, large limits of agreement and clinically relevant differences in individual patients were observed.
Non-depolarising neuromuscular blocking agents are widely used in the field of anaesthesia. They optimise intubating conditions during anaesthetic induction [3, 9], and they can be used intraoperatively to facilitate ideal operating conditions [10]. High-quality guidelines for monitoring patients receiving NMBA have been published [1, 2]. Quantitative or objective assessment of the degree of blockade is considered far superior to qualitative or clinical assessment. The most critical parameter to monitor is the recovery from neuromuscular blockade. However, to reduce the likelihood of intubation-related complications (e.g., unsuccessful intubation, multiple attempts, traumatic intubation, hypoxia), neuromuscular monitoring is applied during anaesthetic induction.
Nevertheless, neuromuscular monitoring continues to be underused [1, 11, 12]. One probable explanation is that suboptimal management of neuromuscular blockade is not immediately evident to the anaesthetist, and it is not often viewed as causal. Problems such as vocal cord lesions may only present after discharge from anaesthetic care, or a patient may develop pneumonia later after silent aspiration during or shortly after extubation. These problems would likely be due to the degree of neuromuscular block, though it is unlikely the anaesthetist would be made aware of them [1]. Equally likely is that the currently available neuromuscular monitors are sometimes challenging to use or prone to error due to the position of the patient and surgeon [1]. Likewise, some devices are more susceptible to breakage, and replacement parts are expensive.
Concerning our study’s findings, bias and limits of agreement between TOF-Cuff and TOF-Scan were comparable to those found during the intra-patient comparison with TOF-Scan on both arms. Although not statistically significant in the non-obese study population, the tendency to arrive at TOF ratio = 0% was faster with the TOF-Cuff than the more peripheral TOF-Scan. There were intra-patient differences of up to 60 s when the TOF-Cuff recorded TOF = 0% earlier. Similar results were reported for anaesthetic induction when comparing a standard acceleromyographic neuromuscular monitoring device (TOF-Watch) to TOF-Scan [4]. In other patients, however, TOF-Scan was up to 30 s faster than TOF-Cuff. For tracheal intubation, this difference could be clinically relevant. In the group of obese patients, TOF-Cuff indicated readiness for intubation significantly earlier.
The differences we found may be due to our monitoring methods or the muscle groups we assessed. Specific muscles, such as the diaphragm, are considered relatively resistant to NMBA when compared to the more delicate musculature of the hand (adductor pollicis) or glottic musculature [2]. Consequently, these muscles take longer to reach complete neuromuscular block. Until now, the majority of quantitative TOF measurements have been taken using the ulnar nerve and adductor pollicis brevis muscle. It is plausible that ideal values according to each anatomic location or muscle (group) need to be defined [13]. Similarly, the response to neuromuscular stimulation assessed at the upper arm may be more challenging to detect than the response of the thumb. This phenomenon would be particularly relevant when treating obese patients. A shortcoming of both devices is that there is no possibility to individually determine supramaximal current [13], which may also play a more prominent role in obese patients [13].
The bias between the two neuromuscular monitors was not larger than the bias between TOF-Scan bilateral comparisons, indicating that the currently available tools for neuromuscular monitoring might lack the sensitivity to precisely detect the onset of neuromuscular blockade. Thus, the question remains: which device is valid? We concede that conclusions from these findings are constrained by our relatively small and homogeneous study population. Our sample size was, nevertheless, similar to other comparative studies of two neuromuscular methods (n = 20–55) [4, 6, 14, 15]. Moreover, we did not assess the increasing effect of the NMBA until complete deep block was attained, as indicated by a TOF count value of 0. Following our institutional standard, we began laryngoscopy when a TOF ratio of 0% (corresponding to a TOF count from 0 to 3) was reached. Consequently, tracheal intubation can be performed quickly and safely, assuming that a deepening of the block occurred between laryngoscopy and intubation [13].
One central limitation of our study was that while TOF-Scan can be considered a clinical standard, the gold standard for monitoring of neuromuscular function is mechano- or electromyography. Since 2007, the classic TOF-Watch SX has been recommended for studying neuromuscular blocking agents when using acceleromyometry [13]. For our study, TOF-Scan was the only option for the clinical standard of acceleromyography since TOF-Watch is no longer available in Switzerland. TOF-Scan is being distributed for patient monitoring by large scale manufacturers, it is widely used in clinical practice, and it is considered suitable for use in research [4]. Another limitation is that we assessed the onset of the neuromuscular blockade after the administration of the NMBA only. In terms of patient safety, the recovery from neuromuscular blockade is considered a more critical issue. Since our patients were not treated according to a study protocol after anaesthetic induction, there was a mix of patients receiving various atracurium re-dosing schemes, which may have hindered proper assessment of recovery. Concerning our study design, a benchmark indicating a clinically significant difference between methods was not established a priori, which impedes further inferences about the limits of agreement. Finally, we did not monitor the performance of the cuff pressure of the TOF-Cuff device because we had too few time points to conduct assessments during anaesthetic induction. However, Veiga Ruiz et al. [5] found that the arterial blood pressure monitoring was sufficient and in accordance with European standard 93/42/EEC.
Further studies are needed to explore the differences found in this study – are they reproducible and, if so, what are the reasons for these differences? Future research projects could assess the differences between measurements on dominant and non-dominant arms, the effectiveness in paediatric anaesthesia or in rapid sequence induction, and the variations in TOF measurement during recovery from the neuromuscular block before tracheal extubation.
CONCLUSIONS
Monitoring of neuromuscular transmission with the TOF-Cuff device remains questionable, even with its interesting and distinctive features. The device needs to be correlated with clinical endpoints before it is widely promoted for clinical use. When compared to TOF-Scan, we found wide intra-individual differences and limits of agreement. These devices cannot be used interchangeably.