
INTRODUCTION
Annular skin lesions have a heterogeneous aetiology, ranging from commonly occurring fungal dermatoses, autoimmune vesicobullous diseases, connective tissue disorders to other unusual dermatoses. The lesions often coalesce forming circinate, serpiginous patterns. These conditions tend to mimic each other clinically hence appropriate investigations are imperative for diagnosis of atypical variants.
CASE REPORT
A 63-year-old woman presented with scaly, erythematous, pruritic lesions over the chest, which had progressively extended over 3 months to the axillae, back, upper limbs, scalp, and face, predominantly in a seborrheic distribution. She reported episodes of fluid-filled lesions that ruptured to form erythematous, eroded, and crusted areas. She initially experienced white flaking over the scalp followed by pruritic erythematous lesions on the back, diagnosed and treated as superficial fungal infection/seborrheic dermatitis without improvement. The lesions continued to progress, prompting the current presentation. She denied photosensitivity, intolerance to spicy foods, ocular burning, or urinary symptoms. Her medical history was significant for hypothyroidism and hypertension, both under treatment.
As mentioned in the first paragraph of the case report, the patient was initially diagnosed with dermatophytosis and seborrheic dermatitis based on the scalp and facial involvement in a seborrheic distribution. Accordingly, the patient was treated with adequate oral and topical antifungal therapy. However, there was no clinical response to treatment. Subsequently, with the progression of lesions into fluid-filled and erosive areas, an infectious etiology, including dermatophytosis, was considered unlikely and hence ruled out, prompting evaluation for autoimmune causes.
Clinical differential diagnoses considered included pemphigus foliaceus, pemphigus vulgaris, subacute cutaneous lupus erythematosus (SCLE), and pemphigus erythematosus.
Later, the lesions assumed an annular morphology with complete central healing and peripheral pustules (Figure 1 B) prompting us to broaden our differential diagnosis to include subcorneal pustular dermatosis (SCPD) and IgA pemphigus.
Figure 1
A – Multiple erythematous coalescing circinate erosive plaques with central yellowish greasy crusting surrounded by peripheral scaling with few pustules and flaccid bullae on the back. B – Annular morphology with central clearing and peripheral pustules. C – Erythematous plaques with central hyperpigmented crusting and peripheral scaling over eyelids, central face and perioral region

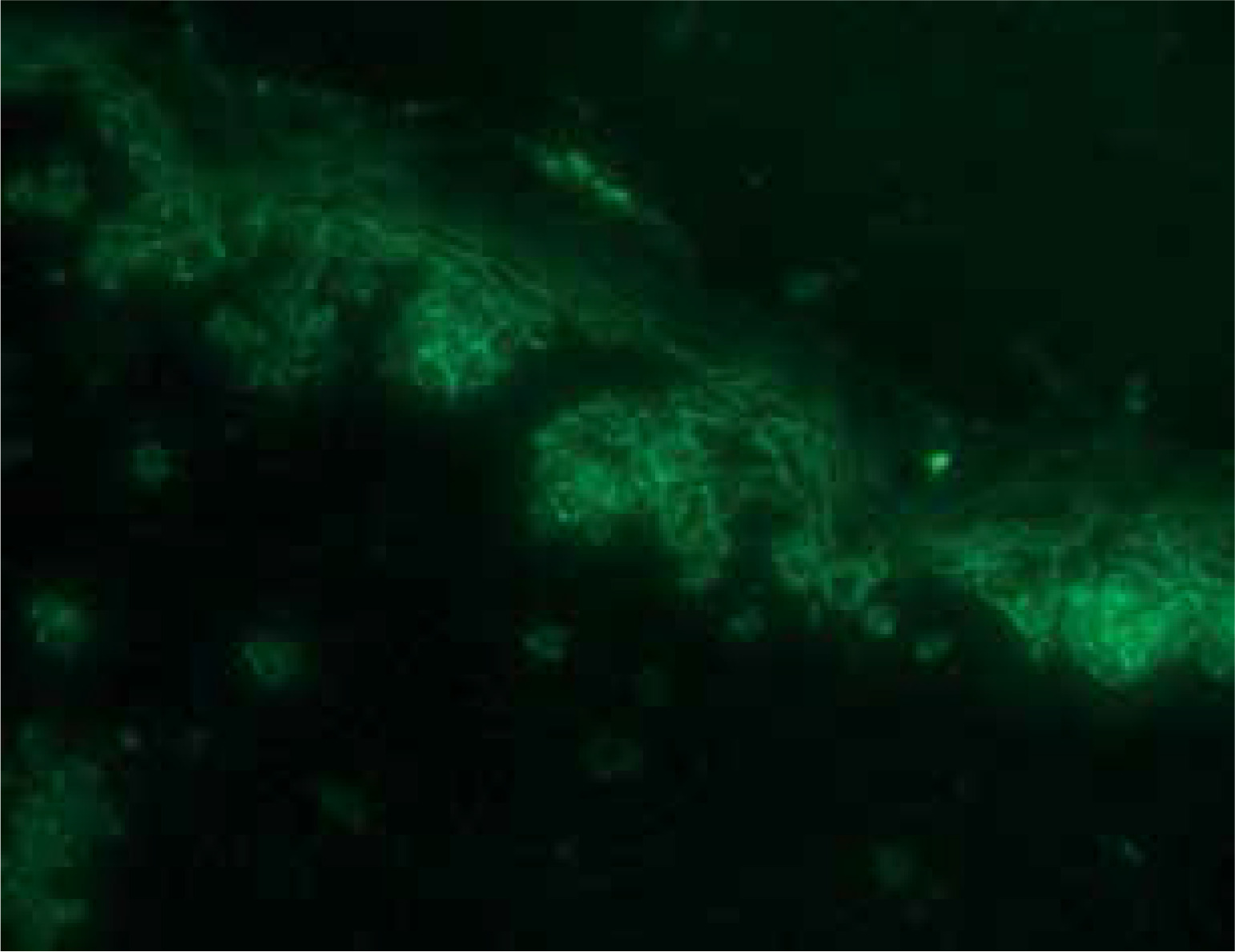
On investigation, the peripheral blood smear showed neutrophilia. Hemogram and other routine tests were within normal limits. Antinuclear bodies (ANA) were not detected. Radiological investigations revealed no abnormalities. Tzanck smear was unremarkable. Skin biopsy showed a subcorneal vesicle filled with neutrophils, absent acantholysis, and dermal perivascular and periductal lymphoplasmacytic infiltrate. Direct immunofluorescence (DIF) demonstrated a fish-net pattern of intercellular IgG (++) deposits in the epidermis. IgA, IgM, C3 were negative (Figures 2, 3). On enzyme-linked immunosorbent assay (ELISA), anti-Dsg1 titres were elevated (72.66; cut-off < 20), while titres of anti-Dsg3 were negative (< 2; cut-off < 20) (Euroimmun kit). Based on these findings, a diagnosis of the annular neutrophilic variant of pemphigus foliaceus was made. The patient was treated with dexamethasone injection (1 mg/kg) (equivalent to 40 mg prednisolone), tapered off by 10 mg every week. Mycophenolate mofetil (MMF) 500 mg once daily was introduced as a steroid-sparing agent, and dapsone 100 mg once daily was initiated to address neutrophilia. Both medications were subsequently discontinued due to elevated transaminase levels, after which colchicine 0.5 mg twice daily was started. Topically the patient was treated with framycetin cream for the erosions and fluocinolone acetonide 0.25% cream was applied for the erythematous plaques. The scalp lesions were treated with a combination of ketoconazole and beclomethasone dipropionate lotion. Due to persistent new lesions and comorbidities, intravenous rituximab (RA protocol: 1 g at week 0 and week 2) was administered [1, 2]. The patient improved significantly (Figures 4 A–C), and has been in complete remission for 8 months, maintained on colchicine 0.5 mg twice daily.
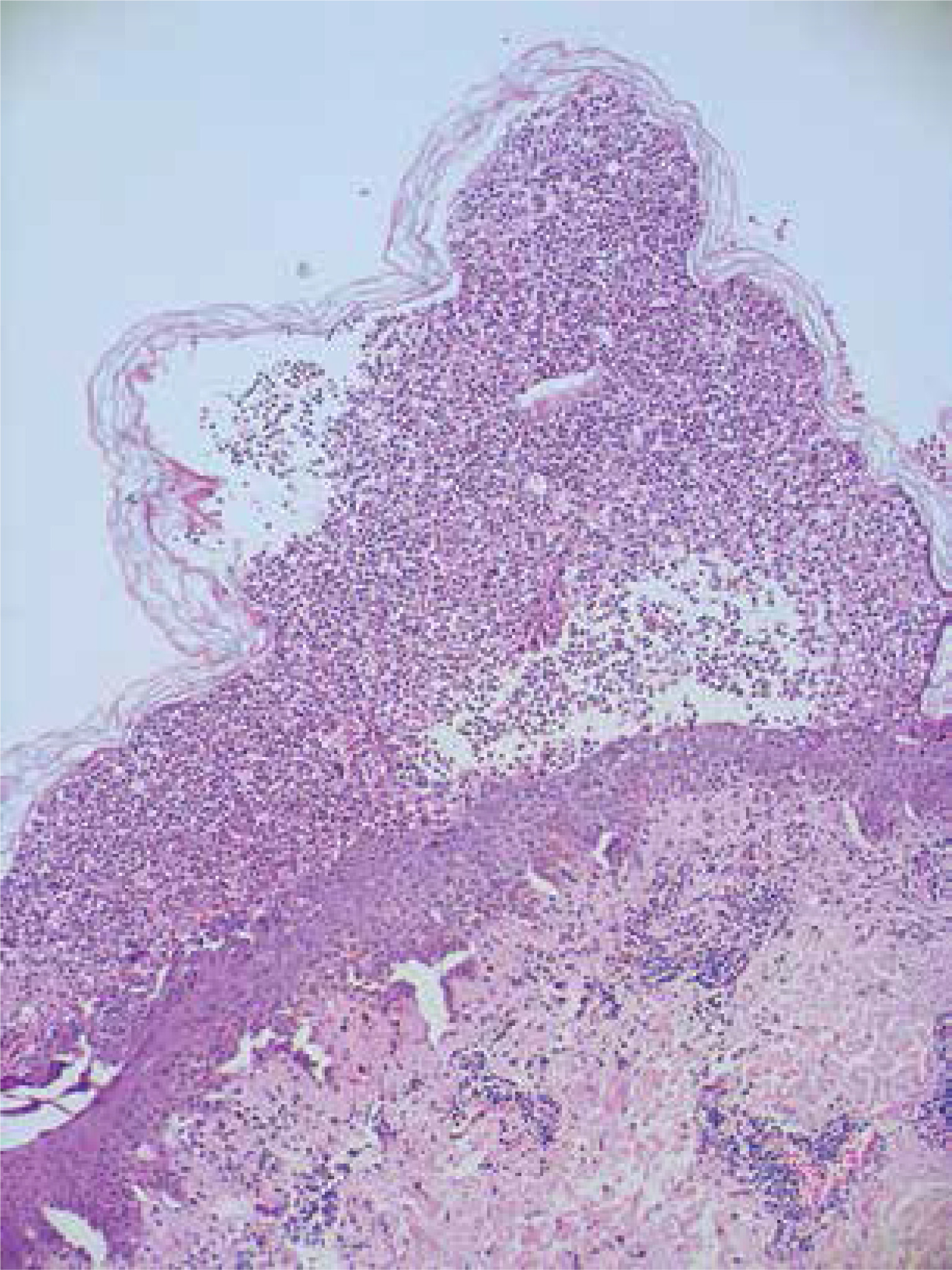
Figure 2
Photomicrograph (H&E 100×) Subcorneal vesicle filled with neutrophils, absent acantholysis, and dermal perivascular and periductal lymphoplasmacytic infiltrate

DISCUSSION
Pemphigus foliaceus is an autoimmune disease with antibodies against desmosomal protein Dsg1, typically showing flaccid blisters and superficial erosions with crusting in a seborrheic distribution, along with classical histopathological findings of subcorneal split and acantholysis. However, our case showed annular erythematous plaques with scaling, crusting, and peripheral pustules. Biopsy revealed a subcorneal neutrophilic vesicle without acantholysis. This annular neutrophilic variant is uncommon, with few cases reported. Annular plaques with peripheral pustules and neutrophilic infiltration, without acantholysis on histopathology, distinguish this form [3]. The absence of acantholysis does not rule out pemphigus as acantholysis on histopathology is not specific of pemphigus but rather suggestive of it. Acantholysis can also be seen in other diseases like Darier’s disease, Hailey-Hailey disease, Grover’s disease, acantholytic dermatosis localized to the vulvocrural area, linear epidermal nevus, warty dyskeratoma, acantholytic acanthoma [4]. Biopsy specimens of early lesions or patients without the typical blister presentation as seen in our case may lack acantholysis and present with eosinophilic or neutrophilic spongiosis [5]. Neutrophil accumulation can be due to secondary superinfection of older subcorneal vesicles or erosions, which may prompt consideration of various conditions presenting with subcorneal neutrophilic pustules. Intercellular IgG deposits confirmed pemphigus, differentiating it from SCPD (lacking immunoreactants) or IgA pemphigus (with intercellular IgA). Negative ANA ruled out SCLE and pemphigus erythematosus in our case. Pemphigus vulgaris was precluded due to the absence of mucosal involvement and negative anti-Dsg 3 antibodies. As histopathological examination (HPE) cannot detect the autoimmune mechanisms specific to pemphigus vulgaris (PV) and pemphigus foliaceus (PF), immunological tests like DIF and ELISA, are essential for diagnosing pemphigus [4].
Over time, several pemphigus variants have been described. One of the earliest reports documented a form characterized by prominent neutrophilic pustules and erythroderma [6], with similar presentations subsequently reported by other authors [7, 8]. Another case described overlapping features with annular pustular psoriasis, suggesting a potential association between pemphigus and other neutrophilic dermatoses [9]. A comparable presentation featuring circinate plaques and neutrophilic pustules in a younger patient has also been noted [3]. In addition, cases of pemphigus foliaceus mimicking erythema annulare centrifugum have been referred to as ‘erythema annulare–like acantholytic disease’ (EAAD). These typically show subcorneal acantholysis or eosinophilic spongiosis without neutrophilia, with a clinical picture lacking pustules [10]. More recently, a unique case with annular pustular lesions was reported, but without neutrophilic infiltration, unlike our case [11]. These unusual and overlapping manifestations highlight the need for detailed histopathological and immunological evaluation in suspected cases to facilitate correct diagnosis and appropriate care.
Traditional PF treatment includes corticosteroids and immunosuppressants like MMF, azathioprine, and dapsone. If these are contraindicated or ineffective, rituximab, an anti-CD20 monoclonal antibody, offers an effective alternative by depleting B cells and inducing sustained remission. The mechanism of action of colchicine in the management of pemphigus, particularly its neutrophilic variants, involves concentrating in neutrophils, inhibiting mobility, adhesiveness, and chemotaxis, likely counteracting IL-8–mediated neutrophilic infiltration [8, 12]. Our patient responded well to rituximab, highlighting its role in refractory cases and emphasizing the utility of colchicine as a preferred maintenance drug.
CONCLUSIONS
This case reinforces the necessity of considering annular neutrophilic pemphigus foliaceous in the differential diagnosis of annular, pustular skin eruptions, underscoring the effectiveness of rituximab as a safe therapeutic option, particularly in cases where conventional immunosuppressants pose unacceptable risks.










