
Rheumatoid neutrophilic dermatosis (RND) is a rare and severe cutaneous manifestation in patients with rheumatoid arthritis (RA) [1]. The skin lesions typically present as red papules, plaques, nodules, or urticaria-like wheals, while ulcers and ecchymoses are rare [2]. The TNF-α inhibitor infliximab has been reported to be efficacious in the treatment of bullous RND [3]. Here, we describe the case of RND characterized by multiple ulcers and ecchymoses that substantially improved following treatment with adalimumab.
A 73-year-old female developed pruritic erythema and nodules on her lower limbs 1 month ago. The patient had previously been diagnosed with “eczema” and treated with oral antihistamines and topical corticosteroids, which showed no significant improvement. Within 2 weeks, the erythema and nodules progressed to ulcers along with pain. The patient had a 13-year history of RA managed with long-term leflunomide therapy. Her other medical comorbidities included interstitial lung disease, hypertension, corticosteroid-induced diabetes mellitus, and severe osteoporosis with a recurrent joint replacement history. Physical examination revealed multiple ulcers and ecchymoses on both lower extremities (Figures 1 A–C). Scattered hemorrhagic lesions were observed on the soles of both feet (Figure 1 D). Laboratory investigations revealed significant inflammatory activity, characterized by elevated C-reactive protein (CRP) at 29.3 mg/l, increased erythrocyte sedimentation rate (ESR) of 114 mm/h, and high-titre rheumatoid factor positivity (288 IU/ml). The pathogen examination results were all negative. Histopathologic examination of the lesion on the left calf showed prominent neutrophilic infiltration throughout the dermis without evidence of vasculitis changes (Figure 2). Direct immunofluorescence showed no deposits of IgG, IgA, IgM, or C3. A diagnosis of RND was made. Considering the history of osteoporosis and steroid-induced diabetes, systemic corticosteroids were not applied. The patient received combination therapy with subcutaneous adalimumab (40 mg weekly) and oral leflunomide (20 mg daily). After 3 weeks of treatment, skin lesions showed significant improvement. Ulcers in the lower limbs gradually heal with newly formed granulation tissue (Figures 1 E–H). In the follow-up stage, the inflammatory markers (CRP, ESR, and RF) exhibited a decline as well.
Figure 1
Skin lesions of the patient. A–C – Multiple ulcers and ecchymoses on both lower extremities. D – Scattered hemorrhagic lesions on the soles. E–H – Clinical manifestation before and after treatment with adalimumab
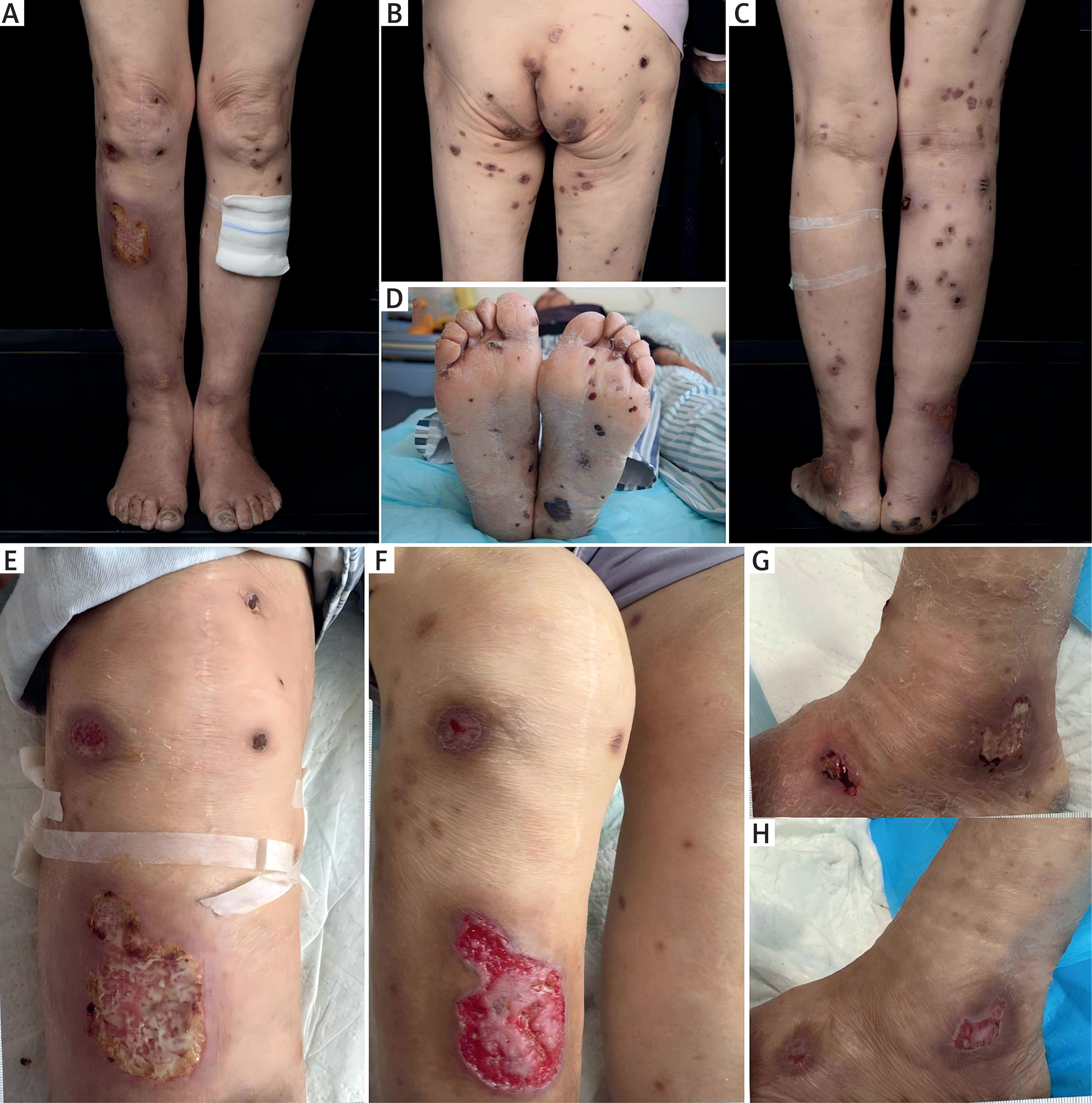
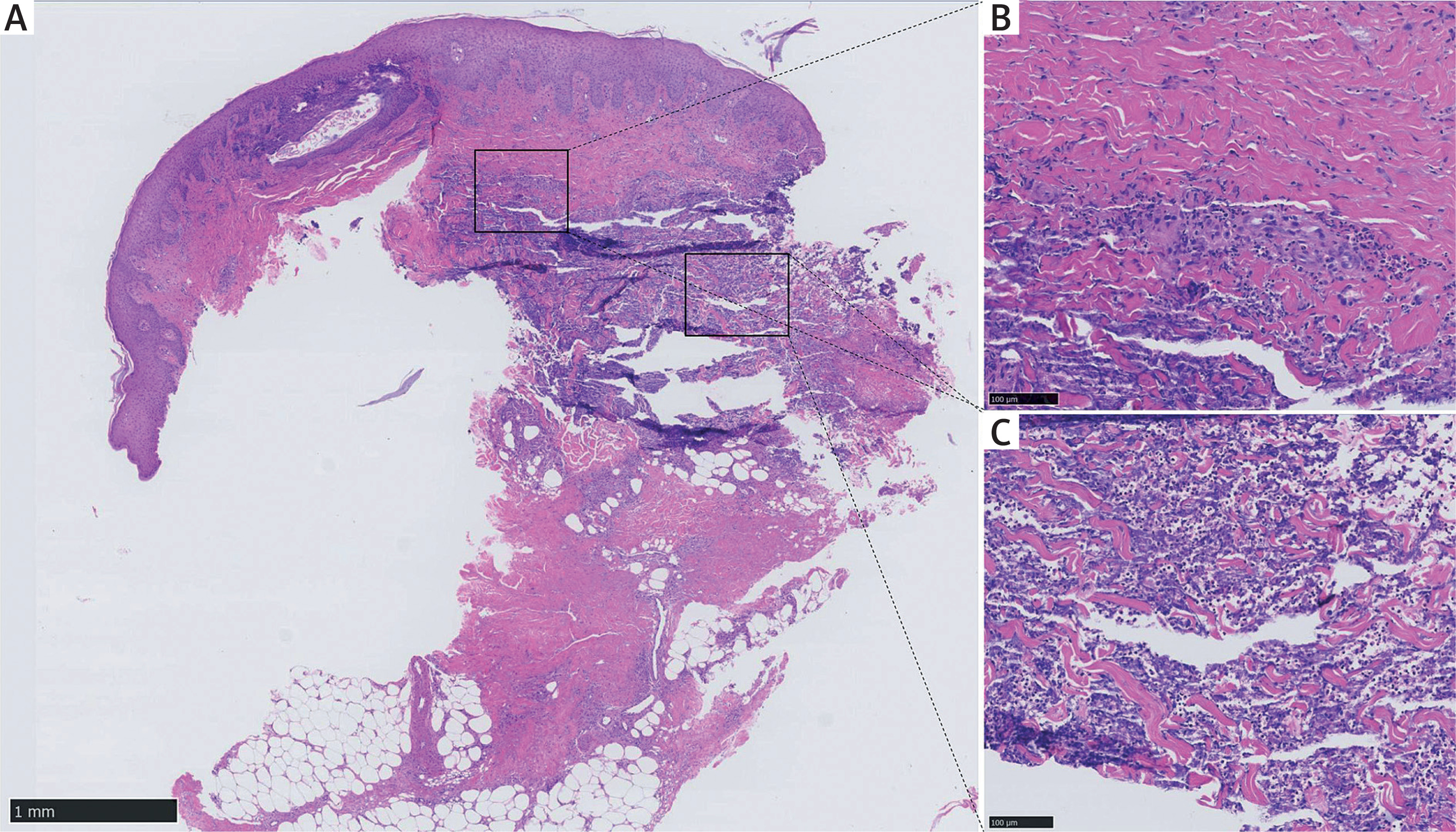
Figure 2
Infiltration of neutrophils is seen between collagen fibres in the dermis without vasculitis change
RND typically occurs in patients with severe RA disease activity, underscoring its prognostic value [4]. Hemorrhagic lesions in RND are rare, especially in patients with ulcers. Our patient had a long history of RA with elevated inflammatory marker levels, likely reflecting heightened RA disease activity. Histopathologically, RND demonstrates dense dermal neutrophilic infiltrates with leukocytoclasis but lacks true vasculitis features [4]. The differential diagnosis for RND includes pyoderma gangrenosum, Sweet’s syndrome, and rheumatoid vasculitis [4]. Most RND patients exhibit high-titre rheumatoid factor positivity [4]. Therefore, the recognition of clinicopathological features is critical for both accurate diagnosis and RA disease activity assessment.
Standardized treatment recommendations for RND have not yet been established. Some patients might experience spontaneous resolution of skin lesions with the improvement of RA [4]. Treatment of RND includes systemic and topical corticosteroids, immunosuppressants like hydroxychloroquine and cyclosporine, as well as anti-neutrophil agents like dapsone and colchicine [4]. Notably, successful treatment with etanercept has been reported in RND patients with vesiculobullous lesions [3]. TNF-α inhibitors are biological agents for RA, effectively alleviating patients’ symptoms and enhancing their quality of life [5]. RA patients exhibit elevated levels of circulating inflammatory cytokines, including TNF-α, which facilitates neutrophil migration and could be blocked by adalimumab [6]. Neutrophils release TNF-α at the early stage of inflammation [7]. Although not the main source of TNF-α, highly infiltrated neutrophils in skin lesions might be therapeutic targets of TNF-α inhibitors. Additionally, TNF-α markedly induces the formation of neutrophil extracellular traps (NETs) in RA, serving as crucial factors in initiating and sustaining inflammation [8, 9]. Therefore, TNF-α inhibitors, such as adalimumab, might alleviate inflammation in RND patients by suppressing neutrophil migration and NETs formation as well. To the best of our knowledge, this is the first reported case of RND treated with adalimumab. Our patient showed a good response to adalimumab therapy, fully demonstrating its therapeutic value. However, this evolution might be independent of adalimumab use, as RND can improve spontaneously with the alleviation of RA. On the other hand, RA patients receiving TNF-α treatment might experience exacerbation of rheumatoid nodules or granulomatous inflammation, mostly induced by etanercept [2, 10, 11]. The underlying pathogenesis remains unclear. Nevertheless, TNF-α treatment could be considered as an effective option in RND patients and requires long-term follow-up.







