








Introduction
Inguinal hernia is the most prevalent type of abdominal wall hernia, and its repair is a highly common procedure, ranging from 10 to 28 operations per 100 000 inhabitants [1, 2]. Its ubiquity has led to a quick and constant improvement in surgical technique to improve postoperative outcomes. Mesh fixation of hernias has become the gold-standard treatment after showing significantly lower recurrence rates and overall better outcomes than non-mesh repairs [3, 4]. While both laparoscopic and open repairs have proven reliable procedures, laparoscopic approaches are becoming more popular due to less postoperative pain and earlier recovery compared to open repair as proven by various studies [5–7]. In open procedures the mesh can be easily fixed via sutures, but in laparoscopy, although feasible, suturing is more difficult and such alternative methods for mesh fixation have been described. Staples, tacks or glue are used to fix the mesh with ease, thus reducing operative time. However, tacking techniques are associated with important complications such as chronic pain [8, 9], hematoma formation [10], severe bleeding (inferior epigastric pedicle injury) [11] or bowel fistula [11]. To overcome the risk of chronic complications due to tack entrapment absorbable tacks have been designed which fix the mesh only until it is integrated by the host tissue, after which fixation should no longer be required [12].
A recent systematic review and meta-analysis, analysing three randomized controlled trials and two observational studies, showed similar outcomes between absorbable and permanent tacks [13]. Thus, the more expensive absorbable tacks are not yet justified. Another recent alternative for mesh fixation is the use of cyanoacrylate glue, which is already used with success on skin grafts [14] and vascular anastomosis [15]. Glue is a non-penetrating technique for mesh fixation and risks of nerve, vessel or muscle injury should be eliminated, reducing postoperative pain and improving patient satisfaction. However, some would argue that it is not as capable as tacks in anchoring the mesh in the preperitoneal plane.
Aim
Herein we aimed to analyse the intraoperative mesh fixation success rate and postoperative outcomes between cyanoacrylate glue versus absorbable tacks in laparoscopic transabdominal preperitoneal inguinal hernia mesh repairs.
Material and methods
Design and setting
This is a prospective comparative study conducted at Naas General Hospital, Ireland on patients who underwent laparoscopic transabdominal preperitoneal (TAPP) inguinal hernia repair between 2018 to 2020. Prospective survey methodology was used to compare the feasibility of mesh fixation and postoperative outcomes in two studied groups: cyanoacrylate glue (LiquiBand FIX8, Advanced Medical Solutions, U.K., LB) and absorbable tacks (5 mm, violet absorbable tacks, AbsorbaTack, Covidien, Ireland, AT).
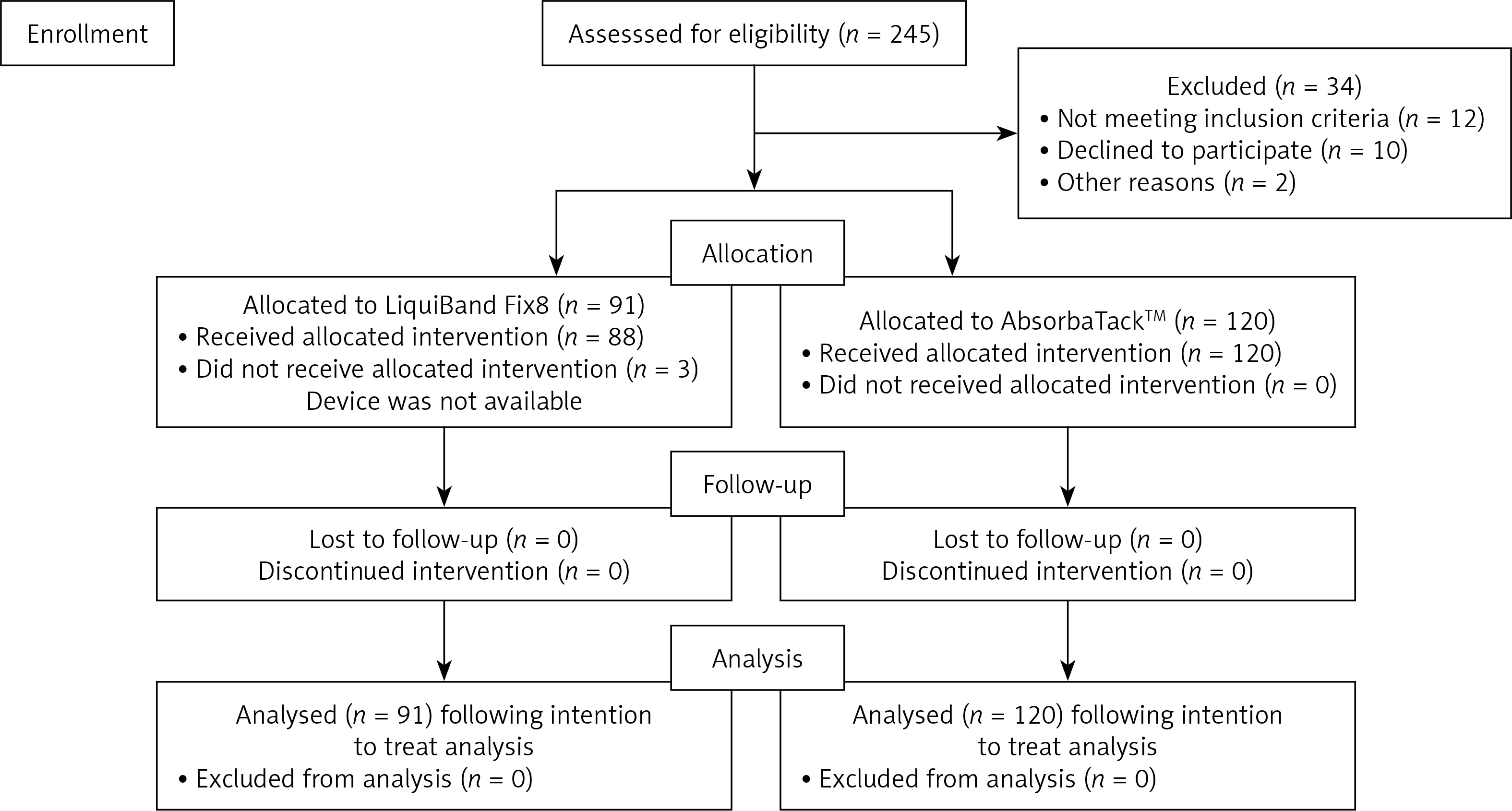
Patients were selected in a non-randomized way to one of the two treatment arms, the study group (LB) or the control group (AT), at a 1 : 1 ratio. The CONSORT flow was followed throughout the study (Figure 1). A single repair technique (TAPP) was performed for all patients to maintain homogeneity and keep appropriate distribution between the study and control devices. The decision to use LB or AT was made based on preoperative patient preference (the patient was informed about the method, advantages and disadvantages of each device) or intraoperative surgeon preference. Once the preperitoneal flap was dissected, if there was significant oozing, then AT were used as LB does not efficiently adhere to a wet surface and the risk of clogging the tip is increased. After reviewing the available classifications for groin hernias, the authors selected the European Hernia Society (EHS) [16] as a method for intraoperative classification and description.
Inclusion criteria
We included all adult patients diagnosed with unilateral/bilateral groin hernia who were candidates for TAPP repair and willing to be part of the study. We analysed both elective and emergency repairs. We included only patients with an American Society of Anaesthesiologists (ASA) grade less than 4.
Exclusion criteria
Patients with recurrent groin hernia or who had previous preperitoneal dissection or pelvic radiotherapy were excluded from the study. Patients with ASA 4 or 5 were excluded. Paediatric cases were also excluded.
Data collection and follow-up
We used a standardized operative form to describe the type of hernia and type of procedure using the European Hernia Society (EHS) classification [16]. The main operator or assistant filled in the forms on the day of admission and at every outpatient visit. Face to face outpatient visits were scheduled at 6 weeks, 6 months and 1 year postoperatively. At 2 years postoperatively, satisfaction scores and recurrence rates were evaluated virtually (i.e., phone call). The exact follow-up date varied within 1–2 weeks depending on clinic slot availability, bank holidays, etc. Patients had direct access to the unit’s secretary and were instructed to call if they had concerns and could book in for urgent outpatient visits if required. These forms were transferred to an electronic database by junior surgeons and included: patient demographics, medical history (surgical, cardiovascular, respiratory and metabolic risk factors or comorbidities), ASA grade, hernia type, procedure type, early postoperative complications (e.g., hematoma, seroma, surgical site infection) and patient reported outcomes. The patients’ name and medical record number (MRN) were coded during data collection and analysis. The immediate and early post-operative pain was assessed by reviewing patients before discharge and at 6 weeks postoperatively. The Visual Rating Scale (VRS) was used to assess level of pain. Patients were asked to scale their pain from one (least) to ten (unbearable pain) and then the pain was classified as being mild (pain score 1–3), moderate (pain score 4–5) or severe (6–10). Postoperative pain was defined as acute if it persisted up to 6 weeks postoperatively or chronic if it persisted after this. Only acute pain was analysed based on severity, while chronic pain was evaluated only through its presence. Surgical complications were defined as early if they occurred in the first 6 weeks postoperatively and late after this date. Patient satisfaction and quality of life were assessed via the Patient Reported Outcome Measures (PROMs) questionnaire (Table I) and by using the Likert scale to provide quantitative data, which were further analysed via χ2 and Mann-Whitney tests (Table II).
Table I
Patient reported outcomes after hernia repair
| Variable | PROME score 10–12 Acceptable | PROME score 13–15 Good | P-value | ||
|---|---|---|---|---|---|
| Fixation | AT | 56 | 64 | 120 | 0.146 |
| LB | 35 | 56 | 91 | ||
| Total | 91 | 120 | 211 | ||
Surgical technique
All procedures were day cases, performed under general anaesthesia, by using a laparoscopic TAPP as previously reported [17]. The mesh fixation method was either using LB or AT based on the patient preference and intraoperative, pre-fixation, surgeon preference. Once allocated to a group, fixation was declared successful if done via the assigned method, regardless of the number of devices used. If after allocation to one of the two fixation methods the surgeon would change the method (e.g., initially allocated to glue, but then the surgeon would opt for sutures or tacks), then that fixation would be assigned to mesh fixation failure. If the surgeon required another similar device, because the first one had technical issues, but did not change the method of fixation, then that case would be assigned to the device failure rate but would not be regarded as a mesh fixation failure.
After preperitoneal dissection and reduction of the hernia sac, it is our routine practice to dry the preperitoneal space with a dental gauze swab. This facilitates optimal application of the glue by preventing tip clogging of the device through backflow of blood or fluid.
A 10 × 15 cm DynaMesh-ENDOLAP 3D was used in all cases. We used medial to lateral fixation of the mesh at five anchoring points: starting medially (i.e., 9 o’clock for a right sided repair) at the pubic tubercle, then at 12 o’clock and 6 o’clock (superior and inferior border of the mesh) and then lateral to the inferior epigastric vessels, at two points (i.e., for a right sided hernia at 2 and 4 o’clock). From our experience, the glue can be applied on the triangle of doom and triangle of pain without significant intraoperative and postoperative adverse events. When applying the glue, it is important to stabilise the mesh against the abdominal wall using a grasper (e.g., Yohan grasper) in the non-dominant hand. We closed the peritoneum using V-Loc sutures instead of glue or tacks. This is more cost-effective and avoids using another LB device for a single hernia repair. Also, the risk of tack related complications is reduced [18]. For the control group (AT), the mesh was fixed via three anchoring points: one medially at the pubic tubercle and another two, one medial to the epigastric vessels and one lateral to it. We always make sure to have a clear view of the musculoaponeurotic layer when applying the tacks. The rest of the procedure followed similar steps to the study group.
Results
Fixation success rate
A total of 211 patients were included in the study, divided into two groups: the study group, in which LB was used to fix the mesh (n = 91) and the control group, in which AT was used (n = 120). The vast majority of hernias were primary (96.7%, n = 88, in LB groups versus 95%, n = 114, in the AT group). Both groups were comparable in terms of type and size of the hernia (Table III). The median follow-up period was 28 months (range: 15–42) for LB and 22 months (range: 6–32) for the AT.
Table III
Preoperative classification of hernias by occurrence, type and size
[i] EHS – European Hernia Society, LB – LiquiBand group, AT – absorbable tacks group, F1 – femoral hernia less than 1.5 cm, F2 – femoral hernia between 2–3 cm, F3 – femoral hernia more than 3 cm, L1 – lateral hernia less than 1.5 cm, L2 – lateral hernia between 2–3 cm, L3 – lateral hernia more than 3 cm, M1 – medial hernia less than 1.5 cm, M2 – medial hernia between 2–3 cm, M3 – medial hernia more than 3 cm.
The mesh fixation success rate when using LB was 96.70% (n = 88). The device failure rate in LB was 6.6% (n = 6). In all 6 cases, the LB device had to be changed due to clogging. A single LB device was required for complete mesh fixation in 93.40% (n = 85) of cases. In the AT group, the mesh fixation success rate was 100% (n = 120). The device failure rate was 1.66% (n = 2), in which an alternative AT device was required to complete fixation (Table II).
Acute pain
Acute pain was classified into mild, moderate and severe. 83.51% (n = 76) of patients in the LB group experienced mild pain. No patients in the LB group reported pain scores higher than 5, based on the VRS scale. In the AT group, 96.6% (n = 116) of patients reported mild pain and 3.3% (n = 4) had a pain score higher than 5. When analysed via the chi square test, patients in the AT group had significantly higher pain scores than patients in the LB group (p < 0.001, 95% CI) (Table IV).
Chronic pain
There was no statistically significant difference in chronic pain between the two groups (p = 0.479, 95% CI). 2.19% (n = 2) of patients experienced chronic pain in the LB group versus 3.3% (n = 4) in the AT group (Table V).
Patient reported outcomes
The patients were evaluated using the PROMs questionnaire at their clinic follow-up, up to 1 year after the surgery (the minimum follow-up period was 6 months). The 2-year follow-up rate was 70% (n = 148) in our cohort (median: 29 months, range: 14–40). There was no significant difference in patient reported outcomes between the two groups (Table I).
Recurrence rate and complications
There was 1 case of hernia recurrence in the LB group (recurrence rate = 0.4%) and no recurrences in the AT group (recurrence rate = 0%). A single case of recurrence was diagnosed in the LB group, which was detected at 5 months postoperatively when the patient requested a visit due to concerns of recurrence. The initial hernia was a medial one (direct) with a size of 3.2 cm. This case was reoperated on via a TAPP approach; the old mesh was left in situ, laterally migrated, and a new, similar mesh was fixed onto the myopectineal orifice via absorbable tacks placed at the pubic tubercle and the superior quadrants. Other procedure related complications were recorded by the surgical team during follow-up and, for both groups, included seroma 2.4% (n = 6), port site bleeding 0.3% (n = 2), and port site hernia 0.3% (n = 2) (Table VI).
Discussion
Our results show that mesh fixation with cyanoacrylate glue is associated with less pain in the early postoperative period and with similar chronic pain, patient reported outcomes and recurrence rates compared to mesh fixation with absorbable tacks. These results corroborate earlier studies [19, 20] which showed that glue is a quick, non-traumatic method to safely fix the mesh, reducing postoperative pain, without increasing failure or recurrence rates. N-butyl-2-cyanoacrylate is a tissue adhesive widely used for skin incisions. Its initial liquid form makes it easy to apply and the subsequent quick polymerization into a solid, waterproof adhesive enables secure tissue fixation.
When using glue, it is highly important to ensure the operative field is dry, otherwise in our experience the glue will not adhere, or the tip of the device will clog in contact with fluids. This was the reason for the three failures in the LB group. Thus, one should dry the operative field before using the LB device or use another fixation method from the start. In our study there were six failure cases in the AT group. In these cases, the tacks did not reach the fascia due to thickened preperitoneal fat. To tackle this, one must ensure that there is a clear view of the musculoaponeurotic layer when firing tacks or using glue, as we did in these 6 cases with success. While adopting TAPP repair by an inexperienced surgeon demands at least 50 cases to become proficient [21], using glue for fixation does not require a learning curve apart from a simple preoperative technical overview as the repair technique remains roughly similar to the original TAPP. All procedures in this study were performed by surgeons experienced in TAPP repairs.
Application of n-butyl-2-cyanoacrylate is less traumatic than sutures or tacks and, in our experience, can be safely applied on both the triangle of doom and triangle of pain when performing TAPP hernia repairs. Indeed, sutures and tacks provide better mechanical support in the first 14 days, but in the medium and long-term follow-up, meshes fixed with tissue adhesives show similar integration and durability as shown in a previous pre-clinical study [22]. What matters probably more than the method of fixation is the size of mesh used. As previously proven, it is imperative to use a minimal size of 10.4 × 13.2 cm in order to cover the entire myopectineal orifice in hernias less than 3 cm and 13 × 15.6 cm in hernias more than 3 cm [23]. Herein we preferred a 10 × 15 cm mesh, which intraoperatively seemed appropriate for all hernias in this study. We found a single recurrence after 2 years of follow-up in a 3.2 cm direct hernia. It is difficult to predict whether this was a case of fixation failure causing lateral migration of the mesh or inappropriate mesh size.
Pain is probably the most well-known complaint surgeons face postoperatively, and given that nerve entrapment is an important cause of it a plethora of studies have proposed less and less invasive fixation methods. Even more, a growing body of evidence has shown that applying the mesh without any fixation is feasible, decreasing postoperative pain without increasing recurrence rates [24, 25]. Despite this, to avoid migration, the vast majority of surgeons are more comfortable when fixing the mesh. Glue is a proven balanced option offering the best of both worlds: reliable fixation without the use of foreign bodies that could cause entrapment and subsequent postoperative pain [26].
A recent randomized controlled trial published by Mohammadi Tofigh et al. [27] comparing sutures versus N-hexyl cyanoacrylate in 58 patients with inguinal hernias who underwent Lichtenstein repair showed reduced operative time and less postoperative pain in the glue group. This is in line with the similar results of an earlier systematic review and meta-analysis on Lichtenstein inguinal hernia repairs using either glue or sutures to fix the mesh [28]. For open procedures, there are enough supporting data favouring n-butyl-2-cyanoacrylate glue for mesh fixation compared to sutures; however, for laparoscopic procedures the evidence is not yet strong. Moreover, studies comparing n-butyl-2-cyanoacrylate to tacks in TAPP procedures are scarce. To our knowledge two studies [29, 30] have compared n-butyl-2-cyanoacrylate to tacks in laparoscopic hernia repair, but in both studies repair was done in a total extra-peritoneal fashion (TEP). Both studies showed that n-butyl-2-cyanoacrylate is similar to tacks in terms of mesh fixation, chronic pain and risk of recurrence. Yu et al. [30] noted less acute pain in the n-butyl-2-cyanoacrylate group and similar chronic pain compared to tacks. In our study all procedures were TAPP, and the results are consistent with the aforementioned studies. More commonly fibrin glue was used, and a meta-analysis published in 2013 by Sajid et al. [31] showed that fibrin glue fixation is associated with less pain and similar recurrences compared to tacks. Another meta-analysis published by Antoniou et al. [32] reached a similar conclusion.
Traditionally, studies have compared different repair techniques in the light of surgical complications such as wound infection, chronic pain and recurrence, but it is now accepted and recommended that functional outcomes, patient satisfaction and quality of life are considered when adopting new approaches [33, 34]. Herein we used the previously reported PROMs [17], which are split into five main questions with regards to pain, mobility, self-care at home, daily activities and satisfaction. Each question is scored with 1, 2 or 3 points based on the answer given, summing up to a maximum grade of 15. Indeed, there is still significant variability in how authors quantify patient reported outcomes. The lack of standardization needs to be addressed. This has been highlighted by Wilcox et al. [35] and it is something we need to change also in future publications.
There are a number of limitations of the study. Randomization of patients was not possible due to logistical reasons in our unit; thus the decision to use LB or AT was based on patient preference or at the surgeons’ discretion. Whenever there was a damp dissection plane, we preferred to use AT. Also, once the medial and lateral inguinal fossae were dissected, if the fascial plane was not clearly visible (e.g., in patients with increased preperitoneal fat pad) we preferred to use LB, rather than risking firing tacks into loose preperitoneal fat. We chose not to analyse the operative time as it would not affect the rate of postoperative pain and recurrence. Reduction of operative time when using tissue adhesives is widely proven already. This study aimed to analyse the feasibility and safeness in using LB to fix the mesh in the preperitoneal space with special regards to the incidence of postoperative pain and recurrence compared to the control group in which AT was used.