
Dear Editor,
Oliguria in the setting of critically ill patients is usually treated by admini-stering fluids and furosemide [1]. Invasive therapies, namely renal replacement therapies (RRT), are reserved for patients in whom less invasive measures have failed [2], especially if acute pulmonary oedema complicates the clinical picture [1].
Intravascular volume depletion elicits a kidney response consisting of augmented sodium retention at Henle’s loop and water at the collecting tubules. In such conditions, loop diuretics such as furosemide would be less effective to improve diuresis and water loss than osmotic diuretics such as mannitol [3, 4].
This case report aims to highlight the utility of the assessment of the glomerular and tubular functions to identify an ineffective diuretic strategy and to select a successful one, which prevented the use of invasive RRT.
A 33-year-old female patient suffering from preeclampsia (gestational age was 35 + 6 weeks) was admitted to our Post-surgical Intensive Care Unit (PICU) after an urgent caesarean section performed under spinal anaesthesia, without further incidents.
At admission to the PICU, the patient was oedematous and presented with hyperreflexia and mild hypertension (150/90 mm Hg). The laboratory tests showed a slight elevation in transaminase levels (AST: 48 U L–1; LDH: 492 U L–1), mild anaemia (haemoglobin: 10.3 g dL–1; haematocrit: 28.9%) with moderate thrombocytopenia (101 G L-1) and signs of mild metabolic acidosis (pH: 7.34; bicarbo-nate: 14.9 mmol L–1; base excess: –9.7 mmol L–1; pCO2: 28 mm Hg) which was attributed to mild dehydration, even though blood loss during the surgery had not been excessive (approximately 800 mL).
Initially, the renal function was not considered to be impaired since urine output was higher than 1 mL kg–1 h–1, and many other serum biomarkers fell within normal limits (creatinine 0.59 mg dL–1; urea 47 mg dL–1; sodium 134 mmol L–1; potassium 3.7 mmol L–1; chloride: 104 mmol L–1). However, oliguria (urine output < 0.5 mL kg–1 h–1) complicated the clinical picture during the first 24 hours of admission. Neither initial fluid overload (3500 mL of crystalloids: 1500 mL of normal saline and 2000 mL of Ringer lactate solution) nor furosemide boluses (20 mg IV every 8 h) restored urine output.
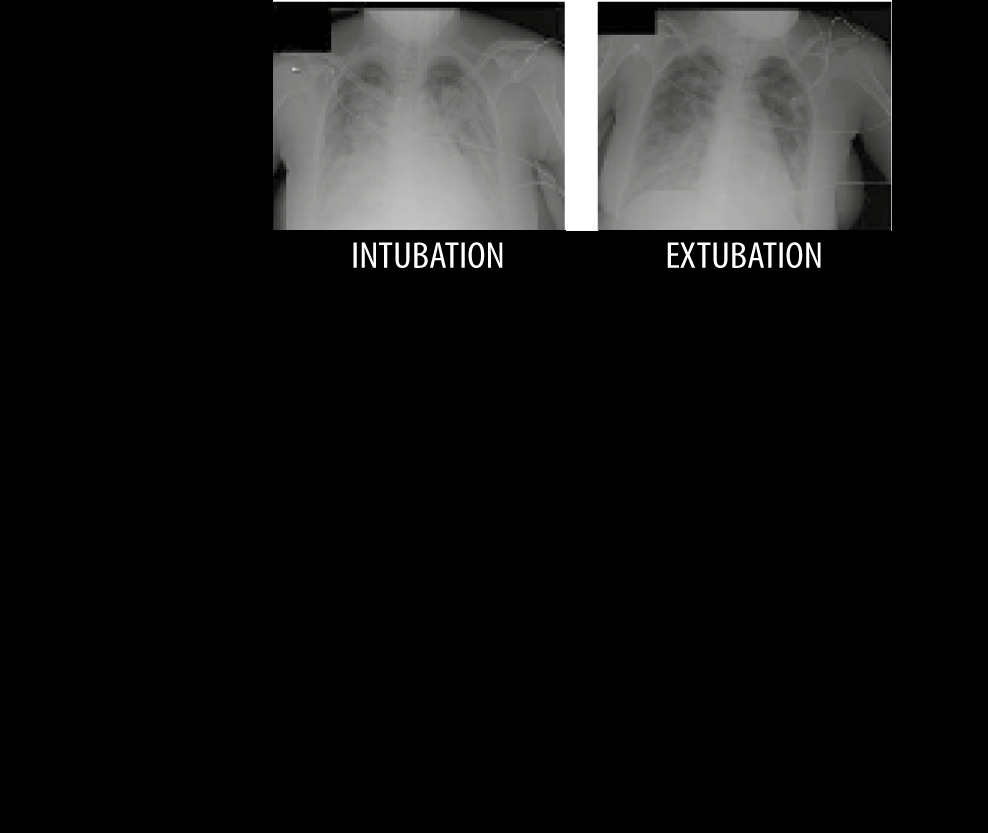
Furthermore, accumulated hydric balance was positive (+ 4 L) in spite of the fluid restriction (saline infusion of only 10 mL h–1) and increase of the dosage of the loop diuretic (continuous infusion of furosemide at a rate of 5 mg h–1). The clinical picture was progressively aggravated by respiratory insufficiency due to acute pulmonary oedema, and invasive mechanical ventilation was required a few hours later (Figure 1). Hemodynamic status remained stable.
FIGURE 1
Daily and accumulated evolution of hydric balance and radiological findings at the time the patient was intubated and extubated
Then, the key issue was to increase the elimination of body fluids, yet the main doubt was how to achieve it; the alternatives considered at this point were either increasing the dosage of furosemide or starting RRT.
However, before any therapeutic decision was taken, the patient’s relatives asked for a change in the medical team. Instead of applying any of those alternatives, the physicians now in charge decided to perform kidney function tests to try to diagnose the cause of oliguria, as the result of such a test would be useful to guide the therapeutic decision. Creatinine clearance showed mild renal insufficiency (CrCl: 74 mL min-1); the fractional excretion of sodium was very low in spite of the natriuretic treatment with furosemide (FeNa: 0.4 %); and free water clearance was negative (ClH2O: –0.6 mL min-1), indicating water reabsorption (Figure 2).
FIGURE 2
Time evolution of diuresis, administered diuretics, and results of the studies of the glomerular and tubular function
Based on the above results, the natriuretic furosemide was deemed ineffective, and it was stopped. If the glomerular function had been so impaired that there would be reasonable doubt about the capacity to filter mannitol, the excess of fluid would have been removed by starting RRT. However, after considering that the glomerular function was preserved enough to filter mannitol, the use of RRT was delayed to give the osmotic diuretic a chance. The administration of the first bolus of 20% mannitol (100 mL) was followed by an increase in urine output (1 mL kg–1 h–1), allowing for a negative fluid balance to be achieved that day (–2000 mL) (Figure 1).
Kidney tests were reassessed 24 hours later. Results for both glomerular (CrCl: 73 mL min-1) and tubular (FeNa: 0.4%) functions remained stable but, interestingly, free water clearance had turned positive (ClH2O: +0.4 mL min–1) (Figure 2). A second bolus of 20% mannitol (50 mL) was again followed by an increase in urine output and negative fluid balance. X-ray findings and ventilatory requirements also improved, making weaning from mechanical ventilation possible (Figure 1).
From then on, the clinical evolution was uneventful, and the patient was discharged from the PICU. After discharge, the patient and her relatives granted us permission to send her clinical case for publication.
The case reported exemplifies the usefulness of assessing the glomerular and tubular status in haemodynamically stable critically ill patients in order to select an effective therapeutic strategy to manage volume overload. The authors are fully aware that the initial aggressive fluid administration could be controversial [5]; nevertheless, unequivocal recommendations on fluid management in pre-eclampsia are lacking [6] and, additionally, discussion about fluid management in pre-eclampsia falls outside the scope of this report.
Regarding diagnostic procedures for suspected renal failure, nephrology guidelines recommend assessing both glomerular and tubular function by measuring CrCl, FeNa, and ClH2O [7]. Critical care guidelines also recommend assessing glomerular function, but diagnostic recommendations concerning tubular function are lacking [8].
Spanish critical care guidelines focusing on the treatment of volume overload recommend first using furosemide and, in the event that it fails, RRT [8]. In our case, RRT would have undoubtedly been as effective as mannitol to achieve a negative fluid balance, but at the price of eventually exposing the patient to a risk of greater morbidity [9] and, obviously, at a higher direct economic cost [10]. The acquisition of a bottle of 250 mL of 20% mannitol costs €1.00 for our hospital, whereas just the material needed to start with continuous venovenous haemodialysis, which only includes the catheter, the extracorporeal circuit and the first dialysate solution bag, would cost €137.58. Therefore, complete treatment with mannitol would be far less expensive (less than €1.00) than a single day on RRT, which would fall in the range of hundreds of euros [10].
Instead of following the therapeutic recommendation offered by critical care guidelines, we decided to follow the diagnostic approach recommended by nephrology guidelines [2]. FeNa was found to be low in spite of furosemide, maybe because the tubular reabsorption of sodium was increased as a physiological response to volume depletion. In such scenarios, osmotic diuretics could be a better alternative than natriuretics to force urine output [3].
Mannitol boluses are routinely used to enhance urine output in some neurosurgical procedures requiring a reduction of intracranial pressure [11]. Mannitol has also been successfully used in intensive care setting for the treatment of clinical conditions presenting with excessive lung water, such as distress or acute pulmonary oedema [4]. However, it should be used with caution in patients presenting with oliguria. Specifically, kidney tests should be conducted to confirm that glomerular function is preserved since mannitol must be filtered to exert its intraluminal osmotic effect; such assessment should be mandatory if renal impairment is suspected, as mannitol by itself can aggravate a preexisting renal injury [11] and even cause pulmonary oedema [12]. Our patient presented with mild renal insufficiency, but the capability of the glomeruli to filter mannitol was judged to be preserved enough [13]. Thus, small daily boluses (20 g, and 10 g) similar to those used in neurosurgical procedures [11] were judiciously administered. As a result, urine output increased, the fluid balance turned negative, and both pulmonary oedema and respiratory insufficiency were ameliorated. This explanation has been agreed on by other authors who also used mannitol to successfully treat acute pulmonary oedema in preclinical and clinical settings [14, 15].
The main strength of the case reported lies in a thorough assessment of the renal function. The results obtained helped us to select what we considered the most efficient alternative (mannitol instead of RRT), even though our diagnostic approach and the further therapeutic decision were not supported by current critical care guidelines [2, 7, 8]. The study of renal function is not recommended even in reviews focused on the management of oliguria in pre-eclampsia [5]. Precisely, this lack of support from such guidelines could be considered as the main limitation.
After taking all the above into consideration, the assessment of the glomerular and tubular function in critical care patients suffering from oliguria and fluid disbalance seems to be helpful to guide therapeutic decisions; such assessment is a non-invasive procedure, it can be easily and rapidly performed, and it has the potential for being cost-effective.