
Introduction
The discovery of acetylsalicylic acid in 1897 opened a new era for the use of non-steroids anti-inflammatory drugs (NSAIDs) [1]. Already a few years after the discovery of the drug, the first cases of hypersensitivity were described [2, 3]. The widespread use of NSAIDs increases the incidence of hypersensitivity to the drug, which in the general population may reach 0.3–0.5% [4]. In the adult population with diagnosed bronchial asthma hypersensitivity to aspirin (ASA) it may even amount to 21% [4, 5]. The enormous scale of the problem gives rise to verification of the symptoms reported by patients. For this purpose drug provocation tests are used, and in this work oral aspirin challenge (OAC) was used.
The OAC is considered the gold standard in the diagnosis of hypersensitivity to NSAIDs [6]. It has the highest sensitivity and specificity, but due to higher cumulative doses, high exposure to the drug of all effector organs (such as the respiratory system, skin, mucous membranes, digestive system or circulatory system) and no possibility of disruption (long absorption time by the gastrointestinal tract), it may have many adverse effects [7]. During the test, special attention is paid to the clinical symptoms of hypersensitivity especially from the skin and respiratory system. Objective monitoring of ventilation disorders with the use of a spirometer was carried out. On the other hand, circulatory functions are not routinely monitored, apart from blood pressure measurements in the search for hypotension as a result of severe anaphylaxis. Meanwhile, the available literature on the subject presents works describing various reactions of the circulatory system during anaphylaxis, e.g. myocardial infarction as a result of the coronary artery contraction or destabilization of the atherosclerotic plaque, or stent thrombosis under the influence of mediators of the allergic reaction – called Kounis syndrome [8, 9], described in patients with hypersensitivity to hymenoptera venom, hypersensitivity to drugs, including aspirin [10] and ibuprofen [11].
It is also known that histamine, through the receptors in the heart, also affects the cardiac-conduction system [12, 13]. The literature describes studies in which heart disorders were recorded such as atrial fibrillation or ventricular tachycardia during anaphylaxis [14, 15].
Aim
The aim of the study was to assess the incidence and nature of cardiovascular side effects in patients suspected of being hypersensitive to ASA/NSAIDs and subjected to OAC, their relation with the outcome of the challenge and the safety evaluation of the test.
Material and methods
The study included 52 patients hospitalized in the clinic in 2012–2016 with signs of hypersensitivity to ASA and/or NSAIDs in the form of urticaria and/or angioedema (n = 47), bronchospasm (n = 11), including the mixed form (n = 6) in the history, with normal ECG and spirometry. The OAC was performed a minimum of 7 days after discontinuation of antihistamines, while using a reliever-free diet (without histamine) in a symptoms-free period. The patients qualified for the study were subjected to a 2-day single-blind challenge test with ASA, with simultaneous monitoring of clinical manifestations of ASA hypersensitivity, ventilation and cardiovascular function disorders according to the protocol in Table 1.
Table 1
Test protocol
| Oral aspirin challenge | |
|---|---|
| Day 1 – placebo | Day 2 – ASA |
| Monitoring of clinical symptoms of hypersensitivity | |
| Monitoring of ventilation disorders – FEV1 | |
| BP and ECG monitoring | |
Particular attention was paid to skin and mucous membrane symptoms such as urticaria, angioedema, erythema, pruritus and the respiratory system: dyspnoea, cough, rhinitis, bronchospasm and a decrease in forced expiratory volume in 1 s (FEV1) (AbcMED’s PNEUO NEBTM spirometer). During the entire study (2 days), the cardiovascular system was monitored using 24-hour registration of ECG recording (Holter ECG) with a Reynolds Medical device (US) as well as daily blood pressure monitoring (DBPM) using a BOSO device (Bosch & Sohn, Germany). The provocation test was carried out according to the protocol by Professor Niżankowska (Table 2) [16].
Table 2
Oral aspirin challenge diagram
| Day 1 – placebo | Day 2 – ASA | |
|---|---|---|
| Doses | Dose [mg] | Cumulative dose [mg] |
| 1. Sacchari lactis | 27 | 27 |
| 2. Sacchari lactis | 44 | 71 |
| 3. Sacchari lactis | 117 | 188 |
| 4. Sacchari lactis | 312 | 500 |
| 5. Sacchari lactis | 500 | 1000 |
On the first day, placebo (lactose) was administered orally 5 times every 1.5–2.0 h in identical-looking capsules; on the second day, doses of ASA were increased up to a total dose of 500 mg or in the absence of any reaction – up to a maximum dose of 1000 mg according to Table 2 [16]. The test was discontinued at the time of occurrence of clinical manifestations of hypersensitivity and/or a decrease in FEV1 ≥ 20% of the output value and/or the appearance of hypotension (Table 3). The study was approved by the Military Institute of Medicine Ethics Committee.
Table 3
Criteria for the recognition of oral aspirin challenge as positive
Statistical analysis
In terms of descriptive statistics, percentages, arithmetic averages and standard deviations were calculated. In order to find the significance of differences in cardinality in the groups, the χ2 test was applied, while the comparison of some parameters in individual groups was carried out using the Student’s t test for independent variables, assuming significant differences in p-values at < 0.05. Calculations were performed using the Statistica software (StatSoft Poland Ltd. 2015, medical kit version 3.0).
Results
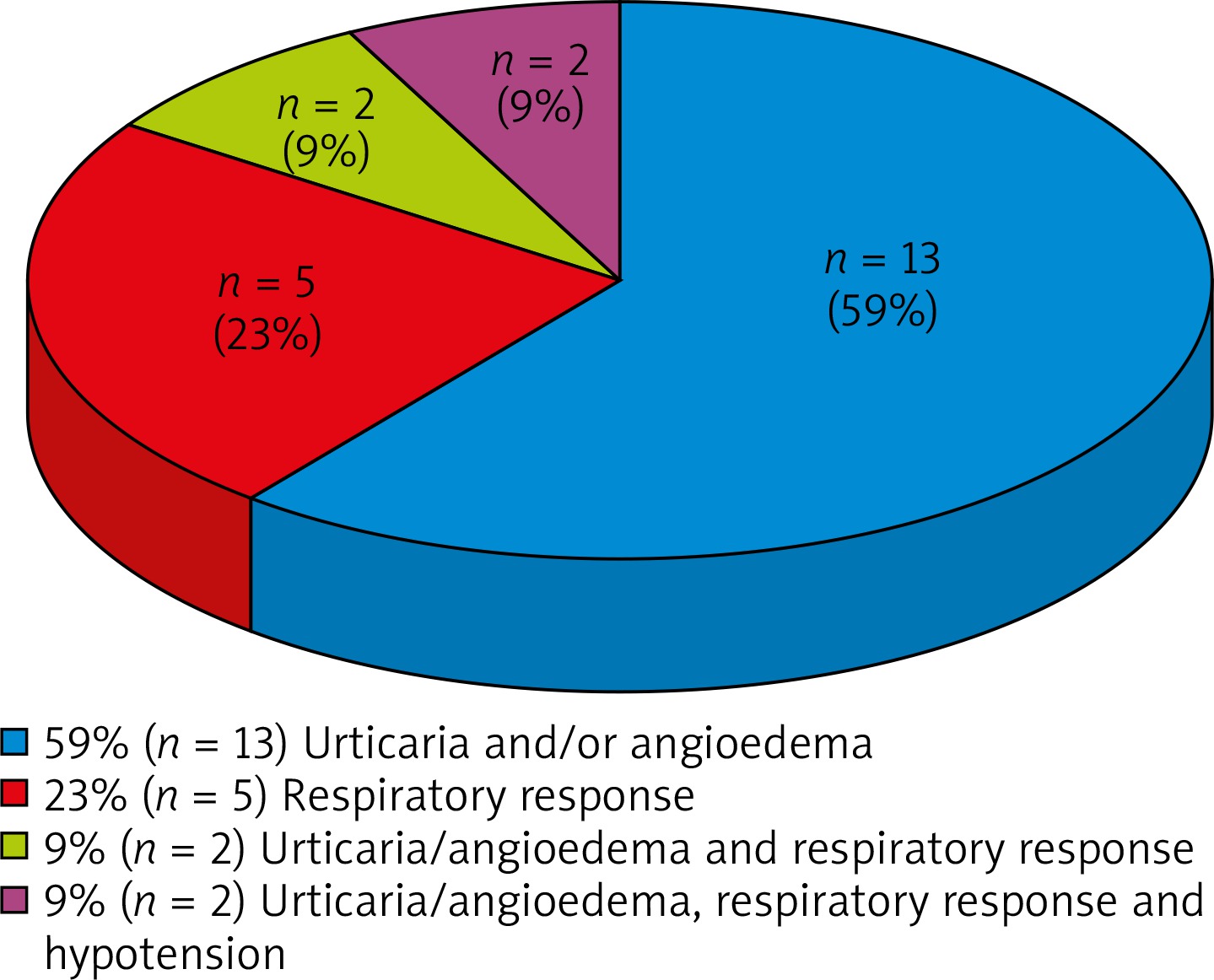
A positive OAC result was obtained in 42% of patients. The most frequently observed clinical manifestation of OAC(+) was cutaneous urticarial-oedema lesions of various severity – 78% (n = 17), including an isolated form ~60% (n = 13), whereas 18% (n = 4) simultaneously manifested urticaria/angioedema and a feeling of chest discomfort or dyspnoea. The isolated obstruction was manifested by 23% of patients (n = 5) (Figure 1).
The most common reaction of the cardiovascular system during OAC was tachycardia (~80% of patients), regardless of the day of the study and the result of OAC. Similarly, supraventricular extrasystoles (SVEx) and ventricular extrasystoles (Vex) occurred with a comparable frequency on both days, regardless of the test result. Both SVT and ventricular tachycardia (VT) were registered in several patients, whereas the disorders occurred both on the day of placebo and ASA administration. In 1 patient, SVT occurred only on the day of ASA administration. The patients did not feel any discomfort and did not require any additional treatment. No severe arrhythmias, i.e. atrial or ventricular fibrillation or flutter were registered. No ischemic heart changes were recorded either (Table 4).
Table 4
Arrhythmia and conduction disorders during oral aspirin challenge
[i] SVex – supraventricular extrasystoles, SVT – supraventricular tachycardia, AF – atrial flutter, AFib – atrial fibrillation, Vex – ventricular extrasystoles, VT – ventricular tachycardia, VF – ventricular flutter, VFib – ventricular fibrillation, AV block – atrioventricular block, OAC(+) – patients with positive oral aspirin challenge results, OAC(–) – patients with a negative oral aspirin challenge results.
Two patients manifested a significant blood pressure decrease, these were the patients with urticaria/angioedema and airway obstruction (Table 5). One of the subjects required typical treatment of anaphylaxis, including adrenaline, while the second one, despite a significant reduction in blood pressure, did not feel any discomfort and did not require any additional intervention.
Table 5
Changes in blood pressure during oral aspirin challenge
| BP | Day 1 – placebo | Day 2 – ASA | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OAC(–) (n = 30) | OAC(+) (n = 22) | All subjects (n = 52) | OAC(–) (n = 30) | OAC(+) (n = 22) | All subjects (n = 52) | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Reduced | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 9 | 2 | 4 |
| Elevated | 4 | 13 | 10 | 45 | 14 | 27 | 3 | 10 | 10 | 45 | 13 | 25 |
[i] Reduced – systolic BP of less than 90 mm Hg and/or rapid BP reduction by ≥ 30 mm Hg from the output value. Elevated – defined as the average value of day and night measurements above 130/80 mm Hg, OAC(+) – patients with a positive oral aspirin challenge, OAC(–) – patients with a negative oral aspirin challenge.
Discussion
The study concluded that in the group of patients with suspected hypersensitivity to NSAIDs in anamnesis, OAC(+) confirms the suspicion in ~42% of patients. Detailed monitoring and analysis of the cardiovascular reaction allow to conclude that, although possible, they are not frequent and despite the theoretical premises, with the currently recommended method of qualifying patients for OAC and the methods of its implementation, do not seem to pose any serious health and life risk to the patients. It is noteworthy, however, that the registered reactions did not always have enough clinical significance for the patients to report them, which would act as a signal to halt the test. Practical conclusions from this last statement must also be cautious, because the presented studies involved a relatively small group of 52 subjects. This stemmed from the necessity to adhere to the recommended OAC protocols (mainly the qualification of patients for the study) as well as simultaneous monitoring of the cardiovascular and respiratory systems, which was not always accepted by the patients. It should be noted, however, that almost all previously published analyses concerning similar problems of running OAC involved similar groups of several dozen patients [17, 18]. For obvious reasons (no indications), for the purpose of the present work, no parallel studies have been planned for the healthy, i.e. the implementation of OAC in patients with a negative history of hypersensitivity to NSAIDs. In the course of OAC, isolated urticaria and/or angioedema occurred most frequently. This concerned almost 25% of patients and 60% of patients with a positive OAC result. This was consistent with the results of virtually all analyses that addressed the problem of the prevalence of hypersensitivity symptoms to NSAIDs [17]. In the studies by Kasper et al. concerning hypersensitivity to ASA in patients with asthma, as also shown in the present study, the most frequently reported form was urticarial oedema, which was found in ~60% of patients, and isolated urticaria was observed only in 33.3% [17].
No studies analysing cardiovascular reactions during OAC were found in the available literature, although, as demonstrated in the introduction, there are theoretical reasons for such reactions. This is mainly due to the currently adopted method of interpretation of the OAC result, which is based on the feedback reported by patients, confirmed later by doctor’s examination, using objective tests such as spirometry performed at selected time points and after reporting symptoms justifying their implementation. ECG is not usually performed routinely, but only when the respondents report pain in their chest area, although then the most expected symptoms are related to the respiratory system and such examination is performed occasionally. Hypotension is one of the extreme manifestations of hypersensitivity. During the controlled administration of ASA, the appearance of first symptoms results in discontinuation of the test and implementation of an appropriate procedure. During the course of OAC, a decrease in BP was registered in 2 patients, while only 1 patient required treatment typical for shock.
It should be emphasized that the patients qualified for the study have not been treated for cardiovascular diseases before, i.e. hypertension, arrhythmia or coronary heart disease, and they have not reported these symptoms, but in some of them, during OAC an increase in blood pressure (BP) values was observed both on the day of placebo and ASA administration; in the group with OAC(+), BP values were significantly higher than in the group with OAC(–). As expected, in the majority of patients with OAC(+), the systolic and diastolic mean values were lower than on the placebo day, but these were not statistically significant changes. Similar results were obtained in the group with OAC(–). It seems that the OAC procedure itself, which assumes the administration of increasing doses of ASA at time intervals, continuous clinical monitoring and early interruption of the test and administering adrenaline, fluids, antihistamines and glucocorticosteroids, depending on the needs, prevented the development of severe hypersensitivity reactions, which could have reduced BP.
Interestingly, there are no cardiac monitoring studies in relation to other provocative tests used in allergology, although it has been known since the 1930s that such a reaction is quite common. The so-called idioblapsis, i.e. a family running IgE-independent response to food, manifested in pulse acceleration was the subject of AF Coca study. In the so-called Coca’s test, which is now of historical importance, acceleration of the heart rate by 10–20 beats per minute after consumption of a specific food was supposed to indicate hypersensitivity to its components [19]. Similarly to the food allergy described by Coca, tachycardia was the expected phenomenon during OAC. However, in my research, it was registered in more than 70% of respondents with no difference to the result of OAC, but both on the day of placebo and ASA administration. At the same time, the mean heart rate in the period of symptoms increased by ~7–11 beats per minute. However, the literature reports cases of atrial fibrillation in patients with an acute allergic reaction, e.g. after an insect bite [20]. Some authors argue that atrial fibrillation episodes can be triggered by allergic reactions that may be caused by an increase in proinflammatory cytokines such as interleukin 6 (IL-6). Other authors explain this with the pro-arrhythmogenic effect of mediators of allergic reactions, especially the effect of histamine on the heart-conduction system [21]. In the current study, the majority of patients suffered from various types of cardiac dysfunctions (up to 90% of subjects) most often in the form of tachycardia, followed by single SVEx and VEx. However, this occurred to a similar degree on the day of placebo administration and on the day of ASA administration. Also, there were no significant differences in this respect between patients with a positive or negative OAC. Similar results were obtained by Malerba et al. They analysed 46 patients in whom coronary artery disease was excluded and no pro-arrhythmogenic drugs were used, with indications for bronchial methacholine challenge, monitoring the occurrence of arrhythmias before, during and after this test [22]. The authors, both in the positive and negative test groups found a similar increase in the number of additional supraventricular and ventricular stimuli and, what is interesting, rather a slow-down than an acceleration of cardiac function. During OAC, the patients did not report any other symptoms, in particular any chest pains, nor were there any changes in the registered material that would be an indication for early discontinuation of OAC, in particular regarding changes in the ST-T segment, which confirms that ischemic heart symptoms are a very rare manifestation of hypersensitivity, and monitoring by available methods (Holter ECG, DBPM) does not allow to register them.
Conclusions
There were no clinically significant cardiac arrhythmias recorded during OAC, and the observed changes in the records of BP and ECG monitoring show that OAC performed in accordance with the current guidelines does not pose a high risk to the patient’s health and life as a result of cardiovascular reactions. However, there is a risk of severe anaphylactic reaction and/or circulation risk during OAC, especially in patients with asthma and airway obstruction after NSAIDs. The fact that not all objectively occurring respiratory and circulatory disorders during the performance of OAC were experienced and reported by patients, as well as the need to provide appropriate assistance in the case of OAC(+) and to monitor its efficacy, result in a situation where OAC should be performed in a hospital setting.







