
Introduction
Systemic sclerosis (SSc) is a rare, generalized connective tissue disease in which one of the most common manifestations is skin thickening (sclerosis). The disease affects the skin of the face – resulting in a mask-like appearance due to dermal fibrosis and a narrowed oral aperture [1–6]. Skin changes of the upper and lower extremities also impair daily functioning and independence.
Functional performance criteria and analysis of their outcomes provide key information regarding treatment effectiveness. Functional assessment scales are clinically meaningful only when they are both scientifically valid and clinically applicable.
Aim
The aim of the study was to analyse hand joint function, strength, chest expansion, exercise tolerance using the 6-minute walk test (6MWT), and the range of temporomandibular joint (TMJ) movements in patients with systemic sclerosis treated at the Dermatology Clinic of PIM MSWiA following 2 years of physiotherapy.
Material and methods
For over 20 years, patients with systemic sclerosis – a chronic and progressive disease – have been treated at the Department of Dermatology, State Medical Institute of the Ministry of the Interior and Administration (PIM MSWiA), Warsaw.
Physiotherapy was based on individually selected exercises and self-massage routines, adapted to the patients’ abilities.
Chest expansion measurement
Chest expansion was assessed by measuring the difference in thoracic circumference between full inspiration and full expiration.
Six-minute walk test
The 6MWT was performed along a hospital corridor 30 meters in length, with markers placed every 1 m. Patients were instructed to walk as far as possible at their maximum pace. The following parameters were measured immediately before and after the test, and every minute until values returned to baseline: arterial oxygen saturation (SpO2), heart rate (HR), blood pressure (BP), dyspnoea and fatigue using the 10-point Borg scale.
Hand strength
Before, during, and after therapy, hand muscle strength was assessed using an electronic dynamometer for both left and right hands.
Temporomandibular joint (TMJ) mobility
The following active mandibular movements were measured: abduction (mouth opening): Normal range in healthy adults – 40–50 mm, lateral movements: Normal range – 6–10 mm, protrusion (forward movement): Normal range – 4–7 mm.
According to Cornu and Dechoux [7], average active mandibular mobility values in adults without pathology are presented in Table 1.
Table 1
The average values of active mobility in adults without pathology
| Movement type | Mean ± SD [mm] |
|---|---|
| Abduction | 50.2 ±6.5 |
| Forward movement | 7.3 ±2.6 |
| Right lateral movement | 9.1 ±2.8 |
| Left lateral movement | 9.9 ±3.0 |
The mandibular opening was measured between the incisal edges of the upper and lower central incisors. Lateral movements were assessed as the distance between the midline of the maxilla and the mandible during maximal lateral displacement of the mandible without occlusal contact from the resting mandibular position. Protrusion was defined as the distance between the labial surface of the upper incisors and the lingual surface of the lower incisors during maximal forward movement of the mandible, with minimal interincisal spacing [8–15].
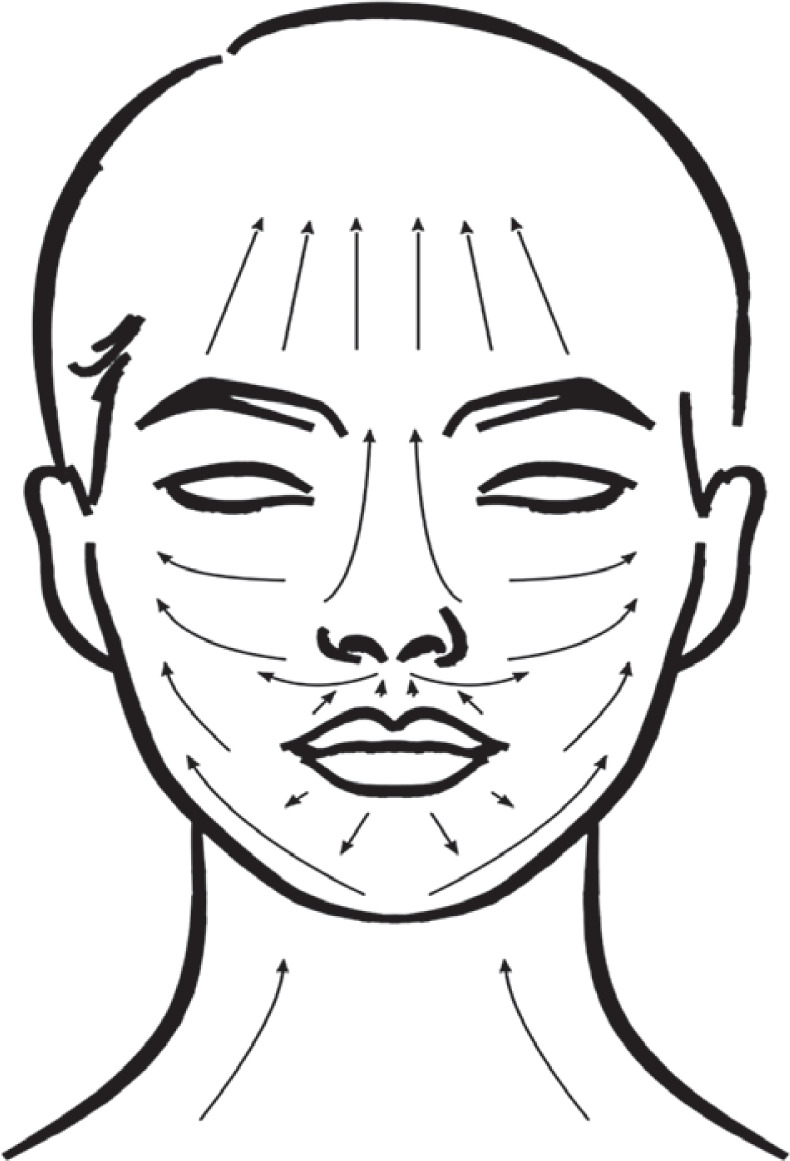
Facial self-massage protocol
Patients were instructed to perform facial self-massage at least twice weekly for a minimum of 10 min per session. Using learned techniques, cream was to be applied every morning and evening after handwashing and facial cleansing. Movements were performed with the middle and index fingers, or with the dorsal surfaces of the hands or forearms, depending on the patient’s capability. The massage technique involved the following directions:
From the mandible upward toward the cheeks and forehead,
From the lower lip downward and then upward toward the cheeks,
From the upper lip upward and toward the cheeks,
Across the cheeks toward the ears and forehead,
Along the nose upward toward the forehead,
Circular motions under the lower eyelid from the outer to inner corner, and along the upper eyelid in the opposite direction,
Upward motions across the forehead,
Neck skin massaged upward toward the face (Figure 1).
Facial muscle exercises
After massage, patients performed active facial mimic exercises in front of a mirror twice daily (morning and evening). These consisted of exaggerated articulation of the vowels A, O, U, and I, with maximal stretching of the perioral skin.
Upper limb self-massage and manual exercises
Patients were instructed to perform upper limb massage twice weekly for at least 10 min. The technique began at the wrist and continued proximally to the elbow, covering both palmar and dorsal hand surfaces from fingers to the wrist joints, then each finger individually from distal phalanx to metacarpus. Movements were performed with fingers, the dorsal part of the hand, or the forearm, always in the direction of the heart. Cream application was recommended in the morning and evening after cleansing the skin.
After massage, manual exercises were performed:
Results
For each measured variable, linear correlation coefficients were analysed, and a standard linear regression model was developed with calculation of standard errors for parameter estimation. To evaluate which parameters were most affected by the intervention, an effect size analysis was conducted using Cohen’s d statistic.
Traditionally, Cohen’s d is used to compare means between two independent groups. In this study, a modified version of the index was applied to a single experimental group to estimate the magnitude of change within subjects, based on repeated measures before and after rehabilitation.
The results are summarized in Table 2.
Table 2
Significance levels for the correlation coefficient test
Cohen’s d is typically recommended for sample sizes n > 50. For smaller samples, a correction factor can be applied to obtain the adjusted Cohen’s d. Both unadjusted and adjusted effect size values are shown in Table 3.
Table 3
Comparison of Cohen’s d and adjusted Cohen’s d effect sizes
Interpretation of effect sizes
Effect size values were interpreted according to standard thresholds:
|d| < 0.2 – very small or negligible effect,
|d| ≈ 0.2 – small effect (slight but possibly noticeable change),
|d| ≈ 0.5 – medium effect (moderate change visible to an average observer),
|d| ≥ 0.8 – large effect (significant change with substantial clinical importance).
Based on the data, the greatest improvement was observed for left lateral mandibular movement (+35.67%), indicating that facial exercises and self-massage had the strongest effect in this parameter. The impact on right lateral mandibular movement was small or negligible (+13.30%), suggesting that rehabilitation effects were not symmetrical. The second most pronounced improvement was noted for mandibular abduction (+26.72%), followed by left hand strength (+21.67%).
The analysis confirmed that patients with systemic sclerosis exhibit significant impairment in small hand joint mobility. The effect on right hand strength (+11.99%) was less marked, possibly due to hand dominance – most participants were right-handed. Thus, exercises and self-massage may have resulted in a relatively greater improvement in the non-dominant hand.
Correlation analysis demonstrated a strong linear relationship between left and right hand strength across all measurement stages. Both absolute strength (in kg) and the changes over time exhibited consistent patterns, confirmed by statistically significant correlation tests. This indicates that the implemented exercise and self-massage protocols produced balanced functional gains in both upper limbs. Minor deviations from perfect linearity likely reflect individual variability, yet overall results confirm that the rehabilitation method influenced both hands comparably.
In contrast, chest expansion showed no improvement; in fact, a slight deterioration was noted.
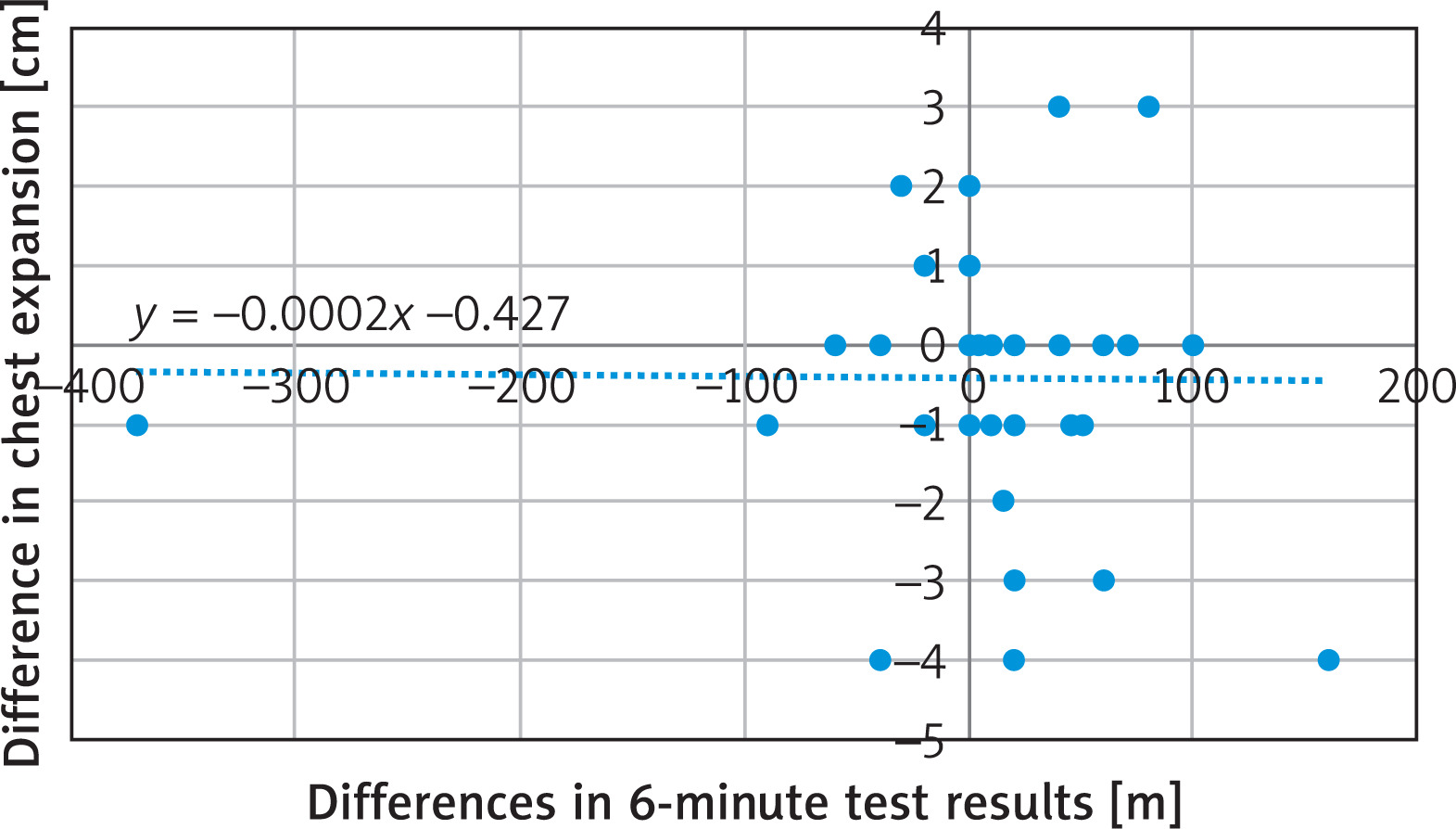
Results from the 6MWT, measured with 1-meter precision, allowed for more differentiated findings. However, chest expansion was assessed with 1 cm precision – too coarse to capture small-scale variability, yielding only eight possible measurement values (0–7 cm). Future assessments with millimetre precision could improve regression model accuracy. No correlation between the variables was found.
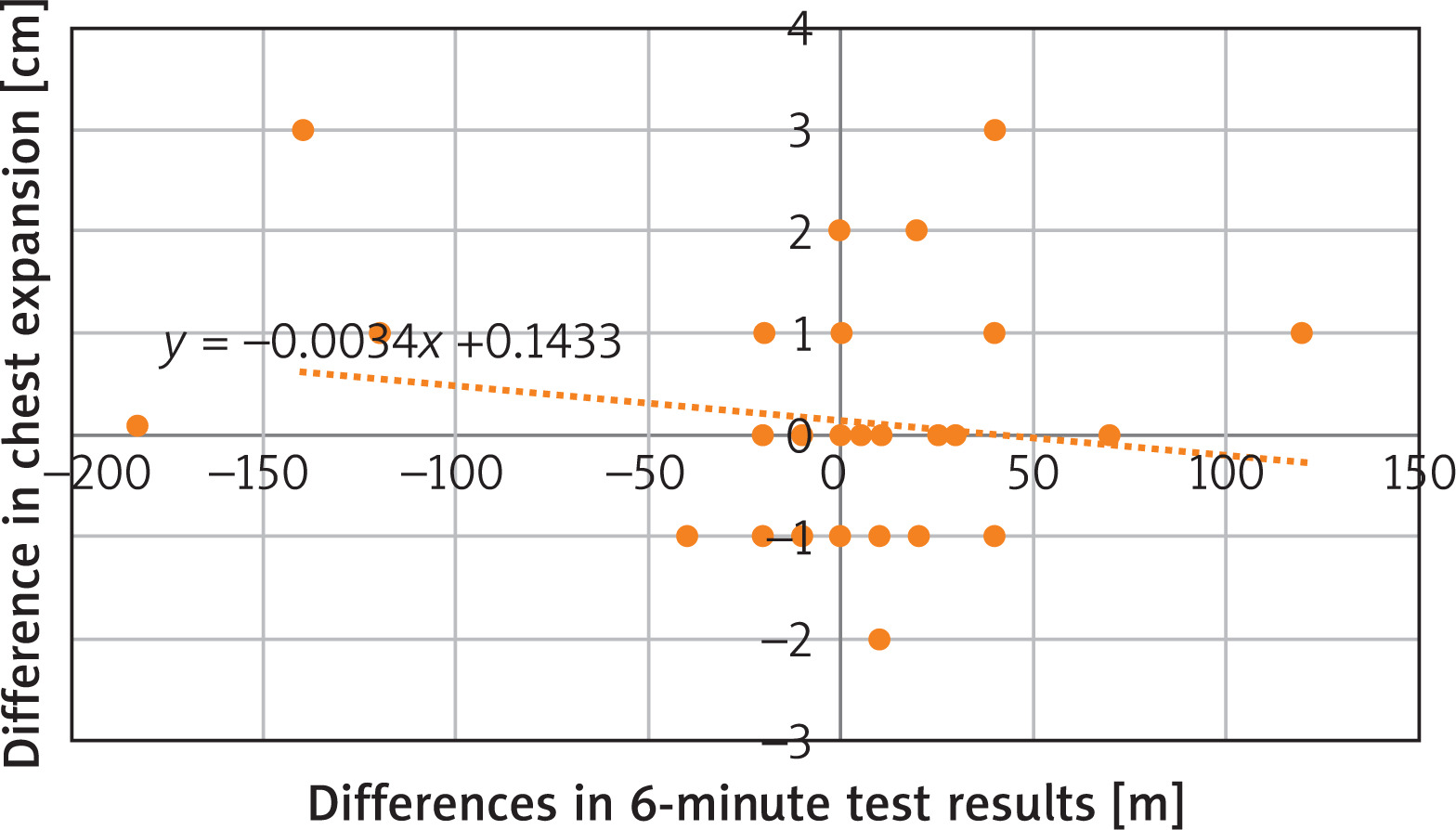
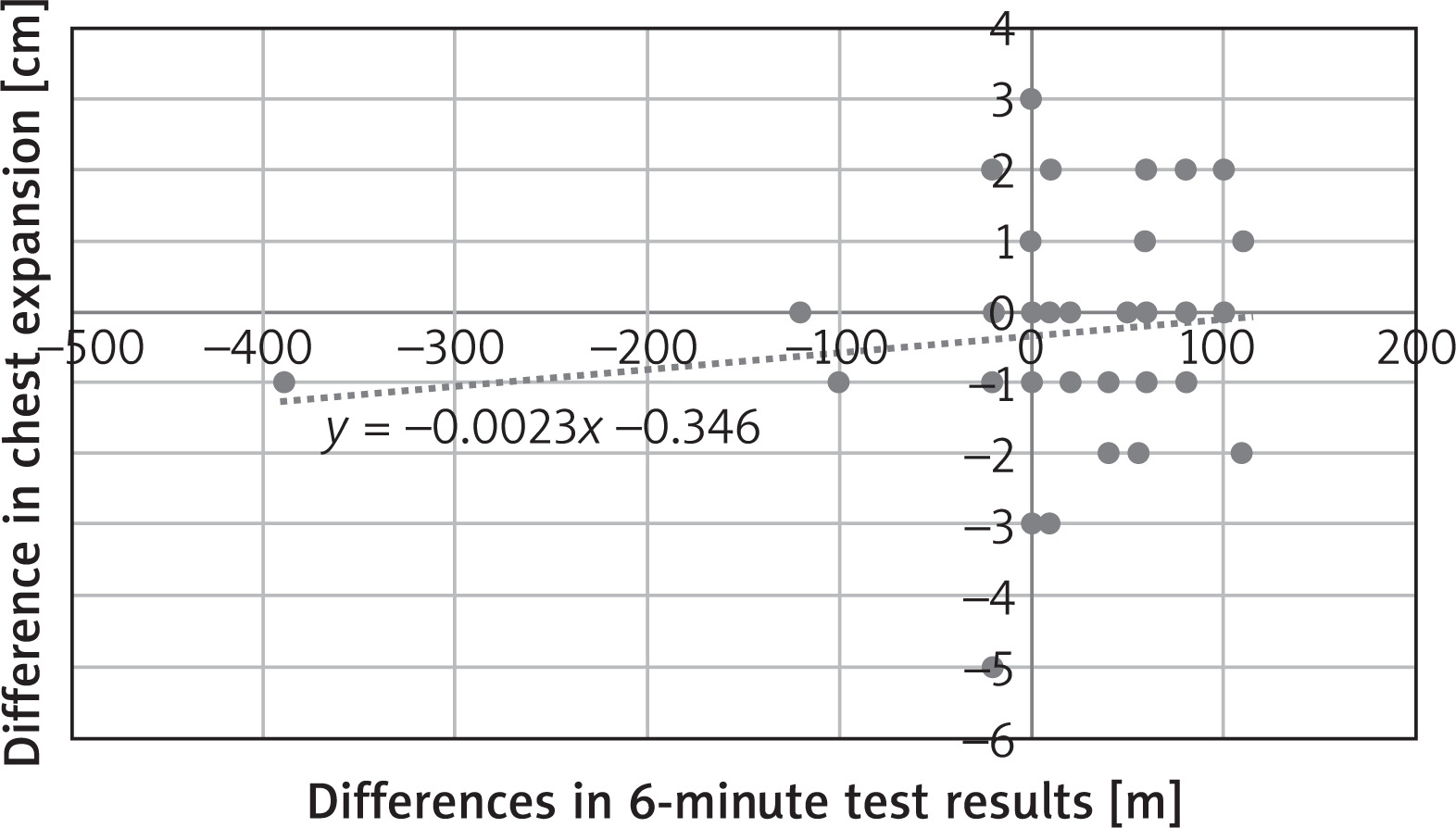
Pearson correlation coefficients (ranging from approximately –0.12 to +0.12) and Spearman correlation coefficients (from –0.01 to +0.12) indicate very weak correlations between the tested variable series. Analysis of plotted results confirmed the absence of clear relationships such as linear, power-law, exponential, or logarithmic distributions (Figures 2–4).
Figure 2
Comparison of the difference in 6-minute walk test results and chest expansion at the beginning of the study with a fitted linear regression curve
Discussion
Systemic sclerosis (SSc) is a progressive autoimmune connective tissue disorder that leads to multiorgan dysfunction, including involvement of the heart, lungs, and musculoskeletal system [5, 6, 8, 9]. Functional performance criteria and their quantitative analysis provide essential data regarding therapeutic efficacy. Functional assessment scales are clinically meaningful only when they consider and integrate all comorbid factors influencing disease activity and patient capability [10].
Chest expansion
Chest expansion reflects thoracic mobility during respiration – defined as the difference in chest circumference between full inspiration and expiration. In healthy adults, normal chest expansion typically ranges from 3.5 to 6 cm, though some studies report values up to 12 cm [11]. Restriction of thoracic mobility in SSc may result from both fibrotic skin involvement of the chest wall and interstitial lung disease, significantly compromising ventilatory mechanics and oxygen transport.
Six-minute walk test
The 6MWT is a widely accepted, objective measure of submaximal exercise capacity in patients with cardiopulmonary and rheumatic diseases. In SSc, the 6MWT outcome is influenced by multiple systemic factors, including vascular, pulmonary, and musculoskeletal limitations [12, 13]. To interpret 6MWT results accurately, it is advisable to concurrently assess: pulmonary diffusing capacity for carbon monoxide (DLCO), membrane diffusion capacity and capillary blood volume, scleroderma health assessment questionnaire (SHAQ) disability index.
Such multimodal evaluation helps to contextualize 6MWT outcomes and differentiate between pulmonary, cardiac, and peripheral limitations [14].
Additionally, gait alterations secondary to skin fibrosis of the lower legs and feet, and muscle weakness, may significantly affect walking performance [13–16]. SSc-related fibrosis of the skin and subcutaneous tissues leads to joint contractures and reduced mobility, further diminishing exercise tolerance.
Rodnan skin score and clinical prognosis
The modified Rodnan skin score (mRSS) quantitatively assesses skin thickness across 17 anatomical sites (face, chest, abdomen, arms, forearms, hands, fingers, thighs, legs, and feet). It is a critical prognostic factor in systemic sclerosis [17]. Higher scores correspond to more extensive dermal fibrosis and are associated with greater organ involvement and poorer prognosis, whereas limited skin thickening is a favourable prognostic indicator [17].
Hand function and strength
Hand strength and dexterity are influenced by both cutaneous and articular changes. Fibrosis of the dermis and periarticular tissues restricts motion in proximal and distal interphalangeal, metacarpophalangeal, wrist, and elbow joints. Digital deformities and resorption of phalanges further compromise grip quality.
Strength assessment using a dynamometer provides objective data, whereas hand-specific functional questionnaires such as: Scleroderma health assessment questionnaire (SHAQ), Modified hand mobility in scleroderma (mHAMIS) test, and Duruöz hand index (DHI), evaluate fine motor function and activities of daily living [3, 18–20]. In physiotherapeutic settings, finger goniometers are also used to assess digital joint range of motion.
The present study demonstrated measurable improvements in hand grip strength, particularly in the left (non-dominant) hand, suggesting that regular self-massage and targeted manual exercises can partially reverse soft tissue rigidity and improve perfusion.
Temporomandibular joint (TMJ) mobility
Destructive changes in the temporomandibular joint are common in systemic sclerosis and result in progressive microstomia, limited mandibular movement, and difficulty with mastication and oral hygiene. Severe restriction may necessitate surgical reconstruction using costochondral grafts [3]. In this study, rehabilitation produced notable gains in lateral mandibular movement and abduction, reflecting improved elasticity of perioral tissues and masticatory muscles following facial exercises and massage. No significant change was observed in protrusive movement, indicating persistent structural limitation within the TMJ capsule [21–24].
Interpretation of findings
The 2-year physiotherapy program combining facial mimic exercises, manual hand therapy, and self-massage demonstrated selective but meaningful functional benefits. While thoracic expansion deteriorated slightly, other parameters – including hand strength, TMJ mobility, and 6MWT distance – showed improvement, suggesting that localized soft tissue interventions can enhance mobility even in the context of systemic disease.
However, the absence of symmetry in TMJ movement improvement and the limited gain in thoracic excursion highlight the heterogeneity of SSc pathology and the need for individualized rehabilitation protocols.
Conclusions
In patients who did not perform the prescribed exercises and self-massage, improvement was negligible (as seen in the 6-minute walk test) or even negative (as in chest expansion).
In contrast, among patients who underwent the 2-year rehabilitation program, improvements were observed in temporomandibular joint mobility, although the effects varied across specific parameters. Abduction and lateral movements improved asymmetrically, whereas protrusive movement showed no measurable change.
Following regular exercises and self-massage, patients with systemic sclerosis demonstrated a noticeable increase in hand strength. The improvement in right-hand strength was smaller compared to the left hand, which may be attributed to hand dominance, as most individuals in the studied population were right-handed.
Overall, the results confirm that long-term physiotherapy incorporating manual therapy and self-massage can effectively enhance joint mobility and muscular strength, particularly in regions affected by fibrotic skin changes. Such interventions should be considered an integral component of multidisciplinary SSc management, complementing pharmacological treatment and promoting patients’ functional independence.







