








Introduction
Each year, approximately 1.3 million patients are hospitalized for pneumonia, and pleural effusion occurs in an average of 36–66% of these patients [1]. Parapneumonic effusions are currently uncommon due to rapid and effective antibiotic therapy. It has been reported that complicated effusions that occur after pneumonia turn into exudative fluid at a rate of 10–20% and require drainage or surgery [2, 3]. Evaluating the patient with rapidly accessible imaging methods such as chest X-ray, pleural ultrasound and chest computed tomography and performing fluid drainage with thoracentesis provide early diagnosis and optimal treatment. Despite this, in some patients, parapneumonic effusion becomes fibrous and empyema occurs [4]. Empyema is of great importance to clinicians due to morbidity, mortality and hospital costs. Treatment options range from antibiotic therapy, thoracentesis, chest tube insertion, fibrinolytic therapy, intrathoracic negative pressure therapy and/or endobronchial valve implantation, to decortication with video-assisted thoracoscopic surgery (VATS) or thoracotomy [5–7]. The main goal in treatment is to increase lung expansion. For this, it is aimed to drain the fibrin deposits by reducing the viscosity of the fluid in the thoracic cavity [7, 8].
In patients with empyema, a decrease in fibrinolytic activity in pleural fluid, high TNF-α, high concentrations of plasminogen activator inhibitor and tissue plasminogen activator have been shown to decrease [9]. For these reasons, fibrinolytic therapy has become used in the treatment of empyema. It is aimed to reduce the viscosity of the empyema fluid by lysis of the fibrin deposits and to facilitate drainage [10]. As a result, there have been increasing numbers of studies reporting the results of intrapleural fibrinolytic application in the literature in recent years. Many fibrinolytic agents such as streptokinase, urokinase, alteplase or dornase alfa are used for this purpose [11]. On the other hand, surgery performed with VATS or thoracotomy is still available as an effective treatment modality.
Aim
In this study, we aimed to compare the treatment results of patients who underwent interpleural alteplase treatment and who underwent surgical deloculation accompanied by videothoracoscopy.
Material and methods
The results of 49 patients who were treated for empyema in our clinic between March 2015 and August 2020 were evaluated retrospectively. Twenty-one patients who underwent tube thoracostomy + intrapleural alteplase (group 1) and 28 patients who underwent VATS deloculation (group 2) were included in the study. Radiological examination results, treatment responses, hospitalization period, bacterial growth in culture, comorbid conditions and demographic structures of our patients were evaluated. As a standard, thorax computed tomography (CT) was performed in each patient before the procedure and diagnostic thoracentesis was performed. Results were evaluated retrospectively. Patients with known bleeding diathesis, recent cerebrovascular bleeding, bronchopleural fistula and coagulopathy were not included in alteplase treatment.
Intrapleural alteplase irrigation technique
A 28 or 32 French (F) thorax tube was applied to the patients under local anesthesia by determining the localization according to the loculation area on thorax CT. Alteplase treatment was administered intrapleurally to the patients after drainage of empyema from the thorax tube. Alteplase is available in a 50 mg vial and 50 ml of sterile liquid for injection. In order to make a ready-made solution, the powder containing the active ingredient and the sterile liquid in the vial was mixed and a ready-made solution containing 1 mg of the active ingredient in 1 ml was formed. For intrapleural lavage to be applied through the thorax tube, the lavage fluid was prepared by mixing 10 ml of ready-made solution into 100 ml of isotonic fluid. The thorax tube was clamped, and lavage fluid was applied to the thoracic cavity twice a day, and the clamp was opened 1 h later. During this time, the patient was placed in a right lateral position for 30 min and left lateral positions for 30 min.
Videothoracoscopic deloculation technique
Patients suitable for general anesthesia were intubated with a standard double lumen tube, and then a left or right lateral position was used. Patients with high risk for general anesthesia were operated on using the non-intubated VATS technique. The localization of the incisions was decided according to the thoracic CT image. A 3-cm incision was made at the appropriate location for the uniport technique, and a 1-cm incision was made at three locations for the multiport technique. Deloculation and decortication procedures were performed using VATS instruments, endo dissectors and surgical energy devices. At the end of the operation, the thoracic cavity was irrigated with saline solution to control air leakage and drainage of fibrin materials was performed. A 28 F drain was placed in the thoracic cavity as a standard.
Expansion of the lungs, stopping of air drainage, drainage fluid becoming serous, and fluid drainage below 200 ml within 24 h were accepted as discharge criteria for both groups.
Statistical analysis
Data were analyzed using the SPSS 20 program. A univariate analysis was performed to determine possible predictors of successful resolution of symptoms. Multivariate analysis was used to determine the factors affecting the treatment outcome. Student’s t test was used to compare the means of successful and non-successful groups. The Mann-Whitney U test was used for comparisons between groups. A p-value of less than 0.05 was considered significant.
Results
The study included 49 patients, 35 (71.5%) male and 14 (28.5%) female. There were 21 (42.7%) patients in group 1, and 28 (57.1%) patients in group 2. The mean age was 50.6 ±17.8 (23–82). There was no statistically significant difference between the patient groups in terms of gender distribution or age (p = 0.785 and 0.294) (Table I).
Table I
Patient demographics
The number of intrapleural alteplase lavage irrigations in 21 patients in group 1 was as follows: in 5 (23.8%) patients, 10 mg (10 times) twice a day for 5 days and in 16 (76.2%) patients 10 mg (5 times) twice a day for 3 days. In this group, empyema was on the right side in 14 (66.7%) patients and on the left side in 7 (33.3%) patients. The Visual Analogue Scale (VAS) pain score measured 24 h after the insertion of the thorax drain was found to be 2.1 ±0.7. As comorbidities, 4 (19%) patients had diabetes mellitus, 3 (14.2%) patients had malignancy, 2 (9.5%) patients had COPD, and 1 (4.7%) patient had cerebral palsy. The average number of days in which patients in our group were symptomatic during the period before tube thoracostomy was 5.2 ±2.2. In group 1, 28 French (F) thorax tubes were used in 13 patients and 32 F thorax tubes in 8 patients. Fluid appearance of all patients was detected as purulent and culture growth was observed in 6 (28.6%) patients.
At the end of the treatment, exploration and deloculation with VATS were performed in 4 (19%) patients because of the ineffectiveness and failure of the treatment. In 17 (81%) patients, the treatment was discontinued without the need for surgery, and the patients were discharged by removing the thorax tube. Three patients were discharged by placing a Heimlich valve in the thorax tube due to continuing drainage. The average length of thoracic tube stay was determined as 7.1 ±2 days. One (4.7%) patient had non-massive bleeding that did not require transfusion, following the last dose of alteplase treatment. In addition, we did not have any patients whose treatment could not be completed for any reason. It was decided to terminate antibiotherapy in our patients after consultation with the Department of Infectious Diseases. In our patient series, complications developed in 4 (19%) patients in group 1, expansion defect in 2 patients (Photo 1), cardiac arrhythmia in 1 patient and wound infection in 1 patient. The duration of hospital stay in this group was 6.73 ±1.94 days (5–10).
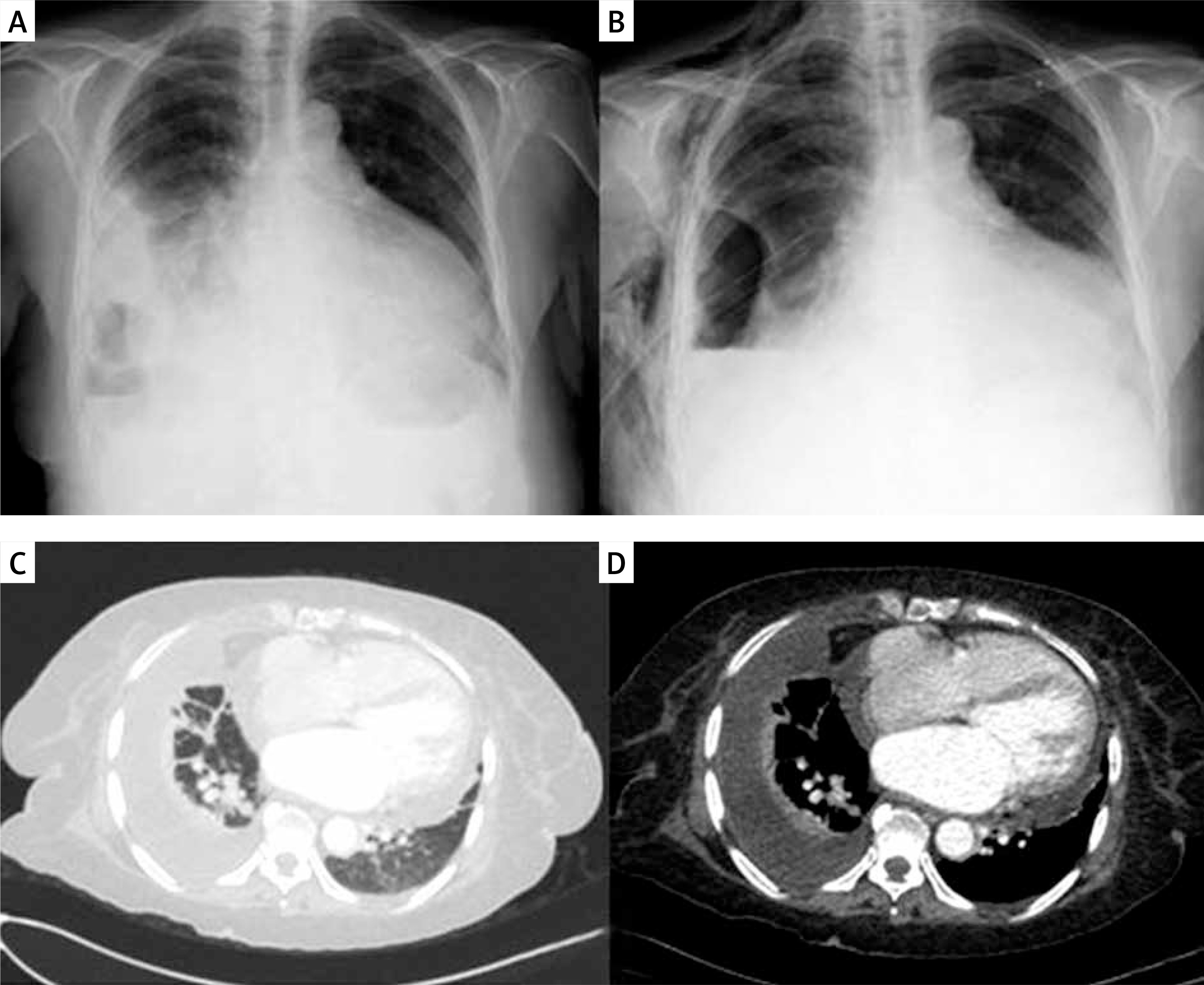
Photo 1
Pre-procedure (A, C, D) and postoperative images (B) of our patient with expansion defect after tube thoracostomy and intrapleural alteplase irrigation
There were 28 patients in the group in which we applied decortication or deloculation with video-assisted thoracoscopic surgery. The procedure was performed on the right side in 18 (64.3%) patients, and empyema was located in the left hemithorax in 10 (35.7%) patients. When both groups were evaluated in terms of empyema location, no statistically significant difference was found (p = 0.937). As comorbidities, 5 (17.9%) patients had COPD, 4 (14.2%) patients had diabetes mellitus, 4 (14.2%) patients had malignancy, and 2 (7.1%) patients had cardiac disease. There was no difference between the groups in terms of comorbidity (p = 0.292). The average time from the onset of symptoms to the surgical procedure in patients in group 2 was 6.57 ±3.46 days.
A uniportal procedure was performed in 19 patients in the VATS-D group (Photo 2), and triportal VATS was performed in 9 patients; in 4 of these patients the surgical procedure was performed non-intubated because general anesthesia was found to be high risk. In the pleural fluid cultures taken during the operation, growth was detected in 5 (17.8%) patients. In the postoperative pain scoring, the VAS value was 2.86 ±0.9; this value was significantly higher than group 1 (p = 0.002). A 28 French thorax tube was used as a thorax drain in all patients in this group; the duration of the drain was determined as 6.96 ±2.7 days. There were 8 patients who were discharged with a Heimlich valve, and the thorax tube was removed during outpatient follow-ups. There was no statistically significant difference in terms of drain duration (p = 0.853). Minor complications occurred in 6 (21.4%) of our patients, 3 had prolonged air leak and expansion defect, 2 patients had wound infection and 1 patient had cardiac arrhythmia. The duration of hospital stay was 6.35 ±1.32 days and there was no significant difference between group 1 and group 2 (p = 0.181). In this group, 3 (10.7%) patients required thoracotomy for decortication and there were 25 (89.3%) patients whose treatment was successful with VATS-D.

Discussion
Parapneumonic effusions mostly develop secondary to pulmonary infection, while conversion to empyema and chronicity usually occur as a result of non-response to antibiotherapy. In the treatment of these patients, deloculation with drainage or surgery in addition to antibiotherapy, and decortication in chronic empyema are required [12]. In the case of empyema, the presence of multiloculation or septations reduce the treatment response and drainage of empyema fluid [13]. The use of fibrinolytic agents intrapleurally in order to increase the drainage by reducing the viscosity of empyema fluid after chest tube placement or surgery increases the effectiveness of the treatment [14]. Various agents are used for this purpose. However, the ideal fibrinolytic agent should have a short half-life, have high fibrin selectivity and specificity, and can be applied by a non-invasive method [15]. Various fibrinolytic agents such as streptokinase, urokinase, alteplase and DNase can provide this effect. Streptokinase has low fibrin affinity and specificity, has little effect on empyema viscosity, but is still used due to its safety [16].
Alteplase, which we used in our study, has a high fibrin affinity and fibrin selectivity, and a half-life of 4–8 min, so it is an ideal fibrinolytic agent for intrapleural use [17]. Thommi et al. [18] investigated the use of alteplase in 120 patients who failed chest tube application due to empyema. In their study, they reported that they achieved treatment success in 105 (85%) patients after intrapleural fibrinolytics administered at different doses. The partial success rate was 8% in the same group, while the percentage of patients who did not respond to treatment was only 7%. In our series, the success rate after alteplase treatment was found to be 81%. In 4 (19%) of our patients, the patients were subjected to VATS deloculation because no response to treatment was obtained. In a similar study, Rahman et al. [19] concluded that alteplase is effective only when combined with DNase. However, in this study, the researchers’ use of chest radiography instead of thoracic CT to determine the response to intrapleural therapy may have caused them to misinterpret the treatment results.
In the retrospective study of Taylor et al. [20] with 73 patients, it was found that mortality decreased, the duration of hospital stay was shortened and the rate of transition to surgery decreased as a result of intrapleural alteplase administration. In another study, Zuckerman et al. [21] randomized and prospectively administered tissue plasminogen activator intrapleurally to 25 patients; it was reported to be effective in the treatment of loculated-complicated parapneumonic effusion and empyema, and the absence of patients requiring thoracotomy is also important in terms of treatment effectiveness. Sumalani et al. [22] obtained satisfactory results with VATS treatment in 202 (86.3%) patients in their study on 234 patients. Forty patients in this group requiring decortication or repeat procedures with thoracotomy had a longer mean symptom duration and longer preoperative hospital stay than patients treated with VATS. In our study, there was a higher symptom duration in the VATS-D group compared to the intrapleural treatment group.
In the study of Sumalani et al. in which they performed medical thoracoscopy under local anesthesia, they reported complete resolution in 92 (57.5%) of 160 patients and partial resolution in 58 (36.25%) patients. They concluded that this procedure is an effective and reliable method, especially in patients with high risk for general anesthesia. In our study group, there were 4 patients who underwent VATS-D non-intubated; these patients were ASA-4 patients who were at high risk for general anesthesia. On the other hand, VATS-D was performed through a uniportal incision in 19 patients. There was no significant difference between the intrapleural alteplase group and the patient group treated with VATS-D between the length of stay of the drain and the length of hospital stay (p = 0.853, p = 0.181). In terms of VAS pain scores evaluated at the 24th hour after tube thoracostomy in the alteplase group and in the VATS-D surgical group, there was a significant increase in the surgical group (p = 0.002). There are many studies showing that there is a difference between multiport technique and single port technique in terms of postoperative pain. It has been reported that there is less pain in single port VATS application [23–25]. In the study of Ismail et al. including 35 patients, they stated that all patients were provided with full debridement and decortication with the U-VATS approach and thoracotomy was not required for any reason, and no significant complications were noted in this group.
Conclusions
VATS-D is an effective treatment option in the treatment of pleural empyema. However, as seen in our study, intrapleural alteplase application is at least as effective as VATS-D in terms of treatment success. The absence of a significant difference between drain length, hospital stay and post-procedure complication rates showed that both methods can be preferred in eligible patients. It is not clear which criteria will be decided in terms of preference for surgery or intrapleural application of alteplase. In addition, performing treatment cost analysis for both techniques and evaluating them in terms of cost-effectiveness will guide us. Therefore, larger series and prospective, randomized controlled studies are needed.