
Dear Editor,
Septic shock is a life-threatening condition. The mortality rate for septic shock amounts to 50% [1], the percentage that has been remaining at this high level for years [2, 3]. The Surviving Sepsis Campaign took the initiative to publish the updated guidelines for optimal diagnostic and therapeutic management of sepsis [4].
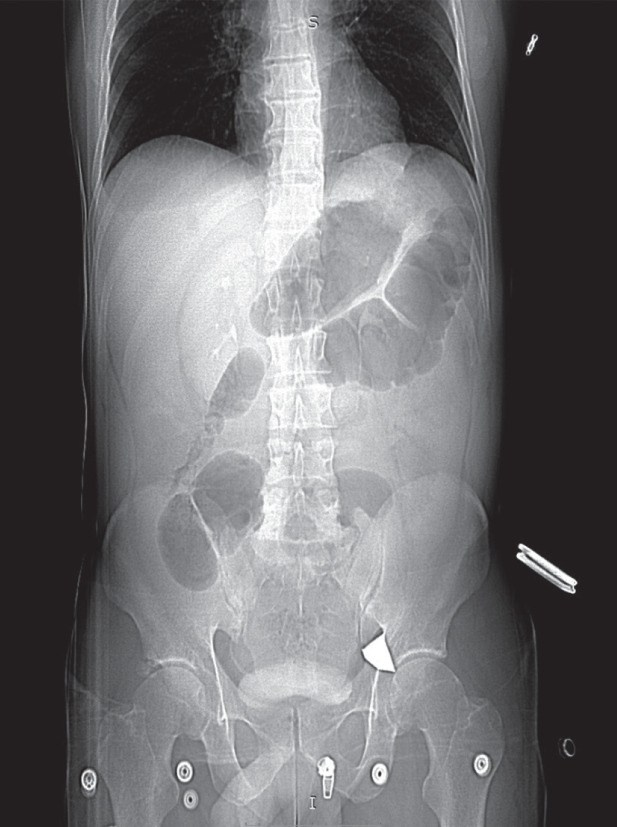
A 43-year-old man had an accident during wood cutting with a circular saw. He sustained a chest injury at the level of the right costal arch caused by a tooth broken off from the circular saw (about 30 × 7 mm in diameter). The patient was transported to the nearest Accident and Emergency Department where he underwent computed tomography (CT), which visualized an interstitial hepatic haematoma, an epigastric haematoma, duodenal perforation and possible splenic marginal rupture. Moreover, the CT scan revealed a metallic foreign body located in the region of the left common femoral vein (Figure 1). The patient was emergently transferred to the operating suite of the Department of General Surgery. During laparotomy the haematoma was evacuated from the peritoneal cavity of the epigastric region, which was followed by duodenorrhaphy with single sutures, local haemostasis, and insertion of a drain into the area of duo-denal injury. Due to haemodynamic instability associated with haemorrhagic shock, the evacuation of the foreign body was abandoned. On post-injury day 6, due to signs of alimentary tract perforation, relaparotomy was required, which revealed the necrotically-altered duodenal wall. Single sutures were placed within the necrotic area. Moreover, the injury to the extrahepatic biliary tract was recognised. Once the telephone consent was obtained, the patient was referred to the Department of Gastrointestinal Surgery and transferred to the Department of Anaesthesiology and Intensive Care for further treatment.
FIGURE 1
Thoracic and abdominal computed tomography scan performed on the day of injury resulting from a job accident. The scan visualises a metallic foreign body in the region of the left common femoral vein
On ICU admission, the patient’s condition was relatively fair; he was conscious and in logical contact, under opioid analgesia, his respiration was efficient while circulation inefficient but stable (noradrenaline in a dose of 0.09 µg kg-1 min-1). On day 8, follow-up CT was performed, which confirmed duodenal perforation and presence of fluid in the abdominal cavity. Emergency relaparo-tomy was undertaken. Within the next two hours, the patient developed the symptoms of shock: he was confused, periodically excited, with increasing respiratory failure (tachypnoea, dyspnoea) and circulatory failure (the Allgower index 2.8, centralization of circulation). Control arterial blood gas test demonstrated the lactate concentration of 4.8 mmoL L-1.
The patient underwent endotracheal intubation and mechanical lung ventilation was initiated. Fluid resuscitation with a balanced crystalloid in a dose of 30 mL kg-1 was administered, the dose of noradrenaline was increased to 0.6 µg kg-1 min-1. Blood was sampled for microbiological testing. Targeted antibiotic therapy (meropenem, colistin) was empirically widened and vancomycin was added. Once the patient was haemodyna-mically stable, he was transferred to the operating suite for emergency relaparotomy. During the procedure a reservoir of bloody and purulent biliary content and an extensive haematoma filling the retroperitoneal space and pressing the damaged inferior vena cava were evacuated. Torn at the segment of 3 cm, the inferior vena cava was repaired with continuous suture. Moreover, full-walled damage to the descending duodenum was found, involving more than half of its circumference; the extra-peritoneal part of the duodenum was reconstructed using end-to-end anastomosis, the prepyloric part of the stomach was cut and closed; subsequently, Billroth II gastrojejunostomy and cholecystostomy with a Kehr’s T tube were performed. Due to the local state and critical general condition of the patient, biliary tract reconstruction was not feasible.
On return to the ICU, the patient’s condition was critical, and he showed features of multiple organ failure. Control arterial blood gas test (ABG) demonstrated lactate concentration of 6.9 mmoL L-1, pH = 7.29, BE = –6 mmoL L-1, HCO3- = 16.6 mmoL L-1. With the fluid susceptibility continuously verified, the infusion of albumins and crystalloids was administered. The dose of noradrenaline was increased to 1.2 µg kg-1 min-1; additionally, terlipressin was included due to ongoing hypotension. Hemodiafiltration was initiated with regional citrate anticoagulation. Thanks to the treatment applied, the patient’s general condition improved; during the subsequent days, haemodynamic support with catecholamines support was diminished, renal replacement therapy was discontinued, and the patient was extubated. Qualitative disturbances of consciousness were observed, i.e. delirium, which required antipsychotic drugs.
On post-injury day 21, third rela-parotomy was deemed beneficial during which the necrotic tissues were removed, and the turbid biliary content was sucked out of the subhepatic region. Since that day due to extensive inflammatory and necrotic changes in this region, the open abdomen method was applied; the revision and seton replacement were planned to be performed every 2–3 days. The permeation of dressings with the duodenobiliary content and progression of abdominal tissue necrosis penetrating the right iliac and right lumbar regions were observed. The above symptoms were accompanied by pain requiring increased doses of opioid analgesics and multimodal adjuvant treatment. On day 27, follow-up CT demonstrated the contrast medium leakage from the alimentary lumen, most likely from the duodenal stump. Five days later during another revision, perforation of the colon was observed, which was locally secured with two layers of sutures; nevertheless, the situation re-occurred on hospitalization day 40.
After 45 days of ICU hospitalization, the patient’s clinical condition improved, which indicated that methods specifically reserved for the ICU were not required. The conscious, normally oriented to time, place and person patient with efficient respiration and circulation was transferred back to the hospital he was first admitted to further treatment in the Department of General Surgery. After three months of hospitalization, i.e. on post-injury day 138, the patient died.
To sum up, patients with septic shock emerging from an intra-abdominal infection and faced with the necessity to undergo numerous laparotomies, are a therapeutic challenge for surgical and anaesthetic teams. Even the management rigorously consistent with the international guidelines of sepsis diagnosis and treatment does not ensure recovery. The more complicated the chain of ailment pathophysiology, the higher the risk of failure.