








Introduction
Upper urinary tract urothelial carcinoma (approximately 5–10% of all urothelial carcinoma cases) rapidly develops in the renal pelvis and ureter [1]. Radical nephroureterectomy serves as the main treatment for the disease, and entire excision including the bladder cuff remains the gold standard [2]. In the 1990s, the laparoscopic technique began to be used in urology surgery and combined with nephroureterectomy [3]. With technological innovations, the retroperitoneal approach has been widely used in nephroureterectomy because of its clinical efficacy. However, surgeons are not satisfied with the retroperitoneal approach and are eager to find safer and more effective alternative procedures. Laparoendoscopic single-site (LESS) surgery, as a novel procedure, appeared by chance [4]. It is a critical stage in the evolution of laparoscopic surgery. In comparison with traditional retroperitoneal laparoscopic surgery, which requires 3–5 incisions, each at least 1–2 cm in length, LESS decreases the potential morbidity risks of bleeding and wounds [5, 6]. Apart from the above-mentioned advantages, patients may suffer less postoperative pain [7, 8].
Although early papers have demonstrated the safety and feasibility of the LESS procedure, analysis and comparison between LESS nephroureterectomy (LESS-NU) and retroperitoneal laparoscopic nephroureterectomy (RL-NU) are lacking. Based on our initial experience of the LESS procedure [9–11], we designed our own modified LESS-NU procedure with bladder cuff excision. It not only reduced the difficulty of the procedure and the operating time but also prevented patients’ intraoperative repositioning.
Aim
We aimed to introduce a modified LESS-NU procedure with bladder cuff excision designed by our department and compare the operative results between RL-NU and modified LESS-NU.
Material and methods
Patients’ selection
From May 2014 to May 2019, 25 patients underwent modified LESS-NU and 17 patients underwent RL-NU. The patients we enrolled in the study were diagnosed with upper urinary tract urothelial cancer (UTUC). Diagnosis of these patients was accomplished by urinary tract ultrasonography, intravenous pyelography (IVP), computed tomography (CT), MRU, cystoscopy, and ureteroscopy in our hospital. All patients with non-transitional cell carcinoma (non-TCC), bladder tumor, clinical > T3 disease, and metastatic disease on the preoperative staging were excluded. None of these patients had adjuvant chemotherapy before surgery.
RL-NU procedure
The RL-NU procedure was carried out as previously reported [12, 13]. After the induction of general anesthesia, the patients were placed in a lateral 90° position on the operating table. A 1.5 cm incision was made in the junction of the psoas edge and costal margin. A balloon was introduced and inflated to separate the retroperitoneal space. Then, 3–4 trocars were placed. After separating the kidney from the middle ureter to renal vein and artery, the patient was repositioned from lateral to supine. A new disinfecting and toweling process was performed. Subsequently, a large lower abdominal oblique incision was made to dissect the bladder cuff and lower ureter, and the intact specimen was extracted with a specimen bag. Finally, the surgery was completed after wound closure.
LESS-NU procedure
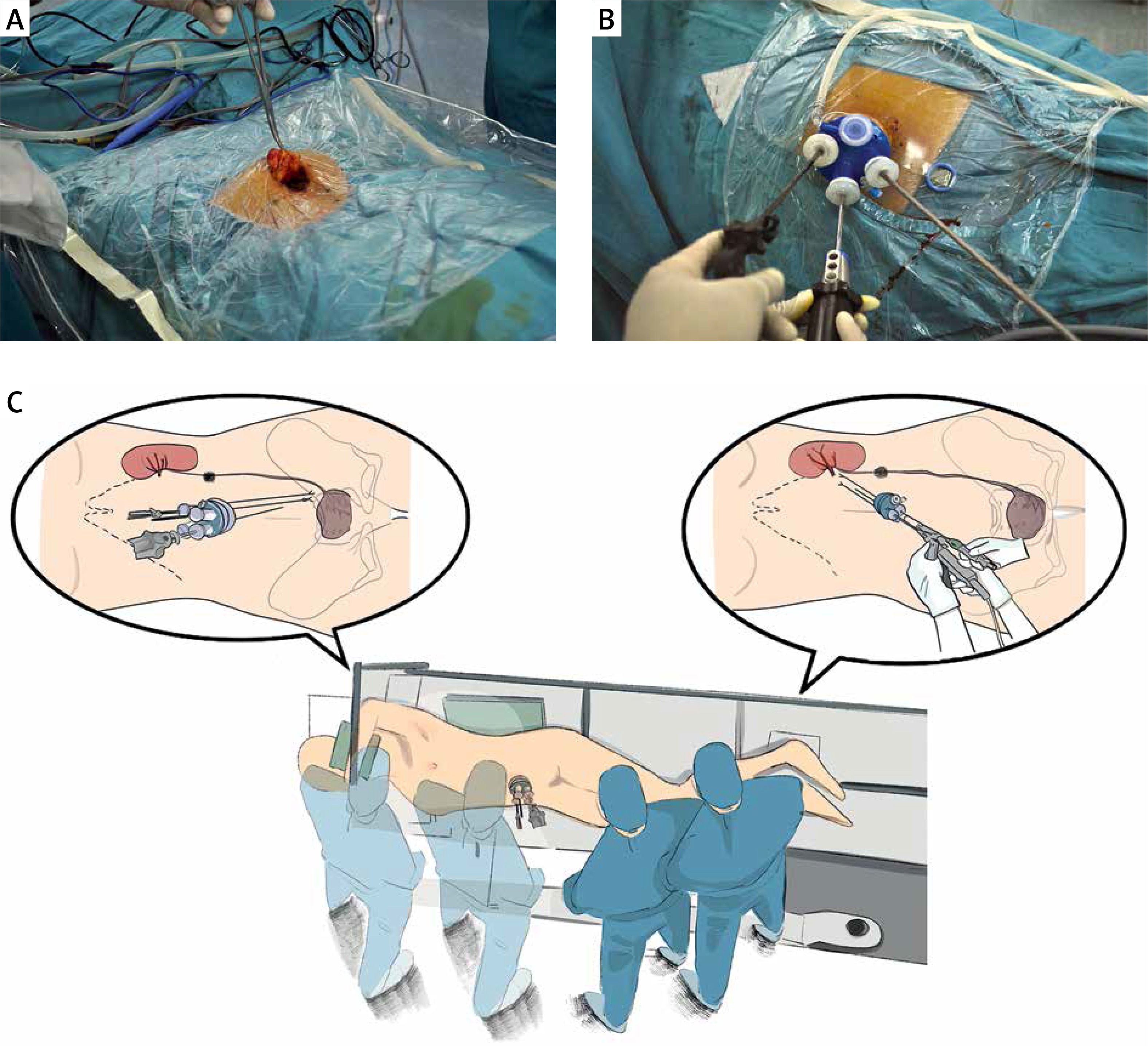
Under general anesthesia and endotracheal intubation, the patients were placed in a modified position, and the flank was elevated by 30–45° and fixed on the operating table. The entire procedure was carried out in the same position in addition to minimal leaning and tilting of the operating table. First, access was obtained via an approximately 3 cm midline circumferential umbilical incision (Figure 1 A). All the instruments were placed through the QuadPort (Innovex Bioscience, Shanghai, China) multichannel port (Figure 1 B). We insufflated carbon dioxide to maintain an intraperitoneal pressure of 15 mm Hg and settle the pneumoperitoneum.
Figure 1
Operation preparation and patient position. A – Circumferential umbilical incision was made. B – The instruments were manipulated through the QuadPort multichannel port. C – Patient is placed with flank elevated by 30–45°. During the operation, surgeons can dissect the kidney and ureter directly continuously
After identification of the anatomical sign, the paracolic sulci were opened. The entire colon slid downward due to gravity, thereby exposing the renal hilum. The renal fascia was incised, and the renal vein was identified. Behind the renal vein, the renal artery was exposed. Herein, the additional blood vessels were considered. EndoGIA was used to cut the renal pedicle after the renal artery was separated from the vein (Figure 2 A).
Figure 2
Key points in the LESS-NU procedures. A – The photo and diagram show the procedure of cutting off the renal vessel. B – The opened bladder wall was closed with running stitches by V-loc suture. C – The specimen is taken out through the patient’s umbilicus incision. Two drainage tubes were placed in the perirenal and pelvic cavity through the wound. D – The specimen was taken with integrality
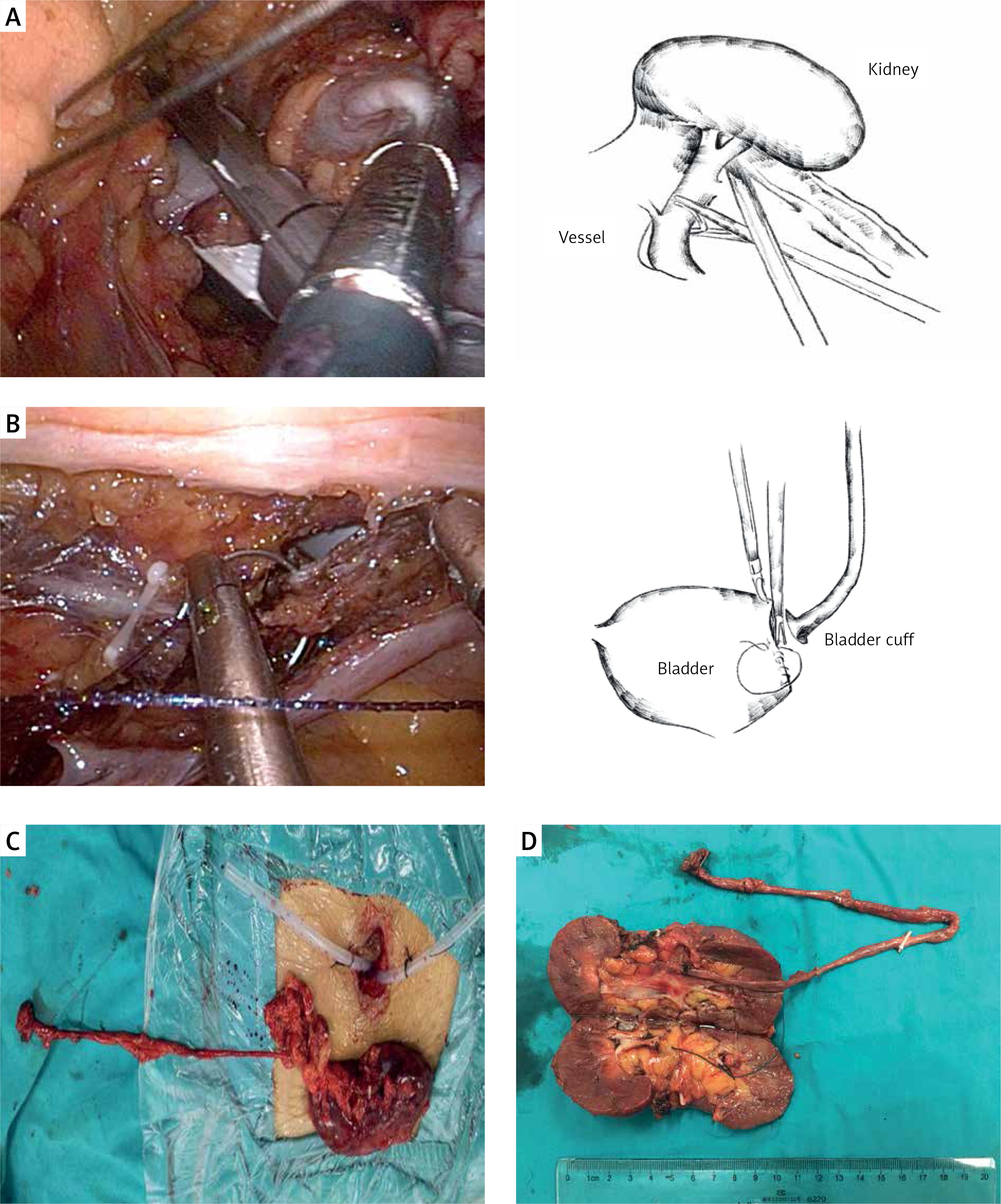
The kidney was sharp-separated gradually. After lifting up the inferior pole of the kidney, the renal pelvis and ureter were divided away from the paracolic. The ureter was lifted, and the tension was maintained. Then, the intact ureter was divided downward gradually. In this process, the surgeons just have to adjust the operation direction instead of the patients’ position (Figure 1 C). The bladder cuff was dissected around the ureteric orifice. Then, the bladder defect was closed with V-loc sutures by running stitches and tightening (Figure 2 B). The suture tail was clipped with Hem-O-loks without knotting. A homemade glove specimen bag was introduced, and all specimens were retrieved en bloc in the bag via the umbilical incision. The drainage tubes were placed in the perirenal and pelvic cavity (Figures 2 C, D). Finally, a catheter was introduced into the bladder, the pneumoperitoneum was evacuated, and the port was removed. The skin incision was closed with absorbable sutures.
Follow-up regime
After the operation, patients were reviewed with a complete blood count, serum electrolyte, and creatinine tests and CT imaging for three months in the first year. In the following time of the review, all patients were contacted by phone to update their status. Cystoscopy was performed when patients were symptomatic or when investigations were abnormal.
Statistical analysis
Patient demographics, including age, gender, history of abdominal or pelvic surgery, American Society of Anesthesiologists score (ASA), and body mass index, were analyzed.
Operative variables, including operating time, change in serum creatinine concentration, change in hemoglobin levels, conversion to open surgery, skin incision length, postoperative hospital stay, postoperative retention time of catheterization, visual analogue pain scale (VPS), and oral analgesic dose were analyzed. Clavien classification of surgical complications was used to grade postoperative complications.
Oncological outcomes, including tumor size, tumor location, pathological stage, tumor grade, margin status, and tumor recurrence, were analyzed. The 2002 TNM staging system was used to classify the tumor, and tumor grades were classified according to the 2004 WHO classification. Data were presented as mean ± standard error of the mean. All data were compared using the Mann-Whitney U test, T test for continuous variables, and χ2 test for categorical variables. Statistical analysis was conducted using SPSS Statistics software version 24.0.
Results
According to Table I, a significant difference was found in patients’ gender (p = 0.037). No significant differences in demographics were noted between the two groups. None of the patients had any previous abdominal or pelvic surgery. In comparison with the RL-NU group, a LESS-NU group patient required more trocars during the operation because of obesity. However, the mean operation time of the LESS-NU group was significantly shorter than that of the RL-NU group (p = 0.006). The mean skin incision length was also shorter in the LESS-NU group (p < 0.001). Additionally, the mean VPS of LESS-NU was significantly lower than that of the RL-NU group (p < 0.001).The LESS-NU group patients required fewer oral analgesics than the RL-NU group patients. Overall, no significant difference was found in the change in serum creatinine concentration and hemoglobin levels between the two groups (p = 0.838 and p = 0.14, respectively). No significant differences were also found in postoperative hospital stay (p = 0.797) and in postoperative retention time of catheterization (p = 0.805) and ASA score (p = 0.612). Postoperative complication syndrome occurred in 11 patients (LESS-NU, n = 7; RL-NU, n = 4). Four patients who belonged to the LESS-NU group had fever after surgery, and one patient in the LESS-NU group suffered abdominal pain. In the RL-NU group, pneumonia was handled with a conservative anti-infection treatment, and two other patients had postoperative fever. All these cases were resolved with conservative management.
Table I
Patient demographics and operative variables of LESS-NU and RL-NU
| Parameter | LESS-NU (n = 25) | RL-NU (n = 17) | P-value* |
|---|---|---|---|
| Gender, n (%): | |||
| Female | 8 (32) | 11 (64.71) | 0.037 |
| Male | 17 (68) | 6 (35.29) | |
| Age, mean (SD) [years] | 67 (9.24) | 69.12 (9.28) | 0.626 |
| BMI, mean (SD) [kg/m2] | 22.26 (5.38) | 25.28 (4.85) | 0.063 |
| ASA score, n (%): | |||
| 1 | 11 (44) | 6 (35.29) | 0.612 |
| 2 | 12 (48) | 8 (47.06) | |
| 3 | 2 (8) | 3 (17.65) | |
| Previous abdominal or pelvic surgery, n | 0 | 0 | |
| Operating time, mean (SD) [min] | 204.4 (36.26) | 236.18 (24.41) | 0.005 |
| Change in serum creatinine concentration, mean [mg/dl] | 8.87 | 9.57 | 0.838 |
| Change in serum hemoglobin level, mean [g/dl] | 11.84 | 19.64 | 0.140 |
| Postoperative retention time of catheterization, mean [days] | 3.88 | 3.76 | 0.327 |
| Surgery conversion, n (%) | 1 (4) | 0 | |
| Skin incision length, mean (SD) [cm] | 2.88 (0.43) | 5.94 (2.63) | < 0.001 |
| Visual analogue pain scale, mean (SD) | 2 (0.57) | 3.76 (1.06) | < 0.001 |
| Oral analgesic dose, mean (SD) [days] | 1.12 (0.65) | 2.75 (0.82) | < 0.001 |
| Intraoperative complications, n (%) | 0 | 0 | |
| Postoperative complications, n: | 0.849 | ||
| Grade 1 | 5 | 3 | |
| Grade 2 or > 2 | 0 | 0 |
All the 42 patients had confirmed UTUC based on the pathological results. The major tumor was in the T3 stage (n = 20, 47.62%) according to Table II. Low tumor grade was observed in 6 (14.29%) patients. One pN2 nodal status and one positive margin status were both noted in the RL-NU group. No significant differences were obtained in the pathological characteristics between the two groups.
Table II
Oncological characteristics
The mean follow-up was 31.64 months, and no significant difference was observed between the two groups (Table III). Among the 33 continuous follow-up patients, two patients died during our follow-up period. Both patients were in the RL-NU group, including the pN2 patient. The pN2 patient died of pelvic metastasis 15 months after the operation. Another patient also died of a cancer-related cause after the 1-year follow-up. Overall, recurrences occurred in 8 patients, and no difference was observed between the two groups.
Table III
Follow-up outcomes of patients in two groups
Discussion
The conventional open nephroureterectomy (ONU) procedure, which is the earliest method of surgery, requires a lumbar incision at the affected side [14]. The kidney and middle and upper ureter were resected through the incision. Then, another large McBurney incision at the affected side was made to resect the distal ureter and bladder cuff. However, this method has been replaced by several minimally invasive procedures because of its wound disadvantage. Since Clayman et al. reported the first successful laparoscopic nephroureterectomy in 1991, minimally invasive approaches have been performed in urological surgery [15]. In recent years, the retroperitoneal approach has become more beneficial than the other approaches [16] and has become a major conventional surgical procedure to treat UTUC. Surgeons prefer to maximize the clinical effect with minimal invasiveness. LESS-NU surgery was introduced as a novel and safe procedure. Our department began to perform LESS in 2009 [10, 11]. Sufficient clinical experience has been accumulated in recent years.
In this study, we designed a modified LESS-NU procedure and made a comparison with the RL-NU procedure in our department. Through this method, we tried to compare the advantages and disadvantages between modified LESS approach and retroperitoneal approach. To our knowledge, this report is the first analysis of these two procedures on the management of UTUC.
On the management of the surgical procedure, many institutions have reported their own modifications and innovation [17, 18]. By summarizing our previous experience, we agreed that separating the renal pedicle was the key step. First, the paracolic sulci needed to be separated as much as possible. The colon would slide downward under the action of gravity. At this moment, the renal hilum would be exposed maximally. When isolating the renal vein, the vein should be bared in parallel with the renal vein path. And, blunt separate and sharp separate could be combined to separate the surrounding tissue. When producing the right side, the fourth channel on the single port can be used to protect the low edge of the liver, vena cava, and duodenum. In our current series, we were able to separate the kidney and dissect the ureter down the bladder cuff region. Additionally, the V-loc suture can be chosen to close the bladder cuff without knotting. It is a direct method to handle the problem of knotting. In the largest multi-institutional series, Park et al. showed that their mean operation time was 221 min [19]. In their series, 20.8% of the cases were performed without bladder cuff excision. In the latest LESS-NU study, Tsivian et al. had a mean operation time of 217 min [20]. In the present series of 25 LESS-NU cases, the mean operation time was 204.4 min, which was shorter than those of the above studies. By contrast, all patients in the RL-NU group needed to be repositioned during the operation. It potentially wasted 20–30 min of operating time for altering the patient’s position, disinfecting, and toweling.
Based on the previous description [12, 13], our RL-NU procedure managed 3–4 ports on the waist. Incisions may be extended to 5–7 cm for specimen extraction. The length of incision was mainly related to the patient’s postoperative pain. In our LESS-NU group, we chose the umbilicus as this single port, because the tissue surrounding the umbilicus was thin. All procedures, such as kidney and ureter dissection, distal ureter and bladder cuff excision, and bladder closure, were performed via this port. It meant that injuries to the abdominal wall and the postoperative pain could be reduced. Identifying the anatomical sign and obtaining a clear operative view were easily done by settling a pneumoperitoneum. Additionally, the use of a flexible single port could ease the manipulation through the transumbilical approach. Owing to the small incision and little tension around the umbilical port, the 3-0 absorbable sutures could be used to make intermittent suture or running suture. Sutures that would reduce the length of stay need not be removed. Due to the umbilicus being a natural fold part of human body, the wound surrounding the umbilicus was inconspicuous. A “scarless” procedure was partially accomplished by the transumbilical LESS procedure. In the present series, the mean incision length of LESS-NU patients was 2.88 cm. By contrast, a 8.94 cm mean large lower abdominal oblique incision was required in the RL-NU group. It was a huge improvement in the management of the operation wound.
At the same time, the size of the wound could directly affect the patient’s postoperative pain. Bansal et al. also agreed with the potential cosmetic benefits of this minimally invasive surgery [21]. According to our analysis, the length and number of skin incisions had a positive correlation with the VPS and oral analgesic dose. This result was in accordance with some previous reports. Fan et al. found that owing to the obvious reduction of the surgical wound, the postoperative pain would be significantly reduced compared with the traditional laparoscopic surgery [5]. In our study, patients in the LESS-NU group required an oral analgesic for 1 or 2 days. However, patients who underwent RL-NU required more oral analgesic due to the large wound. The reduction of the postoperative pain is helpful to evaluate the postoperative patient’s recovery and predict the postoperative complications. During our follow-up, some patients who underwent RL-NU reported ongoing pain on their wounds for almost 1 month after the operation despite the recovery of the wound. Faint pain was also reported on rainy days. In the LESS-NU group, a few patients felt pain after leaving the hospital. Overall, the patients were more satisfied with the LESS-NU for its advantages of postoperative recovery and less pain. Olweny et al. firstly evaluated the patients’ perceptions of the scarring relative to other surgical outcomes [22]. Current patients paid more attention to hospitalization experience, scar length, postoperative cosmetic effect, and postoperative quality of life. The LESS-NU procedure met these patients’ needs.
Interestingly, we found a significant difference in gender. However, the population of women choosing LESS-NU per year increased. With the development and maturity of our LESS-NU technique, more women favored the LESS-NU procedure. UTUC is more popular in female patients (55.4%) than male patients (44.6%) in China [23]. We agreed that LESS-NU would be a perfect choice for female patients because of its better cosmesis and less pain.
In our follow-up period, 33 patients continued reviewing our series until we finished this report. Connections with the nine other patients were lost because of their missing phone numbers or moving to other places. The mean follow-up time was 31.64 months. During this time, 2 patients died of cancer-related causes in the RL-NU group. A patient was pathologically confirmed with pT3 N2 cMo status. When this patient left the hospital for 6 months, he had a confirmed pelvic metastasis. Another patient was diagnosed with bone metastasis. Additionally, 10 metastasis cases were checked. These metastasis patients were still alive and receiving chemotherapy actively. For the short-term review, LESS-NU attained the same achievement as the RL-NU procedure.
The limitations of our study should be noted. The study was limited by its relatively small retrospective sample size, and patient selection between LESS-NU and RL-NU was not randomized. The benefits of LESS-NU should be demonstrated through a large number of trials, and oncology outcomes should be analyzed by conducting a long-term follow-up review. Despite the limitations, this study is still the first to make the comparison between the modified LESS-NU and RL-NU. Meanwhile, we introduce a modified, minimally invasive technique. We believe that our experience will attract more surgeons to perform our modified LESS-NU and help patients benefit from this technique.