





The use of a fibreoptic bronchoscope to facilitate endotracheal intubation via the oral or nasal route is well established in modern anaesthetic practice and undertaken in both awake (sedated) and anaesthetised patients [1, 2]. However, when inserting an endotracheal tube (ETT) over the fibreoptic bronchoscope, the bevel tip can impinge on the right arytenoid, inter-arytenoid tissue, vocal cords or epiglottis, which might impede advancement of the ETT through the laryngeal inlet. This difficulty can result in repeated intubation attempts and increased risk of oedema, airway injury and failed intubation. These problems can occur regardless of the experience of the practitioner [3–5]. Laryngeal impingement or hold-ups have been reported to occur in up to 90% of orotracheal fibreoptic intubations (OFI) and the difficulty can be as difficult as nasal fibreoptic intubation [4]. The complication of impingement has also been reported to cause various types of airway injury [6, 7].
Several techniques such as anticlockwise tube rotation and the design of a tapered tip and a bevel of the tracheal tube have been suggested to enhance the successful railroading of the tracheal tube [8–10]. Moreover, the choice of ETT can also facilitate railroading and potentially reduce the risk of laryngeal impingement [11]. The Parker flex tip (PFT) tracheal tube (Parker Medical, Inc, Connecticut, USA) has a flexible, curved, centred and tapered distal tip that is designed to facilitate rapid and easy non-traumatic intubation. When this unique tube is advanced into contact with the protruding structures of the airway, its tip can flex and slide gently past them and prevent it from getting stuck in the airway, resulting in trauma to the tissue [12, 13].
The unoflex reinforced (URF) tracheal tube (ConvaTec Inc, Tredegar, UK) is a wire-reinforced ETT which is an effective device for facilitating railroading during fibreoptic intubation. It has been previously suggested that a wire-reinforced tube may be easier to pass through the orotracheal airway than a polyvinylchloride tube due to its flexible nature and its larger obtuse distal angle [14].
Very few previous studies have compared the PFT ETT with a wire-reinforced ETT for OFI. To the best of our knowledge, only one study has compared these two types of ETTs, but it was not in simulated difficult airway patients [15]. Hence, the present study was conducted to compare the PFT ETT and the UFR ETT during OFI in simulated difficult intubation patients to evaluate the ease of insertion (smoothness of ETT advancement into the trachea without any resistance or impingement), degree of manipulation (based on the Jones classification), time to intubation, post-operative sore throat, bleeding from the oral cavity and haemodynamic changes. The outcome of the study would potentially provide additional information for the option of ETT for successful OFI in difficult airway patients, particularly those who might have restricted neck movement such as in cervical spine fracture or cervical spine pathology.
METHODS
This single-blinded, randomised controlled trial compared the types of ETT used during OFI. After receiving approval from the Human Research Ethics Committee at Universiti Sains Malaysia (approval code: USM/JEPeM/16060212) and written informed consent from the patients, we recruited 58 elective surgical patients who fulfilled the inclusion and exclusion criteria during the pre-operative assessment. The inclusion criteria were American Society of Anesthesiologists (ASA) classification I–II, age of the patients ranging between 18 and 65 years, duration of surgery within six hours and cases that were planned for the oral route of intubation. The exclusion criteria were potential difficult airway on assessment, previous history of airway and cervical surgery, a known case of hypertension, morbid obesity and pregnancy.
All the selected patients were randomised to two groups using computer-generated randomisation. The PFT group was intubated with the PFT ETT (n = 29) and the UFR group was intubated with the UFR ETT (n = 29). The allocation number was concealed in a sealed envelope, and it was only opened on the day of the study by an assistant nurse prior to ETT preparation. All the patients were given premedication with oral midazolam 7.5 mg on the night prior to surgery and prior to the operating theatre (OT) call.
In the OT, an 18 G or 20 G intravenous (IV) cannula was inserted and non-invasive monitoring devices, such as electrocardiogram (ECG), pulse oximetry (SpO2), capnography and non-invasive blood pressure (NIBP), were put in place. The fibreoptic scope (Storz flexible fiberscope-4 mm OD, 60 cm length (Karl Storz Endoscopy Inc., Berlin, Germany) was prepared prior to the procedure, and the type of ETT was railroaded and loosely fixed at the proximal part of the scope. In the PFT group, either a 7 mm, 7.5 mm or 8 mm PFT ETT was used. In the UFR group, either a 7 mm, 7.5 mm or 8 mm UFR ETT was used. The choice of ETT size was based on the standard physical build in our population and the gender of the patient, which was commonly either size 7 mm or 7.5 mm for female and 7.5 mm or 8.0 mm for male patients.
After pre-oxygenation with 100% oxygen for 3 min, all the patients were induced with IV propofol 2 mg/kg and IV fentanyl 2 µg kg-1. After successful induction, a cervical neck collar was subsequently applied to simulate the difficult airway condition, and anaesthesia was maintained with sevoflurane 2–3% with 100% inspired oxygen. Once adequate mask ventilation was established, IV rocuronium 0.6 mg kg–1 was administered as a muscle relaxant and IV glycopyrrolate 200 µg was administered as an anti-sialagogue. After the establishment of complete muscle relaxation as determined by single twitch neuromuscular monitoring, OFI was initiated with a jaw thrust manoeuvre to obtain a view of the glottis and to advance the tube into the trachea via the vocal cords. Once the carina was seen on the screen, the preloaded ETT was railroaded into the trachea. The fibreoptic intubation and the railroading of the tube were performed by a a similarly experienced practitioner where the same persons performed all the fibreoptic intubations as well as advancement of the tube. The practitioner was a senior trainee in anaesthesiology who had more than 5 years of experience in anaesthesia practice and had undergone theoretical as well as practical training in fibreoptic intubation. The training session included hands-on practice to the manikin and to at least 10 patients under close supervision and guidance from a consultant. If any impingement occurred, the steps of the manoeuvre were attempted based on the Jones classification (Table 1). If the SpO2 level dropped to less than 95%, the procedure was stopped temporarily, and the patient was manually ventilated again until the SpO2 value improved. The next attempt was labelled as the second attempt; if it was still unsuccessful, the cervical collar was removed, and the patients were subsequently intubated using conventional laryngoscopy. The attempt for repeat check of OFI was restricted to only once before conversion to conventional laryngoscopy. Patients with failed fibreoptic intubation were omitted from the statistical analysis.
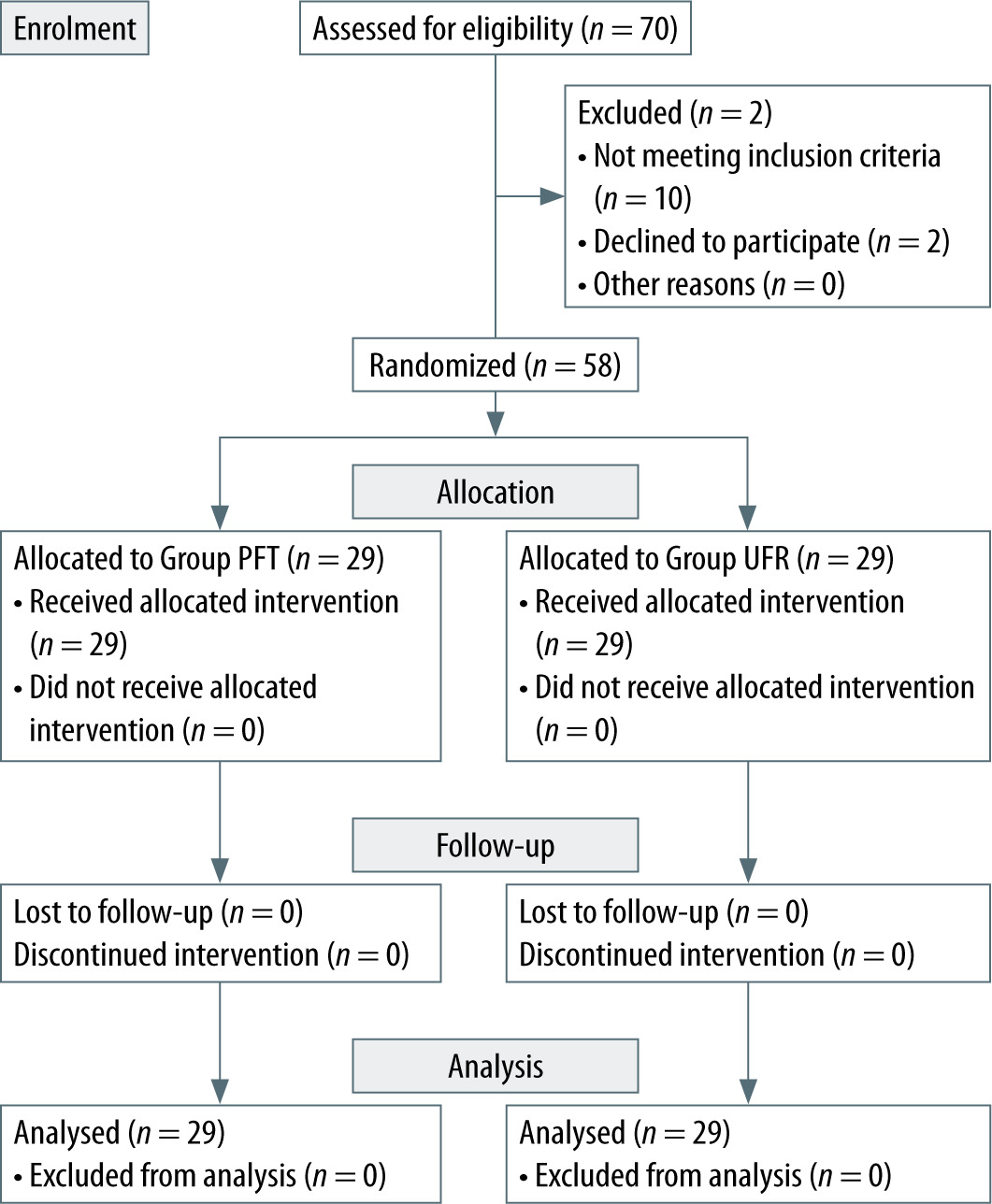
TABLE 1
Jones classification of degree of manipulation
After successful fibreoptic intubation and railroading of the ETT, a Yankauer suction tip was used to determine any blood-stained aspirate. Haemodynamic parameters mainly mean arterial pressure (MAP) and heart rate (HR) were recorded using NIBP and ECG at baseline before intubation, after 1 min and after 5 min of successful OFI and railroading of ETT by the anaesthesia assistant. The time taken for OFI until successful railroading and the scoring of sore throats based on the visual analogue scale (VAS) were also recorded 30 min postoperatively.
Sample size was calculated using Power and Sample Size software version 3.0 (January 2009, 1997–2009, Dupont WD and Plummer WD) based on a previous study by Barker et al., in which p0 is taken as 0.01, p1 as 0.333, m = 1 with α = 0.05 (type 1 error) and power of 0.9 [16]. Based the sample size calculation, 26 subjects were required, and after taking into consideration a 10% dropout rate, in our study, each group consisted of 29 subjects; thus, the total sample was 58.
Data were analysed using SPSS software version 24.0 (IBM Corp., NY, USA). Ease of insertion, degree of manipulation and bleeding and sore throat complications were analysed using the c2 test. Time for intubation was analysed using the independent t-test. The haemodynamic parameters were analysed using repeated measures analysis of variance (ANOVA). P < 0.05 was considered statistically significant.
RESULTS
There was no significant difference in the demographic data between the two groups (Table 2). The intubation profiles, which consisted of the number of intubation attempts, the degree of manipulations (according to the Jones classification) and the time of intubation, were also not significant between the two groups (Table 3). The success rate of intubation was 100% in both groups. No procedure needed to be stopped due to a fall in oxygen saturation. Ease of intubation was not significant and comparable in both groups (69.0% vs. 62.0%; P = 0.599). The degree of manipulation was also not significant and comparable between the two groups (69.0% vs. 62.1%; P = 0.849). Time of intubation was also not significantly different between the two groups (56.9 s ± 39.7 s vs. 63.9 s ± 36.9 s; P = 0.488).
TABLE 2
Demographic data
TABLE 3
Intubation profiles between Parker flex tip (PFT) and Unoflex reinforced (UFR)
There were no significant differences in the sore throat score and complication of bleeding between the two groups (Table 5). The percentage of bleeding from suctioning was not significantly different between the two groups (17.2% vs. 6.9%; P = 0.227). There were no significant differences in the haemodynamic parameters between the two groups (Table 4).
TABLE 4
Comparison of mean (95% CI) of mean arterial pressure (MAP) and heart rate (HR)
DISCUSSION
The flexible fibreoptic scope is a valuable instrument for performing difficult intubation. However, successful placement of the fibreoptic scope in the trachea does not ensure successful passage of the tube into the trachea [3, 13, 16]. Furthermore, repeated attempts at passage may result in airway bleeding, damage to the arytenoid cartilages or epiglottis or swelling of the airway, which leads to more difficult intubation on subsequent attempts [3–5, 17]. The choice of ETT is another factor that can influence successful intubation during OFI. Our study showed that the PFT ETT and the UFR ETT are comparable in terms of the number of attempts, ease of insertion, degree of manipulation, time of intubation, haemodynamic parameters and complications.
To the best of our knowledge, only one previous study has compared these two types of ETTs for OFI. Jafari et al. [15] conducted a study to compare the PFT ETT to a wire-reinforced (WR) tracheal tube in two orientations of bevel – posteriorly and anteriorly positioned tip bevels (WRP and WRA groups, respectively) – during OFI in 90 patients who were scheduled to undergo either ophthalmic or urologic surgery. The results showed that ETT advancement was easier and faster in the WRP and PFT groups than in the WRA group [15]. In that study, successful endotracheal intubation on the first attempt was 67%, 60% and 20%, respectively; P = 0.03. The ETT advancement time was 6.9 s ± 3.5 s, 8.0 s ± 3.1 s and 11.7 s ± 4.6 s, respectively; P < 0.001. In our study, the success rate on the first attempt was 100% for both groups. However, only 62% of the patients from the PFT group and 69% from the UFR group had easy insertion during railroading of the ETT; moreover, the time to successful intubation was comparable, 56.9 s ± 39.7 s vs. 63.9 s ± 36.9 s, respectively. Jafari et al. [15] concluded that advancement of the ETT over a fibreoptic bronchoscope was easier with the PFT tube and with a WRP tube than with a WPA tube.
Some previous studies have compared the PFT tube with the standard ETT; they showed that PFT had reduced resistance for tracheal intubation and a lower impingement rate than the standard ETT [13, 18]. One study reported a 100% success rate with the first attempt at railroading, while others reported a success rate of 91%, 89% and 76%, respectively [13, 16, 18, 19]. However, other studies reported that the PFT insertion rate was not statistically significant in terms of ease of railroading, which was similar to the findings from our study [3, 20]. In terms of the UFR tube, the success rate of intubation during first attempt was also 100%. However, only 69% did not require any manipulation. Previous studies have also shown that the success rate for a flexometallic tube was also 100% but the percentage of no manipulation was 46.7–66.0%. The flexometallic tube had a more rounded bevel to facilitate intubation, but when compared to the ETT used for an intubating laryngeal mask which had a rounded bevel as well as a tapered tip, the flexometallic tube showed a significantly higher percentage of ETT manipulation requirement [16, 17].
In our study, the ease of insertion was 62% and 69% for the PFT and UFR groups, respectively (P = 0.599). Although more of the patients in the UFR group did not require any manipulation in comparison to the patients in the PFT group, the difference was not statistically significant (P = 0.849). A study done by Barker et al. showed that, for nasal fibreoptic intubation, insertion was easier with the PFT than the Mallinckrodt reinforced tube. The Jones classification 0 was n = 15 and n = 9 respectively (P = 0.034) [16]. A study by Kristensen using PFT ETT and a Portex tube for OFI also showed that the ease of insertion was better for the PFT ETT and the difference was statistically significant (P < 0.01) [13]. Our study investigating oral fibre-optic intubation showed that the ease of railroading was comparable for the PFT ETT and UFR ETT.
In our study, time to successful intubation was calculated from the beginning of the OFI to the successful railroading of the study tube into the trachea and confirmation of the tube in the trachea by visualising the carina. Mean intubation time was 63.9 s for the PFT tube and 56.9 s for the UFR tube (P = 0.488). This finding was similar to the results reported in a study by So et al., which found that using the PFT tube did not result in a statistically significant reduction in the time to intubation [12]. However, a study by Kristensen reported that the time for intubation was shorter for the PFT tube, 7.5 s in comparison to 20 s for a conventional tube, which was half of the time required [13]. Lomax et al. reported that the median (IQR [range]) time to intubation was comparable between a PFT nasal tracheal tube (GlideRite) and a pre-rotated RAE nasal tube (7.6 (4.7–10.8 [3.0–46.2]) s vs. 8.0 (6.2–10.7 [2.4–30.0]) s, respectively) during nasal fibreoptic intubation, which was a shorter time than our result [3].
In a previous study, overall, the incidence of post-intubation sore throat was 63.9%.[21] Cochrane database review incidence ranged from 30% to 70% [22]. Previous studies reported that PFT did not decrease the incidence of sore throat, which is similar to the finding of our study (P = 0.483) [17, 19]. Mean VAS score (range: 0–10) was 1.52 and 1.28, respectively, for PFT and UFR. The aetiology of post-operative sore throat is likely to be multifactorial. Thus, it is partially related to ETT and perceived trauma during ETT insertion. There is also a lack of correlation between multiple attempts at intubation and sore throat development. The duration of the presence of ETT also affects the incidence of sore throat, as does the amount of intraoperative analgesics used. A duration of more than 90 min was reported to significantly affect post-operative sore throat [21]. Insertion into the Guedal airway might also affect the sore throat score. One study showed that the use of PFT resulted in a less severe sore throat in comparison to the standard ETT [18]. Our study showed that 17.2% of the patients in the PFT group had bleeding from the oral cavity in comparison to 6.9% of the patients in the UFR group. The duration of surgery for both groups was within six hours and the duration of surgery might not affect the difference in incidence of sore throat between the two groups. This finding was similar to the results reported in a study by Timothy et al., which found no significant difference in oropharyngeal bleeding between the PFT tube and the standard tracheal tube [19].
In terms of haemodynamic changes, few previous studies have reported significant changes in the haemodynamic parameters between fibreoptic intubation and conventional intubation [23, 24]. Our study was designed to compare the haemodynamic changes between two types of tubes both inserted by OFI. We found no significant differences in MAP (P = 0.361) and HR (P = 0.152) between the PFT tube and the UFT tube. There was no previous study comparing the haemodynamics between these two types of tubes. A study that compared the cardiovascular responses during awake nasotracheal intubation using a fibreoptic bronchoscope and a blind intubation device showed significant increases in both blood pressure and HR compared with baseline or postsedation values. Both techniques used a wire-reinforced tube for intubation. However, no significant difference was found between the two groups [25].
Our study had some limitations. It was designed as a single-blinded study that was performed in simulated difficult airway patients. It would be better if the comparison could be double-blinded, but doing so would be difficult; this obstacle was also encountered in several other studies [3, 5, 11]. Moreover, we designed this study of a simulated difficult airway condition for OFI during general anaesthesia, which might not accurately reflect an actual difficult airway patient for awake OFI. In terms of the incidence of post-operative sore throat, our study did not consider the duration of ETT in situ and the use of analgesia as other influencing factors.