





Choosing an optimal postoperative analgesia modality after total knee arthroplasty (TKA) plays a major role in the early postoperative period. Early rehabilitation is possible in the situation when the pain is reduced to the minimum. Thus pain management using the methods of femoral nerve block promotes function restoration in patients after TKA [1]. The method of local anesthetic infusion still remains the subject of investigation for many authors [2]. The continuous infusion reduces pain after the surgery; it may, however, be inadequate during increased activity of the patient, for example during the physiotherapy sessions. An additional possibility of administering the boluses of a medication using the patient-controlled regional analgesia (PCRA) system could allow the patient to react in case pain occurs or becomes more intense directly before the exercises, or it could intensify physiotherapy procedures as they last. The majority of authors emphasize that the best way to use local anesthetics in the form of an infusion has not been indicated as yet [3]. There is no sufficient evidence showing the superiority of any particular method of continuous perineural infusion over others. An attempt to identify the ideal method of continuous infusion of local anesthetics should consider not only its effect on pain reduction in the early postoperative period, but also the possibility of increasing motor blockade with any kind of infusion used [4, 5].
The aim of the study was to assess the effectiveness of CFNB with elastomeric pump by means of PCRA combined with basal infusion to manage pain in the early postoperative period following TKA and to compare it with the method of continuous infusion as well as with treatment consisting only of intravenous morphine analgesia. Moreover, the effect of the two methods on opioid consumption, the incidence of adverse effects and the possibility of functional restoration after the surgery were compared.
METHODS
The prospective randomized controlled trial (Approval of Bioethics Committee of the Medical Faculty of the University of Warmia and Mazury in Olsztyn N23/2014, 25/06/2014) included 90 patients after TKA assigned randomly to three groups (Figure 1).
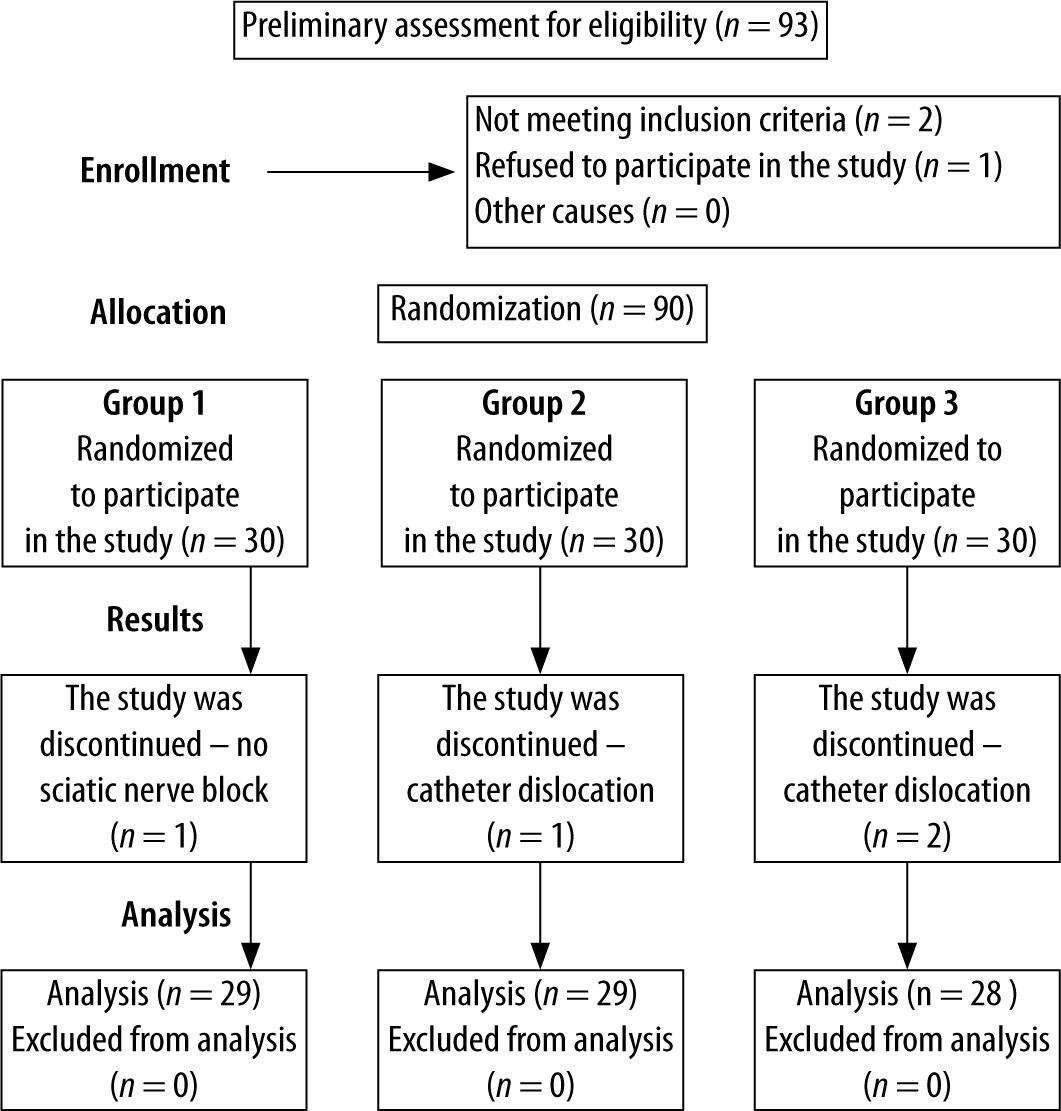
Patients were randomized to groups I–III by using a website (http://www.randomization.com) and a computer-generated table of unallocated numbers, thus determining who would receive CFNB continuous infusion plus bolus, only CFNB continuous infusion or be excluded from CFNB and receive intravenous morphine infusion. The inclusion criteria were ASA I–III adult patients scheduled for elective TKA due to gonarthrosis.
Exclusion criteria were as follows: refusal to participate in the study, neuropathy, puncture site infection, coagulopathy, surgical revision of TKA, TKA due to trauma, abuse of opioids. Group I was the control group. The patients in this group received intravenous morphine. The patients in this group did not receive CFNB. Sham CFNB was not applied due to ethical issues. Patients randomized to group II had standard CFNB [6] performed under ultrasound guidance with 0.2% ropivacaine as continuous infusion 5 mL h-1. Group III consisted of patients who received CFNB as an infusion of 0.2% ropivacaine 5 mL h-1 combined with additional boluses of 0.2% ropivacaine at a dose of 5 mL injected by the patient in case of pain, as a patient controlled regional analgesia technique. Ropivacaine infusion in groups II and III was provided by an elastomeric pump (Infusor LV5, Baxter International Inc.). The total dose of ropivacaine in the elastomeric pumps in groups II and III was 600 mg (300 mL of 0.2% ropivacaine). After 60 hours the pump was disconnected and the catheter was removed. The number of boluses and time of emptying of the pump in group III were not measured. As intraoperative anesthesia all the patients received spinal anaesthesia with 15 mg of 0.5% hyperbaric bupivacaine plus 10 µg of fentanyl and single-shot sciatic nerve block in the popliteal fossa with 30 mL of 0.375% ropivacaine. CFNB with Contiplex Tuohy Ultra, B. Braun Medical Inc. was performed before spinal anesthesia with the ultrasound method using the in-plane technique in short-axis (BK Medical Flex Focus 800 linear probe 12–15 MHz). The femoral nerve was localized in the inguinal ligament area laterally to the femoral artery. The catheter was inserted 3 cm beyond the needle G18 and its localization was confirmed. Then the catheter was secured with sterile dressing and 10 mL of 0.375% ropivacaine was given. In case of pain of intensity of more than 3 on a numerical rating scale (NRS) the patient received 5 mg of morphine intravenously. Paracetamol 4 γ per day and ketoprofen 200 mg per day orally in the divided doses were given in all the groups as an additional pharmacotherapy. All the patients gave their informed consent to participate in the study.
The treatment efficacy consisted of assessment of pain using the NRS scale, consumption of morphine (mg per day), patient satisfaction after the surgery, the incidence of adverse effects and the effect of each method on the possibility of functional restoration after the surgery. The assessment of functional outcome after the operation was conducted by evaluating the range of motion (ROM) in the knee joint measured with a goniometer, in degrees, as well as measuring the distance covered in meters. The patients were monitored for 96 hours after TKA. Patient satisfaction was assessed with a questionnaire that included a 3-point scale: satisfied, partially satisfied, unsatisfied.
The statistical analysis was performed using the SPSS Statistics software package (version v19).
The significance threshold adopted for the analysis was α = 0.05. The results of the Kolmogorov-Smirnov normality test were used to assess the distribution. In order to compare the independent groups for variables with normal distribution Student’s t-test for independent samples was used, while the Mann-Whitney U test was used for the variables with non-normal distribution. In order to compare the differences between the independent groups for qualitative variables the χ2 test was conducted.
RESULTS
There were no differences between the groups in terms of demographic data (Table 1). Group III showed a lower intensity of pain (Figure 2), a smaller opioid consumption (Figure 3), better functional restoration with a greater ROM in knee joint and a greater distance covered (Figure 4), as well as a smaller nausea rate when compared with other groups (Table 2). No statistically significant difference was noted between the groups in terms of other adverse effects. The rate of catheter dislocation was 7%. Statistical significance in satisfaction was revealed between group III and group II at 24 and 48 hours after surgery (P = 0.01) with greater satisfaction in group III, as well as between group III and group I at 24, 48 and 72 hours after surgery (P = 0.01) also with greater satisfaction in group III. Moreover, statistical significance was found between group I and group II at 24 and 48 hours after surgery (P = 0.01) with greater satisfaction in group II.
TABLE 1
Results for basic demographic variables. The differences between the groups are statistically non-significant
FIGURE 2
Comparison of pain intensity on NRS in the three groups
*P < 0.005
NRS – numerical rating scale
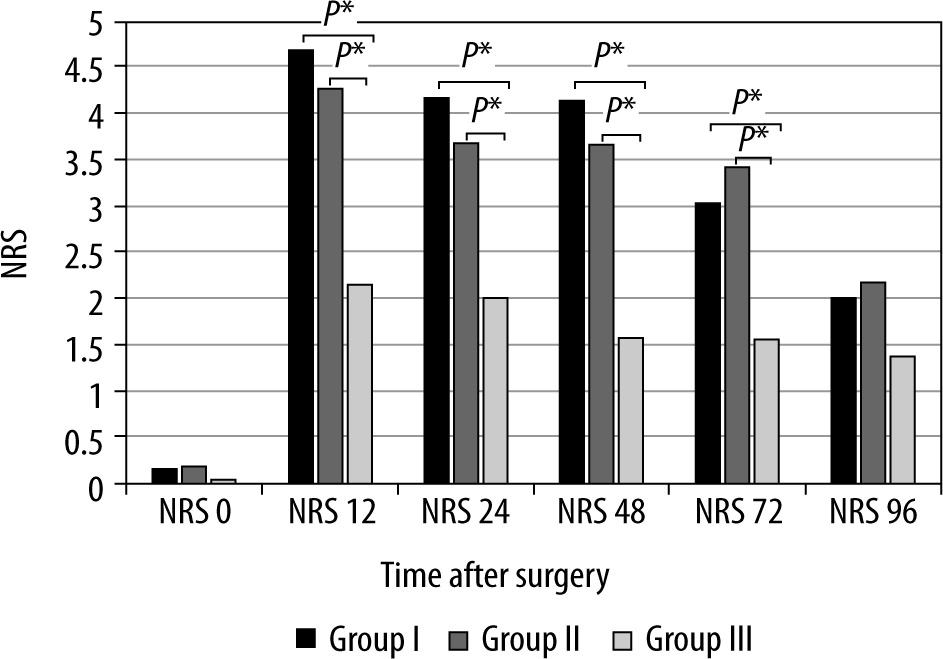
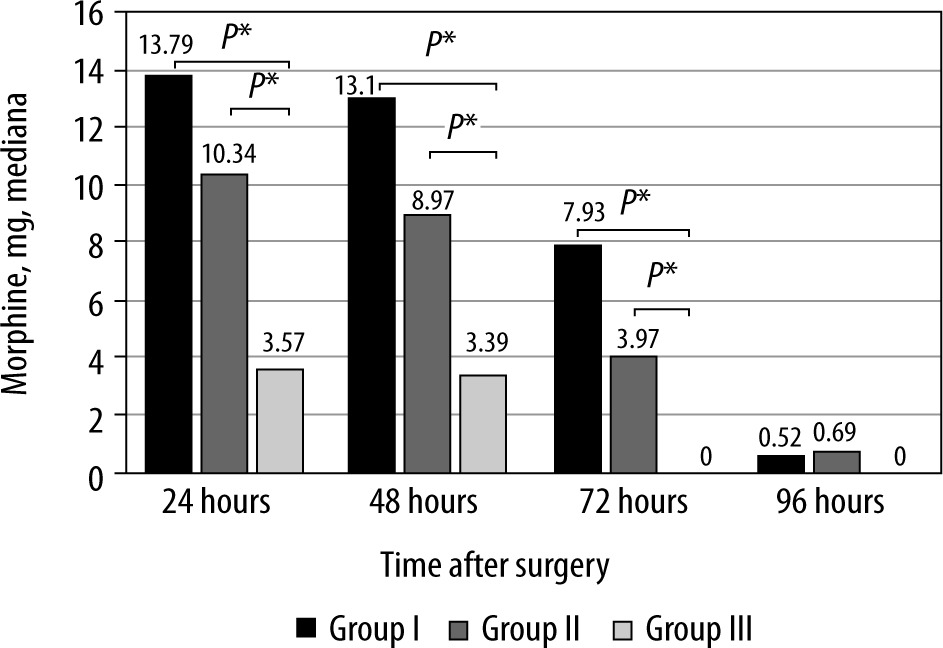
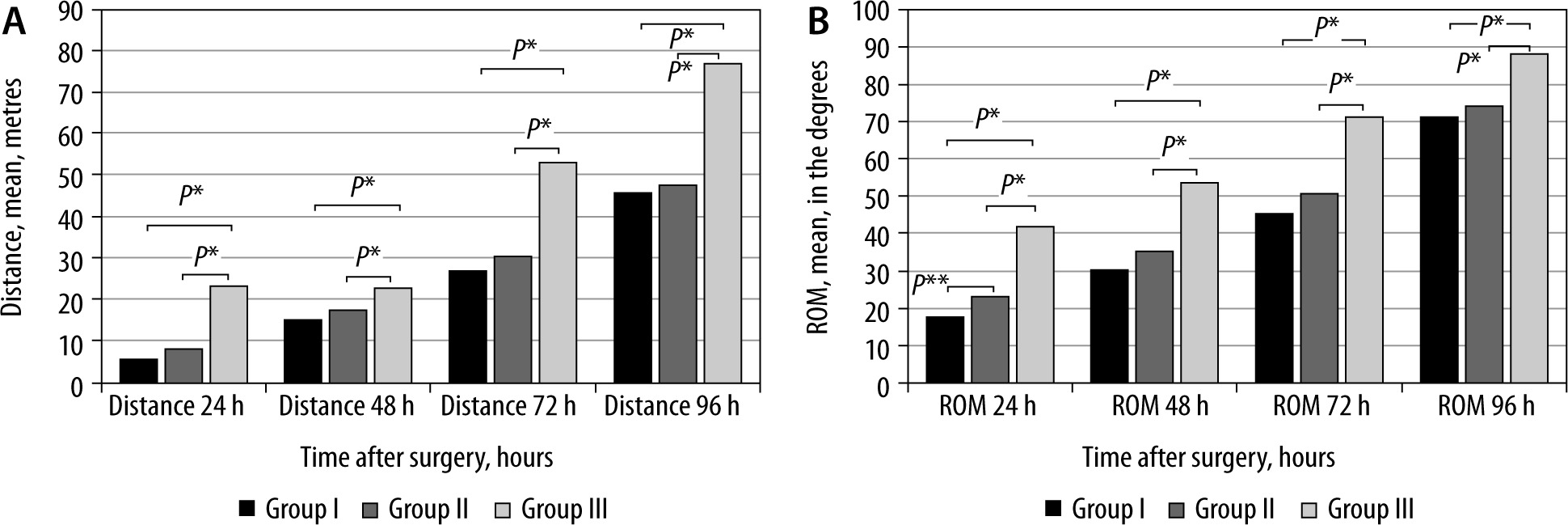
FIGURE 4
Evaluation of range of movement in the knee joint and covered distance. ROM – range of movement in degrees in the knee joint in the degrees. Distance in the meters
*P < 0.005, **P = 0.019
DISCUSSION
In this prospective randomized trial greater efficacy of CFNB with 0.2% ropivacaine infusion at the rate of 5 mL h-1 plus 5 mL bolus versus CFNB as continuous infusion without additional boluses was demonstrated in patients after TKA. This superiority consisted of reduced pain intensity and opioid consumption, better functional restoration and a lower rate of nausea in the group of patients who had CFNB continuous infusion plus boluses. The study did not demonstrate an advantage of continuous infusion of 0.2% ropivacaine over the group without CFNB. As the number of TKA procedures performed worldwide over the past few decades is growing, there is considerable interest of anesthesiologists and clinicians in the patient’s condition during the postoperative period following TKA [7]. There is an ongoing search for an adequate method of pain management after TKA [8, 9]. Possible advantages of continuous peripheral nerve blocks (CPNB) are the possibility of using this method for a few days and not only for several hours following the surgery and a lack of analgesic effect with a single injection after the blockade resolves. The use of CPNB lowers the NRS score of the most intensive pain as well as pain at rest on days 1, 2 and 3 following the surgery in comparison with the group treated with a single-injection peripheral nerve block [10]. Our results correlate with this evidence.
The study compared two methods of local anesthetic infusion: continuous infusion versus bolus administration combined with continuous infusion. Pain intensity was lower in the group treated with local anesthetic infusion plus bolus, which indicates greater efficacy of the method in which boluses were administered as top-ups to the continuous infusion. Such a method of analgesia makes it possible for the patient to self-administer a bolus immediately on pain occurrence. A basal continuous infusion of a local anesthetic was found to reduce the incidence of breakthrough pain and to improve the quality of sleep [11]. Addition of self-administered boluses considerably improves analgesia, making it possible to reduce the rate of basal infusion and greatly decrease the consumption of opioids as well as to diminish the incidence of adverse effects of opioids [3]. In our study a continuous infusion of 5 mL h-1 was used in both groups. Similar rates of infusion, as well as boluses or lockout time, are recommended by many authors that bring up the topic of CFNB [3, 10, 11]. Increased satisfaction in patients using PCRA may result from reduced use of opioids, which are characterized by a high incidence of adverse effects such as nausea, vomiting, and itchiness [7]. Elastomeric pumps are more widely used in a one-day surgery ambulatory setting [16]. Our aim was also to assess the efficacy of using an elastomeric pump in the hospital setting. Our intention was to take the advantages of the pumps offered, such as facilitation of mobility and walking in the early postoperative period. Elastomeric pumps are a common solution to be used with CPNB due to their independence from electric current supply, low costs, small size, and disposability [16].
The available literature does not define precisely which method of perineural infusion is the most beneficial [2]. Furthermore, data on particular blocks are missing. With some blocks, better results are achieved with the method combining a bolus with a basal infusion, whereas with other blocks these advantages have not been proved [2]. Our study shows that using a bolus and basal infusion with femoral nerve block after TKA is more effective in pain relief during the first three days after the surgery than infusion only. The study has also demonstrated a more beneficial effect on functional results when using a bolus with basal infusion compared to using a only continuous infusion. According to Galitzine [7], when assessing the effect of CPNB on the outcome, it is not only the postoperative pain that should be considered. Regional anesthesia inhibits inflammation in the knee joint, thus reducing local edema and hyperthermia. Anti-inflammatory effects improve the joint function and increase the possibility of mobility in the conditions of adequate analgesia [7]. The study demonstrated a difference between the groups in the distance covered as well as the degree of flexion in the knee joint on days 1, 2, 3 and 4 after the surgery. The aforementioned tests were chosen for the assessment of the effects of the two methods on the functional results due to their common use in research studies and easy applicability [14]. Active knee flexion, extension or passive ROM conducted with the help of an assistant are measured with a goniometer. A patient requires 90 degrees at flexion to be able to move up and down the stairs. In order to perform daily activities adequately, the range required is 110 degrees at flexion. Effective perioperative analgesia accelerates passive flexion of the knee joint in the first two months after the surgery, but its effects on the reduction of persistent pain and functional disability remain unclear [3]. The distance covered and the degree of flexion in the knee joint were greater in group III. In the early postoperative period flexion-extension movements in the knee joint function as a pump which drains the excess water, exudate and lymph from the surgical site, thanks to which the edema in the knee joint is reduced faster. Reduced edema promotes greater mobility in the knee joint [14]. Our results show that a continuous infusion with a bolus ensures superior conditions for rehabilitation during the first 4 days after surgery when compared to a continuous infusion, and in comparison to pharmacotherapy. If the dynamic flexion-induced pain becomes more intense, the administered bolus possibly allows the nociceptive afferentiation to be minimized through increasing the concentration of a local anesthetic in the perineural space. With a continuous infusion such possibilities of immediate reaction to a pain stimulus are limited. The method of continuous infusion did not allow a more personal approach in regulating pain sensation, which may differ in a population.
Charous [5], when comparing the effect of continuous infusion with a bolus in femoral nerve block in TKA, came to the conclusion that both methods equally reduce muscular strength and did not find either of these methods superior. Other authors claimed the bolus system to be more effective in the reduction of postoperative pain intensity with a continuous sciatic nerve block in the popliteal fossa in foot surgery [10, 15]. However, in foot surgery, unlike in knee arthroplasty, a greater motor blockade does not exert such a significant influence on the course of rehabilitation. The perineural space in the popliteal fossa contains a large amount of fat tissue [15]. In femoral nerve block a local anesthetic is administered to relatively small interfascial compartments under the iliac fascia [6]. Anatomical differences may affect the pharmacokinetics and pharmacodynamics of a local anesthetic and thus may have clinical implications [5]. The above-mentioned arguments indicate that study results obtained for one site of perineural infusion should not be applied to another CPNB. The conclusions drawn for particular surgical procedures cannot be extrapolated to other operations [2]. A fact of clinical significance may be not only reducing the postoperative pain with a particular method of perineural infusion but also accelerating physiotherapy [14].
CFNB remains a widely used method [13]. As has been stated above, the significance of the dysfunction of the quadriceps femoris muscle is a much more complex process than only the one related to the direct influence of the block. The correlation between the risk of a fall and a femoral nerve block after TKA has not been proved [9]. Effective pain management still remains the main priority after TKA. CFNB is a validated method with a proven efficacy, a broad safety spectrum and minimal adverse effects. The research should continue to improve the quality of multimodal pain control [1, 12].
CONCLUSIONS
CFNB with a preoperative single-injection sciatic nerve block is an effective and safe method of postoperative analgesia, which may constitute the basis of the treatment regimen during the early postoperative period after TKA. CFNB with 0.2% ropivacaine infused at 5 mL h-1 with a PCRA bolus of 5 mL to a larger extent decreases postoperative pain intensity, opioid consumption and contributes to achieving better results in functional restoration during the first 4 days following TKA in comparison with a simple continuous infusion. Moreover, it constitutes an effective and safe alternative to using electronic pumps, also addressing the need to achieve early patient mobility.