
Introduction
Nutrition strongly influences skin health. Key nutrients, including omega-3 fatty acids, vitamins A, D, E, C, zinc, and selenium, support the epidermal barrier, regulate immune function, and reduce oxidative stress. Dietary modifications may enhance dermatological treatment outcomes and patients’ quality of life. Recent studies highlight the role of specific dietary patterns: Mediterranean, low-glycaemic, ketogenic, vegetarian, gluten-free, elimination, and low-histamine diets in modulating inflammatory skin conditions. This article reviews nutritional strategies for managing various skin diseases.
Methods
A literature search was conducted in PubMed and Scopus for articles published between 2008 and 2025 using terms related to nutrition and skin diseases, including acne vulgaris, rosacea, seborrheic dermatitis, psoriasis, atopic dermatitis, and urticaria.
Inclusion and exclusion criteria
Eligible studies assessed dietary factors, nutrients, or dietary patterns in dermatological conditions. Meta-analyses, randomised controlled trials, cohort and case-control studies, relevant animal studies, and narrative reviews were considered.
Results
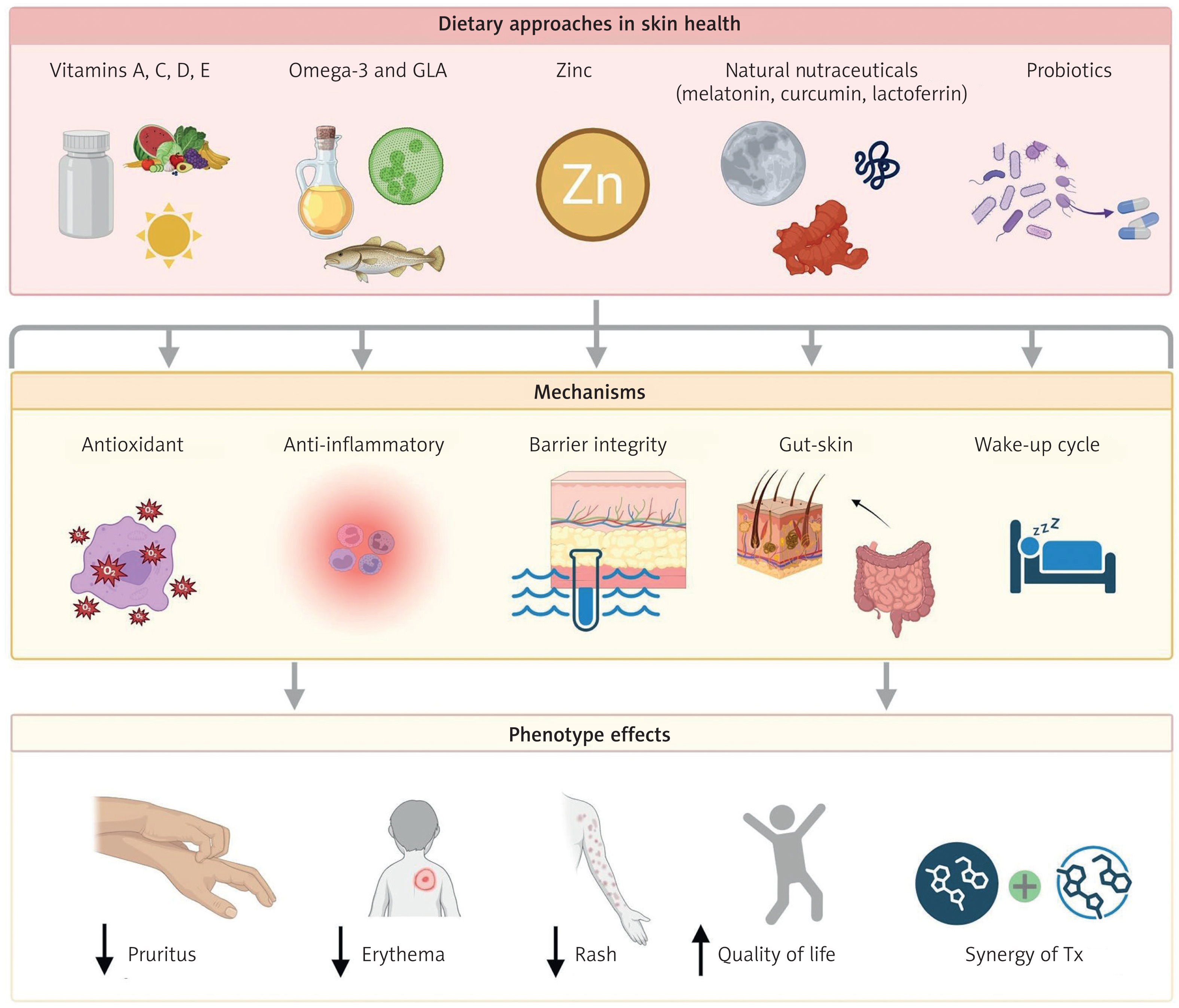
Skin health is strongly influenced by nutritional status. Nutrients not only fuel cellular metabolism but also regulate proliferation, differentiation, and repair. Because of the high proliferative activity of cutaneous tissue, adequate intake of essential macronutrients, vitamins, trace elements, and antioxidants is crucial for maintaining epidermal integrity, reducing oxidative stress, and supporting immune balance [1]. The Mediterranean diet, rich in plant-based foods with moderate fish and dairy intake and limited red meat, saturated fats, and sugars, provides these compounds in optimal proportions. Its anti-inflammatory properties and beneficial effects on the gut microbiota further contribute to systemic and cutaneous immune regulation via the gut–skin axis [2–4] (Figure 1).
Figure 1
Inflammatory mechanisms across common dermatological disorders and the modulatory role of nutrition
Acne vulgaris
Acne vulgaris is a prevalent inflammatory skin disorder driven by genetic predisposition, hormonal imbalances – particularly hyperandrogenism – Cutibacterium acnes colonization, and immune-mediated inflammation. It is often accompanied by sebaceous hyperactivity and abnormal keratinocyte differentiation, with its course further modulated by stress, certain medications or cosmetics, and diet [5].
Western diet and acne pathophysiology
Mounting evidence links the Western dietary pattern – characterized by high intake of high-glycaemic index (GI) foods, ultra-processed products, refined sugars, saturated fatty acids (SFA), and sugar-sweetened beverages – with a heightened risk and severity of acne. This diet is typically deficient in polyunsaturated fatty acids (PUFA), fibre, antioxidants, and anti-inflammatory micronutrients, which are protective against acne development [6]. The Western diet promotes hyperinsulinemia and elevated levels of insulin-like growth factor 1 (IGF-1), both of which activate signalling cascades that influence sebocyte proliferation, keratinocyte hyperproliferation, and androgen metabolism. Specifically, insulin and IGF-1 upregulate sebaceous gland activity, increasing sebum production and contributing to follicular occlusion. Moreover, excessive insulin levels stimulate gonadotropin production, leading to reduced concentrations of sex hormone-binding globulin (SHBG). This reduction increases the bioavailability of free testosterone; a key androgen associated with seborrhoea and acne severity. A positive correlation between free androgen levels and tissue insulin sensitivity has also been documented, further linking metabolic and endocrine axes with acne pathogenesis [7, 8]. Additionally, diets rich in palmitic acid – a major SFA – may promote local inflammation via upregulation of interleukin-1α (IL-1α) and interleukin-1β (IL-1β), aggravating the inflammatory component of acne. A deficiency in essential fatty acids (EFAs) may result in xerosis, altered sebum consistency, and hyperkeratinization, which contribute to comedogenesis. In contrast, adherence to a Mediterranean diet with a low glycaemic index has demonstrated potential benefits in acne management. This diet, rich in vegetables, fruits, legumes, nuts, seeds, fish, high-quality meats, eggs, dairy products, olive oil, and adequate hydration, provides antioxidants, omega-3 fatty acids, and anti-inflammatory compounds that support skin health [2, 9, 10].
Ketogenic diet
Preliminary evidence suggests that the ketogenic diet (KD) may aid inflammatory skin diseases such as acne by modulating cytokine activity through β-hydroxybutyrate and inhibiting the NLRP3 inflammasome. KD also lowers insulin and IGF-1, reducing mTORC1 signalling and sebum production. In a 2024 study, 45 days of very-low-calorie ketogenic diet (VLCKD) reduced acne severity by ~31% and decreased oxidative stress in overweight women [11]. Despite these mechanisms, clinical evidence remains limited, and well-designed randomised trials are needed to confirm its therapeutic value [12–14].
Role of omega-3 fatty acids and anti-inflammatory nutrients
Omega-3 fatty acids, particularly eicosapentaenoic acid (EPA) and gamma-linolenic acid (GLA), reduce inflammation by limiting arachidonic acid (ARA) conversion to leukotriene B4 (LTB4) and downregulating IGF-1, thereby lowering sebaceous activity. Regular consumption of fatty fish and seafood has been associated with reduced sebum production and fewer acne lesions [5, 15].
Dairy products and acne
Certain individuals with acne may be sensitive to dairy, particularly milk and whey protein, which raise IGF-1 and transform growth factor β (TGF-β) levels and contain testosterone precursors that promote sebogenesis and follicular obstruction. A 2018 meta-analysis linked whole milk, skim milk, and whey protein to increased acne risk, while yogurt and cheese showed no such association [16]. Whey protein, especially in male strength athletes, may promote acne due to its leucine content, which stimulates epidermal proliferation and sebaceous lipogenesis [17]. In contrast, fermented dairy products may exert protective effects on the skin, attribute to their lower IGF-1 content and the presence of probiotic strains such as Lactobacillus delbrueckii subsp. bulgaricus and Streptococcus thermophilus [18].
Chocolate and acne
The role of chocolate in acne remains controversial. Some studies suggest that chocolate may modulate inflammatory cytokine release triggered by Cutibacterium acnes and Staphylococcus aureus. However, natural cocoa and dark chocolate are rich in polyphenols with anti-inflammatory and antioxidant properties. Therefore, consumption of high-cocoa, low-sugar chocolate in moderation may be acceptable – and even beneficial – in an anti-acne diet [19]. Individualized dietary monitoring is advisable to identify specific food triggers.
Rosacea
Rosacea is a chronic, inflammatory dermatological disorder characterized by vascular pathogenesis, evolving progressively from transient facial erythema to more persistent symptoms, including telangiectasia, papulopustular lesions, and chronic flushing [20].
Dietary triggers
Nutritional factors can modulate inflammation and vascular tone. Reported triggers include alcohol, spicy foods, processed meats, and cinnamic aldehyde–rich foods such as tomatoes, carrots, citrus fruits, apples, chocolate, and cinnamon. Hot beverages, particularly coffee, are also implicated, though a large cohort of 82,737 women (4,945 with rosacea) showed an inverse association between caffeinated coffee intake and disease severity [21–23]. Foods high in histamine or promoting its release may exacerbate vasodilation and erythema via histamine receptor activation [22].
Vitamin B3 (niacin) may also aggravate symptoms by activating transient receptor potential vanilloid 1 (TRPV1) channels in keratinocytes and sensory neurons and stimulating the G protein-coupled receptor 109A (GPR109A) receptor on Langerhans cells [21].
Gut-skin axis and gastrointestinal comorbidities
Recent studies highlight a strong gut–skin link in rosacea, with higher rates of gastrointestinal comorbidities such as Helicobacter pylori infection, celiac disease, Crohn’s disease, ulcerative colitis, small intestinal bacterial overgrowth (SIBO), and irritable bowel syndrome (IBS). In a cohort of 49,475 individuals, rosacea was associated with a 46% higher risk of celiac disease, 45% higher risk of Crohn’s disease, and 19% higher risk of ulcerative colitis [24]. The underlying mechanisms are likely mediated by dysbiosis, increased gut permeability, and systemic pro-inflammatory cytokine release, contributing to neurovascular and immune activation [25, 26].
Nutritional recommendations
Therapeutic dietary strategies for rosacea should focus on supporting gut microbiota through higher prebiotic fibre intake and anti-inflammatory foods. An individualized assessment is essential, with monitoring of tolerance to histamine-rich foods, cinnamic aldehyde and niacin [22]. A tailored, low-histamine Mediterranean diet may help alleviate symptoms.
Seborrheic dermatitis
Seborrheic dermatitis (SD) is characterized by hyperactivity of the sebaceous glands, overgrowth of lipophilic yeasts of the Malassezia genus, cutaneous mucosal inflammation, and dysbiosis of the skin microbiota. Clinically, SD manifests as erythematous, scaly plaques accompanied by itching, burning, and in severe cases, the formation of scabs and exudates [27, 28].
Dietary influence
Although evidence is mixed, diet may influence SD. A Mediterranean diet is linked to reduced inflammation and sebum, with higher fruit intake lowering severity by 25%, while a Western diet increased the risk by 47% in women [29, 30].
Omega-3 fatty acids from fish and plant oils show anti-inflammatory, immunomodulatory, and moisturizing effects, with regular intake reducing seborrhoea and lesion severity [31, 32]. Deficiencies in biotin (vitamin B7) and vitamin D are common in SD and may worsen symptoms, warranting supplementation [33]. Vitamins A and C further support inflammation control, sebaceous regulation, and collagen synthesis, whereas deficiencies impair barrier function [30, 34, 35]. Among minerals, zinc is crucial due to its immunomodulatory, antibacterial, and antioxidant cofactor roles [36].
Western diet, glycaemic load, and inflammation
The Western diet may exacerbate SD symptoms. Such diets promote insulin resistance, hyperinsulinemia, and elevated IGF-1 levels, which contribute to androgen-mediated sebaceous gland stimulation and excessive sebum production. This pro-inflammatory dietary profile may amplify skin inflammation and dysregulate the gut-skin axis [37].
Gut microbiota and nutritional interventions
Emerging evidence indicates that patients with inflammatory skin disorders, including SD, often exhibit intestinal dysbiosis, altered gut transit, and barrier dysfunction, which can heighten systemic inflammation. Fermented foods (e.g., pickles, yogurt, kefir) and prebiotic-rich fibre may help restore eubiosis, strengthen the intestinal barrier, and support immune balance [30, 34].
Weight and caloric balance
While no definitive link has been established between obesity and SD severity, some data suggest that moderate caloric restriction may reduce systemic inflammation by decreasing the synthesis of immunoactive and endocrine factors derived from visceral adipose tissue, thereby contributing to symptom improvement [29, 30].
Atopic dermatitis
Atopic dermatitis (AD) is a chronic inflammatory skin disorder driven by immune dysregulation, with predominant T-helper 2 (Th2) responses, excessive immunoglobulin E (IgE) production, and elevated proinflammatory cytokines. Mutations in skin barrier–related genes, particularly filaggrin (FLG), are key genetic factors, while family history, pollution, stress, cosmetics, and diet influence disease severity [38, 39].
Elimination diets
Elimination diets are frequent in paediatric AD, with 16–75% avoiding eggs, milk, soy, nuts, and seafood. Prolonged restriction may cause iron, zinc, calcium, and B-vitamin deficiencies, impairing growth and cognition and raising anemia risk up to eightfold [40, 41]. In pregnancy, iron deficiency may increase offspring’s atopic predisposition [42].
Evidence is mixed; benefits occur mainly in confirmed sensitivities. Personalized, temporary elimination based on food challenges is recommended, while universal or long-term restrictions are discouraged due to the risk of nutrient loss and symptom worsening [38, 43]. No evidence supports routine avoidance during pregnancy; a varied maternal diet is protective [44, 45].
Nutritional support during pregnancy and infancy
Maternal deficiencies in vitamins A, E, D, iron, zinc, and omega-3 fatty acids increase the risk of AD in offspring, whereas breastfeeding supplies human milk oligosaccharides (HMOs) that promote immune maturation and protective gut microbiota. Higher omega-3 fatty acids in breast milk correlates with reduced atopy [45–47]. Introducing complementary foods at 17–26 weeks is linked to a lower allergy risk [48, 49].
Essential nutrients and anti-inflammatory dietary components
Diets for AD should emphasize anti-inflammatory nutrients, antioxidants, and barrier-supporting minerals such as vitamins A, E, D, zinc, copper, iron, selenium, and EFAs [50].
EFA deficiency leads to dry skin, impaired barrier, and more inflammatory lesions. GLA restores lipid balance, while omega-3 fatty acids (EPA, DHA) reduce inflammation, strengthen the barrier, and improve elasticity. Maintaining a balanced omega-6/omega-3 ratio is essential to prevent proinflammatory effects [7, 51, 53].
Gut microbiota and the skin–gut axis
Recent research links intestinal homeostasis to skin health, with AD associated with reduced beneficial microbes such as Faecalibacterium prausnitzii, Lactobacillus, Bifidobacterium, and Akkermansia, and increased Clostridium difficile [54–56]. A diet rich in prebiotic fibres supports microbial diversity and strengthens the intestinal barrier, which is crucial for immune regulation [57, 58].
Intestinal dysbiosis promotes the generation of harmful metabolites, such as p-cresol and free phenols, which can reach the skin via the bloodstream and impair barrier integrity and hydration [7, 59]. Short-chain fatty acids (SCFAs) provide protection:
Dietary patterns and clinical implications
The Mediterranean diet encompasses many of the nutrients and compounds beneficial for AD. Vegetarian or flexitarian diets may also be effective due to their high content of plant-derived anti-inflammatory agents and prebiotic compounds [43, 53]. In contrast, the Western dietary pattern is associated with proinflammatory responses, barrier dysfunction, and increased AD severity [62, 63].
Psoriasis
Psoriasis is a chronic, immune-mediated inflammatory skin disorder characterized by keratinocyte hyperproliferation, aberrant immune responses, and recurrent episodes of exacerbation and remission. It often coexists with other autoimmune conditions and is associated with both cutaneous and systemic comorbidities, notably cardiovascular disease [64, 65].
Dietary models
Mediterranean diet
The Mediterranean diet exerts anti-inflammatory, antioxidant, and cardioprotective effects. This diet is rich in fibre, PUFAs, flavonoids, carotenoids, vitamins C and E, coenzyme Q10, and selenium, all of which contribute to a reduction in oxidative stress, modulation of inflammatory cytokines, and improved microvascular function [66, 67].
Studies indicate an inverse association between adherence to the Mediterranean diet and Psoriasis Area and Severity Index (PASI) scores. GI foods are advised, as simple sugars may aggravate psoriatic lesions. Monounsaturated fatty acids (MUFA), particularly oleic acid from olive oil and avocados, help protect cell membranes and lipoproteins from oxidative damage [64, 68].
Omega-3 fatty acids reduce proinflammatory mediators by competing with arachidonic acid for cyclooxygenase-2 (COX-2), lowering tumor necrosis factor-α (TNF-α), IL-1, interleukin-6 (IL-6), and interleukin-8 (IL-8) levels [69]. Higher omega-3 levels correlate with lower PASI scores, with an optimal omega-6 : omega-3 ratio of 3 : 1. Additionally, omega-3 fatty acids support neurotransmitter balance and reduce depressive symptoms making them especially relevant in psoriasis management [66, 69].
Vegetarian diet
A vegetarian diet may be particularly advantageous due to its exclusion of animal-derived arachidonic acid, a precursor of proinflammatory LTB4. This dietary model is rich in antioxidants, PUFAs, fibre, and micronutrients, and has been associated with reduced systemic inflammation, lower leukotriene levels, and reduced cardiovascular risk. Furthermore, vegetarians are less likely to be overweight, which is independently associated with reduced disease severity [2, 70].
Gluten-free diet
A vegetarian diet may be beneficial in psoriasis because it excludes arachidonic acid, a precursor of pro-inflammatory LTB4, and is rich in antioxidants, PUFAs, fibre and micronutrients. This dietary pattern is linked to lower systemic inflammation, reduced leukotriene levels and decreased cardiovascular risk, and vegetarians tend to have lower body weight, which can also lessen disease severity [71–73]. A gluten-free diet may improve symptoms only in patients with positive celiac serology; in seronegative individuals no benefit has been shown, so gluten should be removed only after diagnostic confirmation to avoid unnecessary restrictions.
Ketogenic diet
A very-low-calorie ketogenic diet may help psoriasis patients with obesity by reducing weight, visceral fat, and systemic inflammation, though evidence is limited. A 4-week VLCKD improved metabolic and inflammatory markers, including IL-1β [74]. A 10-week program with an initial VLCKD phase improved PASI, but benefits cannot be clearly attributed to ketosis [75]. In murine models, ketogenic diets, especially those high in MCTs (high in medium-chain triglycerides), have been shown to exacerbate psoriasiform lesions [76].
Energy restriction and obesity
A hypocaloric diet is recommended for patients with coexisting overweight or obesity, which are strongly associated with psoriasis pathogenesis. Obese individuals display elevated levels of T helper type 1 (Th1) and Th17 lymphocytes, contributing to systemic inflammation [77–79]. Psoriasis prevalence is doubled in individuals with BMI > 29 kg/m2, especially with visceral obesity and low muscle mass [80]. Weight loss improves disease severity and quality-of-life measures, inflammatory markers and treatment response [81].
Urticaria
Urticaria is a multifactorial skin disorder characterized by transient wheals with intense pruritus, sometimes with angioedema. Acute forms last less than 6 weeks, while chronic urticaria affects ~1% of the population and often recurs with remissions [82]. It involves immune dysregulation, where mast cell degranulation releases histamine that binds to histamine type 1–4 (H1–H4) receptors, causing vascular leakage, itching, and erythema [83].
Dietary triggers
Urticaria may arise from IgE-mediated allergy or non-IgE mechanisms such as histamine intolerance. Ingestion of histamine-rich or histamine-liberating foods can trigger symptoms, and individualized dietary restriction may improve control [84].
A low-histamine diet may reduce plasma histamine and improve symptoms. Foods to limit include:
Fermented/aged products: cheeses, yogurt, kefir, smoked or canned fish, aged meats, wine.
Certain fruits and vegetables: citrus, strawberries, avocados, spinach, tomatoes, eggplant, mushrooms.
Legumes and dried fruits.
Beverages and additives: coffee, tea, fruit juices, benzoates, sulfites, monosodium glutamate (MSG) [85, 86].
Pseudoallergens and salicylate sensitivity
Pseudoallergens, such as naturally occurring salicylates in plant foods, can trigger hypersensitivity-like reactions without IgE involvement. Up to 50% of chronic urticaria patients show dose-dependent sensitivity, and reducing salicylate intake may alleviate symptoms in some cases despite inconsistent evidence [87, 88].
High-salicylate foods include: fruits (especially berries, citrus), olives, tomatoes; spinach, artichokes, peas, mushrooms; legumes, eggs, fish; coffee, tea, honey, spices, processed foods, and sweets.
This strategy should only be implemented under clinical supervision and as part of diagnostic investigation, rather than routine management.
Urticaria and celiac disease
An association between chronic urticaria and celiac disease has been reported. Increased intestinal permeability in celiac disease may allow dietary antigens to trigger immune activation and IgE-mediated mast cell degranulation, making urticaria a possible extraintestinal manifestation even without gastrointestinal symptoms [89, 90]. Serologic screening may be considered in selected patients, and a gluten-free diet can improve symptoms in those with confirmed celiac disease, whereas unnecessary gluten restriction is not recommended.
Discussion
Cited studies indicate that nutritional interventions can influence the course of dermatological diseases, including acne, rosacea, psoriasis, atopic dermatitis and urticaria. Their beneficial effects are mainly associated with modulation of inflammation, reduction of oxidative stress, support of the skin barrier and interactions within the gut–skin axis (Figure 1). Dietary approaches such as low-glycaemic-load patterns, omega-3 fatty acid intake, elimination of trigger foods and adequate antioxidants show the strongest evidence for acne, psoriasis and atopic dermatitis, with more variable findings for rosacea and urticaria. Limited methodological consistency and small samples reduce the strength of conclusions, and self-reported data introduce bias. Emerging evidence suggests that ketogenic dietary strategies may also modulate inflammatory pathways, although current data remain preliminary. Given the complexity of nutrition–skin interactions, larger, well-controlled studies are needed to establish clear dietary recommendations for dermatological patients.
Conclusions
Dietary patterns significantly affect skin health: Western diets exacerbate inflammation and metabolic imbalance, while Mediterranean diets provide protective, anti-inflammatory benefits. Nutrients such as omega-3 fatty acids, antioxidants, vitamins, and minerals improve barrier integrity and immune regulation. Personalized approaches, including low-GI, low-histamine, gluten-free, or supervised elimination diets, may support conventional therapies. Further clinical studies are required to establish clear, evidence-based nutritional guidelines for dermatological practice.







