
Introduction
Atopic dermatitis (AD) is among the most common inflammatory skin diseases, affecting 1–3% of adults and 15–25% of children worldwide [1]. It is characterized by eczematous lesions with a chronic, relapsing course and a marked tendency for exacerbations, invariably accompanied by intense pruritus – the hallmark of the disease [2]. The clinical presentation of AD may be acute – with erythematous papules or plaques, pronounced epidermal desquamation, and oozing erosions – subacute, or chronic, with the latter typically manifesting as lichenification (thickened skin with accentuated natural lines) [3]. While the most frequent disease trajectory involves onset in early childhood followed by spontaneous remission (“outgrowing” the disease) [4], distinct phenotypes are also observed in adults and elderly patients [5].
Secondary features of AD include xerosis resulting from impaired epidermal barrier function, as well as a predisposition to atopy – defined as an increased propensity for IgE-mediated hypersensitivity reactions [1, 3]. Cutaneous dysbiosis further contributes to heightened susceptibility to bacterial, viral, and fungal infections, with Staphylococcus aureus being the predominant pathogen [6]. These abnormalities markedly impair quality of life and increase the risk of emotional and psychological disturbances [7]. Indeed, AD is associated with the greatest quality-of-life impairment among all chronic skin disorders [8], and its management imposes substantial economic burdens on both patients and healthcare systems [1]. Patients with severe disease are particularly vulnerable, frequently experiencing depression, anxiety, and an elevated risk of suicidal ideation [9].
AD often coexists with other atopic conditions – including allergic asthma, allergic rhinitis, and conjunctivitis (historically referred to as the “atopic march” but now more accurately described as “atopic clustering” [3]) – as well as autoimmune diseases such as vitiligo and alopecia areata [10, 11]. Additional, less well-defined associations remain under investigation, particularly possible links with cardiovascular diseases and malignancies [11].
The nail apparatus is a specialized structure that protects the distal digits and enhances both sensory perception and fine motor skills [12]. The nail matrix produces the nail plate – a highly keratinized structure composed of multiple layers of keratin-filled cells resting on the nail bed. Beyond its functional role, the nail is also a key aesthetic element. Its abnormalities can significantly diminish quality of life [13]. Traditionally, AD was not considered to involve the nails, as its underlying pathology does not primarily target the nail matrix or bed – in contrast to other inflammatory dermatoses such as psoriasis or lichen planus, which frequently manifest with nail changes [14].
Nevertheless, several mechanisms could contribute to secondary nail abnormalities in AD. Persistent pruritus inevitably results in repeated scratching, causing direct mechanical trauma to all components of the nail unit [15]. Furthermore, an impaired skin barrier increases vulnerability to infections, which may further compromise nail integrity [16].
Despite this plausible pathophysiological rationale, nail involvement in AD remains poorly understood and has been addressed in only a limited number of studies. Detailed analyses of the specific types and patterns of nail changes in this patient population are lacking.
Aim
The aim of this study was to assess the frequency and types of nail abnormalities in adult patients with severe AD, and to explore potential distribution patterns and clinical factors associated with their occurrence.
Material and methods
This single-centre, cross-sectional study was conducted at the Department of Dermatology and Allergology, University Hospital in Krakow. The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [17]. All patients meeting the inclusion criteria and providing written informed consent were enrolled; thus, convenience sampling was applied.
The inclusion criteria were: (1) diagnosis of AD confirmed by a board-certified dermatologist-venereologist according to the Hanifin and Rajka criteria [18]; (2) severe disease, defined as an Eczema Area and Severity Index (EASI) score > 21 points [19]; and (3) age ≥ 18 years. The exclusion criterion was the presence of other inflammatory skin diseases or systemic conditions affecting the nails.
The following data were collected: age and sex, age at AD onset, disease severity (EASI score), most recent total serum IgE concentration (measured within the preceding 28 days), and types of hand nail abnormalities observed.
All participants were treated in the standard way according to the Polish and European guidelines [20–23].
IgE levels were assessed from fasting serum samples using fluorimetric analysis with the UniCAP system (Phadia, Stockholm, Sweden).
Statistical analysis
Nominal variables were presented as counts and percentages (N, %), whereas continuous variables were reported as medians and interquartile ranges (Q1–Q3) due to non-normal distribution, as assessed by the Shapiro-Wilk test and visual inspection of histograms. There were no missing data in the analysis.
Comparisons of proportions for binary categorical variables were performed using the two-sided Fisher’s exact test, whereas variables with more than two categories were analysed using the χ2 test. Relationships between continuous variables were evaluated using Spearman’s rank correlation, with the correlation coefficient (R) used to quantify the strength of association.
Comparisons of continuous variables between two groups were conducted using the Mann-Whitney U test, while comparisons involving more than two groups were analysed using the Kruskal-Wallis test followed by post-hoc Bonferroni correction.
Principal component analysis (PCA) was applied to explore patterns in nail abnormalities among patients with AD. The analysis was based on a binary matrix containing 14 nail abnormalities per participant. A covariance matrix was calculated from centred data, followed by eigendecomposition to extract the principal components. PCA was used as an exploratory method for binary data to identify dominant patterns and feature associations [24]. The total variance explained by each component was calculated, and the first two components – accounting for the majority of the variance – were selected for visualization.
Unsupervised clustering was then performed to identify distinct phenotypic subgroups based on nail abnormality profiles. Jaccard distances were calculated for all pairwise combinations of participants, and agglomerative hierarchical clustering with average linkage was applied to the resulting dissimilarity matrix. The optimal number of clusters (k = 3) was determined based on the highest silhouette score observed across a range of k values (2–6).
The significance threshold for type I error was set at α = 0.05. To control the false discovery rate due to multiple testing, the Benjamini-Hochberg procedure was applied with a false discovery rate set at 0.05.
All statistical analysis were performed using IBM SPSS Statistics for Windows, version 29.0.2.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 47 participants were consecutively recruited, comprising 28 (60%) males and 19 (40%) females. The median age was 37.0 years (Q1–Q3: 26.0–51.0). Most participants reported disease onset during infancy (43%) or between the ages of 12 and 60 years (36%). The median EASI score was 48.2 (Q1–Q3: 36.6–53.5), and the median serum IgE concentration was 4080.0 UI/ml (Q1–Q3: 1780.0–13,600.0). Baseline characteristics are presented in Table 1.
Table 1
Baseline characteristics of the study group (N = 47)
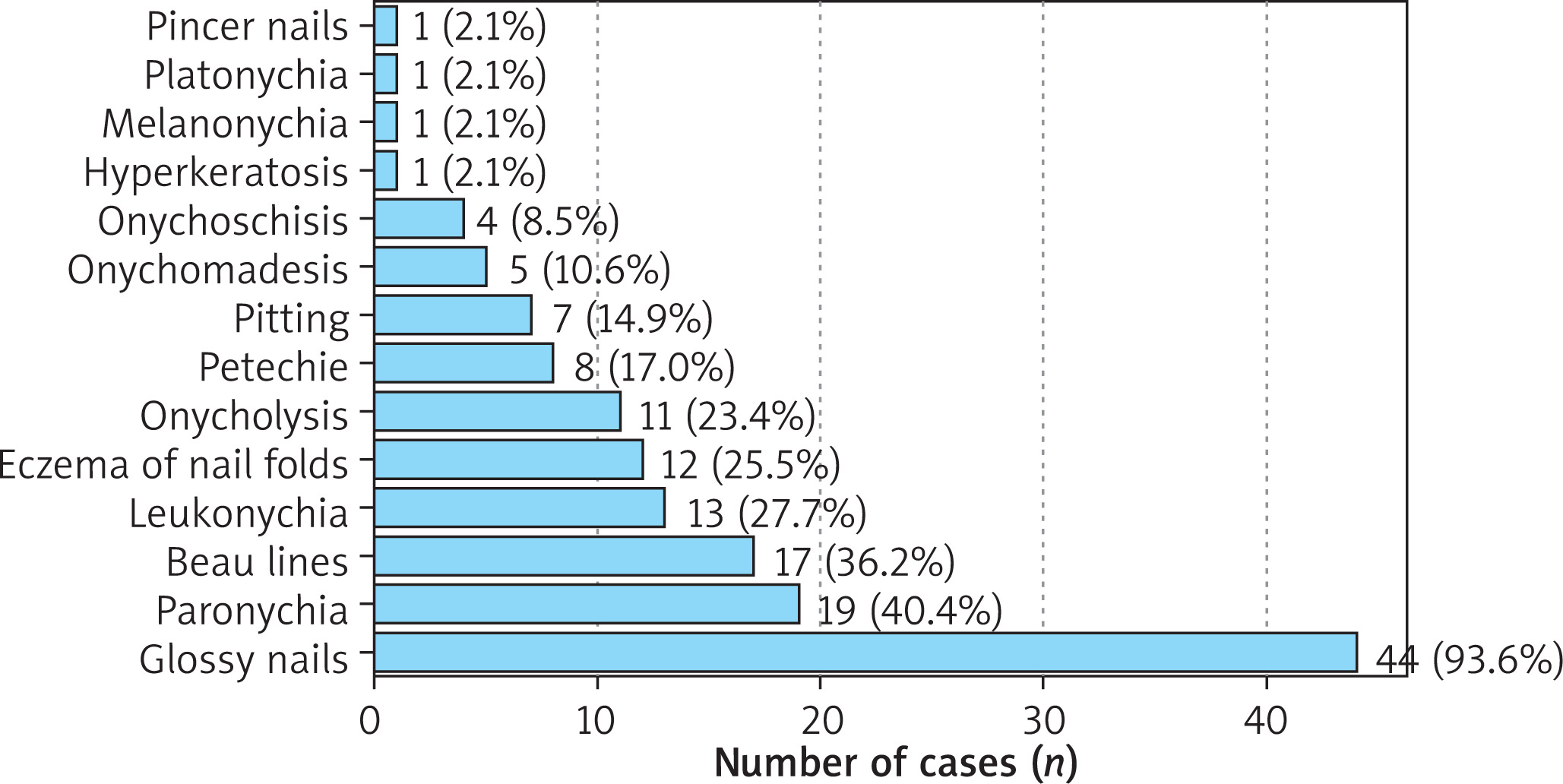
Glossy nails were the most frequently observed abnormality, present in 94% of participants. Other common findings included paronychia (40%) and Beau’s lines (36%). The counts and frequencies of all identified nail abnormalities are shown in Figure 1.
Comparisons of baseline clinical characteristics between participants with and without specific nail abnormalities revealed, after correction for multiple comparisons, that higher EASI scores were significantly associated with the presence of Beau’s lines, onychomadesis, eczema of nail folds, petechiae, and paronychia (pBH < 0.05) (Table 2). Unadjusted p-values for all comparisons are provided in Supplementary Table S1.
Table 2
Statistically significant relationships between presence of nail abnormalities and EASI score. Clinical predictors were compared between patients with and without the feature using the Mann-Whitney U test. The table presents median values and interquartile ranges (Q1–Q3) for each group, along with original and Benjamini-Hochberg (BH) corrected p-values
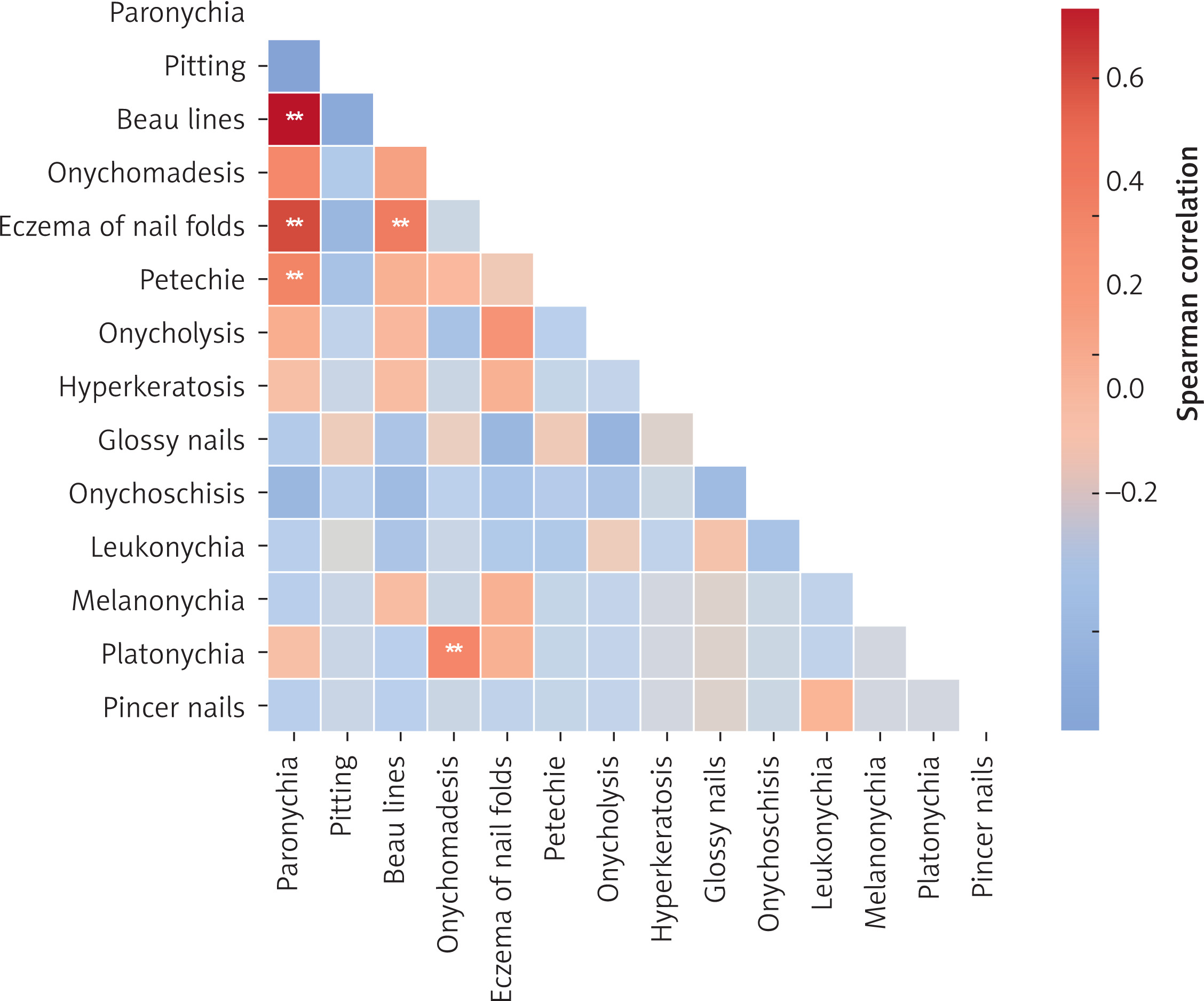
Correlation analysis demonstrated strong positive associations between paronychia and Beau’s lines (R = 0.73, pBH < 0.001), paronychia and eczema (R = 0.61, pBH < 0.001), and paronychia and petechiae (R = 0.43, pBH = 0.009). Additional correlations were observed between Beau’s lines and eczema (R = 0.47, pBH < 0.001) and between onychomadesis and platonychia (R = 0.43, pBH = 0.042). The complete correlation matrix is presented in Figure 2.
Figure 2
Spearman correlation matrix presenting relationships between particular types of nail abnormalities. Correlations that remained significant after Benjamini-Hochberg correction for multiple comparisons are marked with a double star mark (**)
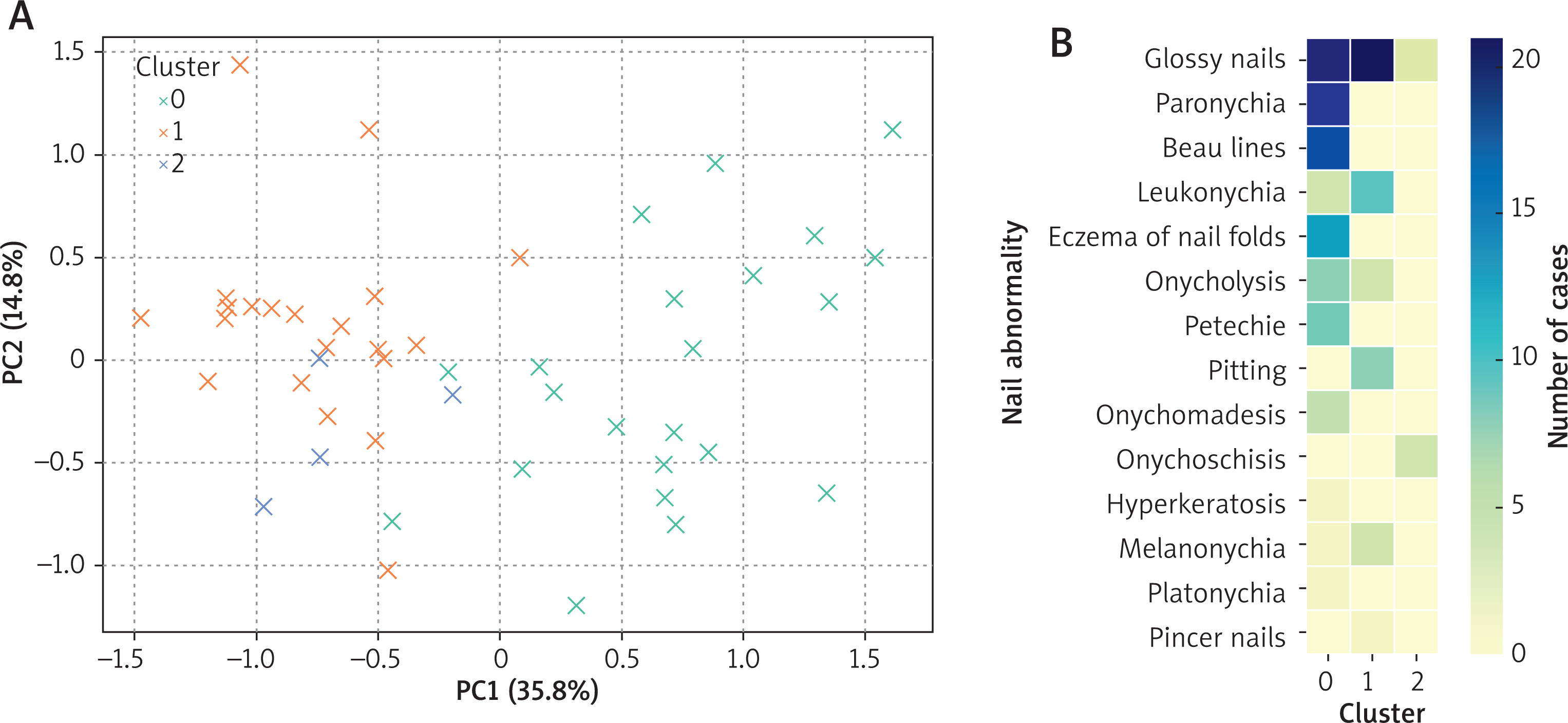
An exploratory PCA identified three distinct clusters (Figure 3 A), with the frequency of specific nail abnormalities depicted in Figure 3 B. Based on the type and distribution of changes, these were designated as the “destructive-type”, characterized by multiple abnormalities involving the nail matrix, plate, and bed; the “mild-type”, comprising more benign changes such as leukonychia and pitting with occasional onycholysis; and the “onychoschisis-type”, in which onychoschisis was the sole predominant finding. Glossy nails were present in nearly all participants and did not differentiate the clusters.
Figure 3
A – Principal Component Analysis (PCA) of nail abnormality patterns among patients with atopic dermatitis. The plot displays the first two principal components (PC1 and PC2), which explain 35.8% and 14.8% of the total variance, respectively. Each point represents a single patient and is coloured according to their assigned cluster. PCA was performed on binary variables representing the presence or absence of 14 distinct nail changes. B – Heatmap illustrating the frequency of 14 distinct nail abnormalities across the three identified patient clusters. The colour intensity reflects the number of patients within each cluster exhibiting a given abnormality
Comparison of baseline clinical characteristics between clusters (Table 3) showed that participants in the “destructive-type” group were significantly older and had more severe disease (p < 0.05). Notably, age and disease severity were not correlated in the studied population (R = 0.07, p = 0.7). Although total IgE concentrations differed across clusters, post-hoc analysis did not identify statistically significant differences between individual groups.
Table 3
Clinical characteristics of patients across the three identified clusters. Clinical predictors were compared between clusters using the Kruskal-Wallis test with post-hoc comparisons after Bonferroni correction (continuous data) or χ2 test (categorical data)
| Variable | Cluster 0 (“destructive-type”) | Cluster 1 (“mild-type”) | Cluster 2 (“onychoschisis-type”) | P-value |
|---|---|---|---|---|
| Age [years], median [Q1–Q3] | 41.5 [31.8–53.8]a | 29.0 [22.0–39.6]a | 51.0 [27.0–54.8] | 0.013 |
| Sex, n (%) | ||||
| Male | 11 (50) | 7 (33) | 1 (25) | 0.4 |
| Female | 11 (50) | 14 (67) | 3 (75) | |
| Total IgE [IU/ml], median [Q1–Q3] | 7520.0 [2465.0–17975.0] | 3300.0 [990.5–6200.0] | 11845.0 [4332.5–19650.0] | 0.024 |
| Age of onset [years], median [Q1–Q3] | 6.5 [1.0–21.3] | 3.0 [1.0–18.0] | 24.5 [5.5–37.5] | 0.2 |
| Disease duration [years], median [Q1–Q3] | 28.5 [17.8–40.3] | 22.0 [9.0–36.0] | 22.0 [12.8–30.5] | 0.4 |
| EASI [points], median [Q1–Q3] | 53.5 [52.2–57.2]a | 37.0 [32.4–45.5]a | 39.5 [31.4–52.7] | < 0.001 |
Discussion
This study provides new insights into the spectrum and patterns of nail abnormalities in patients with severe AD. Glossy nails were present in nearly all participants, while Beau’s lines and paronychia were also observed at high frequency. The analysis revealed that destructive nail abnormalities were associated with greater disease severity and older age. Furthermore, patients could be classified into three distinct subgroups based on the pattern of nail involvement: destructive-type, mild-type, and onychoschisis-type.
Recognition of specific nail manifestations in AD is an essential step towards guiding appropriate therapeutic strategies for affected patients. Several mechanisms may contribute to the development of these abnormalities, including damage to the proximal nail fold, matrix, bed, or hyponychium. The existing literature consistently emphasizes that nail involvement in AD remains underrecognized and underreported [25].
According to a systematic review by Chng and Yew, the prevalence of nail lesions in AD is estimated at 11% (95% CI: 9–14%), with only a few studies reporting higher rates of 20–30% [26]. In a cross-sectional analysis by Satasia and Sutaria, nail disorders attributed to AD accounted for only about 1% of all nail disease cases [27]. In contrast, nail abnormalities were identified in all participants in the present study, with glossy nails as the most frequent finding. This feature reflects the shiny appearance of the nail plate caused by mechanical polishing from chronic scratching – a common behaviour in AD. Importantly, even when glossy nails were excluded from analysis, at least one other nail abnormality was present in 90% of participants. This striking prevalence is likely related to the high severity of the disease in our cohort. For comparison, in dermatoses typically associated with nail involvement, the point prevalence of nail changes is approximately 50%, while lifetime incidence may reach 90% [28].
Inflammatory changes in the proximal nail matrix can produce features such as pitting, melanonychia or transverse grooves (Beau’s lines) [26, 29, 30]. Inflammation of adjacent skin on the hands and feet increases the likelihood of nail involvement [30]. Other contributory mechanisms include mechanical trauma from intense scratching and, in rare instances, deliberate self-induced nail damage [31]. These mechanisms are not specific to AD and are responsible for the presence of nail lesions in other inflammatory dermatoses such as psoriasis, lichen planus, or non-atopic eczema [29].
The observed association between disease severity and specific nail abnormalities aligns with prior findings. In a paediatric cohort, Arslan Uku et al. reported that nail pitting was significantly more frequent in AD than in controls (26% vs. 6%, p = 0.007) and correlated with SCORAD (R = 0.21, p < 0.05) [25]. IgE concentrations in our cohort were markedly higher, likely reflecting the exclusive inclusion of patients with severe AD [32].
Reports of marked improvement in nail lesions following dupilumab therapy underscore the potential role of biologic agents in targeting the underlying immunological pathways of AD [33, 34]. However, rare cases of transient worsening of nail lesions despite overall cutaneous improvement have also been documented [35].
The classification proposed in this study demonstrates a clear relationship between the type of nail abnormalities and AD severity. The mild-type subgroup was characterized by nail pitting and leukonychia without nail fold involvement. Leukonychia reflects mild nail bed pathology, whereas pitting indicates limited proximal matrix disruption. These features are therefore more likely to occur in patients with less severe disease, while more aggressive inflammatory activity can produce lesions resulting from matrix damage such as Beau’s lines.
Some participants displayed isolated onychoschisis. Previous studies have shown that this condition can result from repeated cycles of handwashing and drying [36], suggesting a behavioural component in these cases. Notably, onychoschisis responds well to treatment with oral biotin [37], highlighting a potential targeted intervention for this subgroup.
A particularly noteworthy finding was the association of destructive-type nail changes with older age, despite no direct correlation between age and AD severity. Interestingly, total IgE concentrations were lowest in this subgroup. While our classification scheme shows promise for clinical utility, it requires validation in larger, prospective cohorts.
This study has several limitations. Its cross-sectional design precludes assessment of causal relationships and limits longitudinal inference, such as evaluating the impact of treatment over time. Recruited from a single centre, the moderately-sized study population may not fully capture the clinical heterogeneity of AD. Due to sample size restrictions, the results of PCA and clustering were merely exploratory, although further analysis highlighted substantial differences between identified clusters, supporting their validity. Moreover, as only patients with the most severe form of the disease were included, the findings may not be generalizable to those with milder AD. In particular, the inclusion of control groups (such as individuals with mild or moderate AD, other dermatoses, or healthy subjects) would allow to draw important conclusions regarding the relationship between the underlying entity and the nail changes, as currently we were not able to rule out they were caused by non-specific factors such as mechanical or environmental ones.
Conclusions
Nail abnormalities are a frequent finding in patients with severe AD and contribute substantially to overall disease burden. Their occurrence appears to be closely linked to disease severity, with distinct profiles of nail changes reflecting varying degrees of structural damage. Depending on the extent of eczema, specific types of nail involvement may be anticipated. Longitudinal studies are needed to evaluate the natural course of these abnormalities and to determine the impact of AD treatment on nail outcomes.







