








Introduction
Idiopathic trigeminal neuralgia (ITN) is severe chronic neuropathic facial pain, characterized by recurrent episodes of intense, lancinating pain localized to dermatomes of the face innervated by the trigeminal nerve [1]. Oral medication, rapid and convenient, is the first-line therapy for ITN [2]. However, for medication-resistant or medication-intolerant ITN, surgical treatment needs to be considered [3].
Because of minimal trauma and long-term pain relief, percutaneous trigeminal radiofrequency thermocoagulation (PT-RFT) has become a primary minimally invasive surgical treatment modality [4]. However, the technique is associated with a high incidence of post-operative facial numbness because of nerve injury caused by the high temperatures needed for thermocoagulation [5]. In comparison, coblation has been reported to produce only slight numbness when used to ablate the thoracic paravertebral nerve [6]. The relatively low working temperature (40–70°C) and the short thermal penetration distance (~1.0 mm) of coblation might help preserve neural function.
Aim
In our previous study, we provided preliminarily data showing that coblation can reduce the degree of postoperative facial numbness in patients with ITN in the short term [7]. In the present study, we further evaluate the long-term efficacy and safety of ablating the trigeminal ganglion with coblation technology under fluoroscopic guidance.
Material and methods
The randomized, prospective, clinical study was approved by the institutional Ethics Examining Committee of Human Research. A total of 56 patients with TN provided written informed consent, and were randomly scheduled to receive coblation (coblation group) or PT-RFT (RFT group) of the trigeminal ganglion between January, 2017 and June, 2018. ITN was diagnosed according to the criteria of the International Classification of Headache Disorders-II (2004).
After entering the sterile operating room, all patients received standard monitoring, that is, heart and respiratory rate, and fingertip digital oximetry. A 0.5 g dose of atropine was administered intravenously 5 min prior to surgery to block the trigeminal–baroreceptor reflex, and a 50 µg dose of fentanyl was injected intravenously to provide analgesia. No other sedatives were given, to maintain consciousness and responsiveness to nerve root stimulation during surgical procedures.
All surgical procedures were performed under fluoroscopic guidance, with the patient in the supine position. A soft pad of 10 cm thickness was placed under the neck to retroflex the head approximately 45°. Fluoroscopic guidance was performed with the OEC 9900 Elite C-Arms (the American, GE). The preset coronal and sagittal angles of the X-ray tube to reveal the foramen ovale (FO) were 10° and 10°, pre-operatively (Photo 1 B).
Photo 1
A – Lateral view of C-arm showed that the depth of the needle tip was not beyond the clivus. B – For the coaxial view, the preset coronal and sagittal angles of the X-ray tube to reveal the foramen ovale (FO) were 10° and 10°
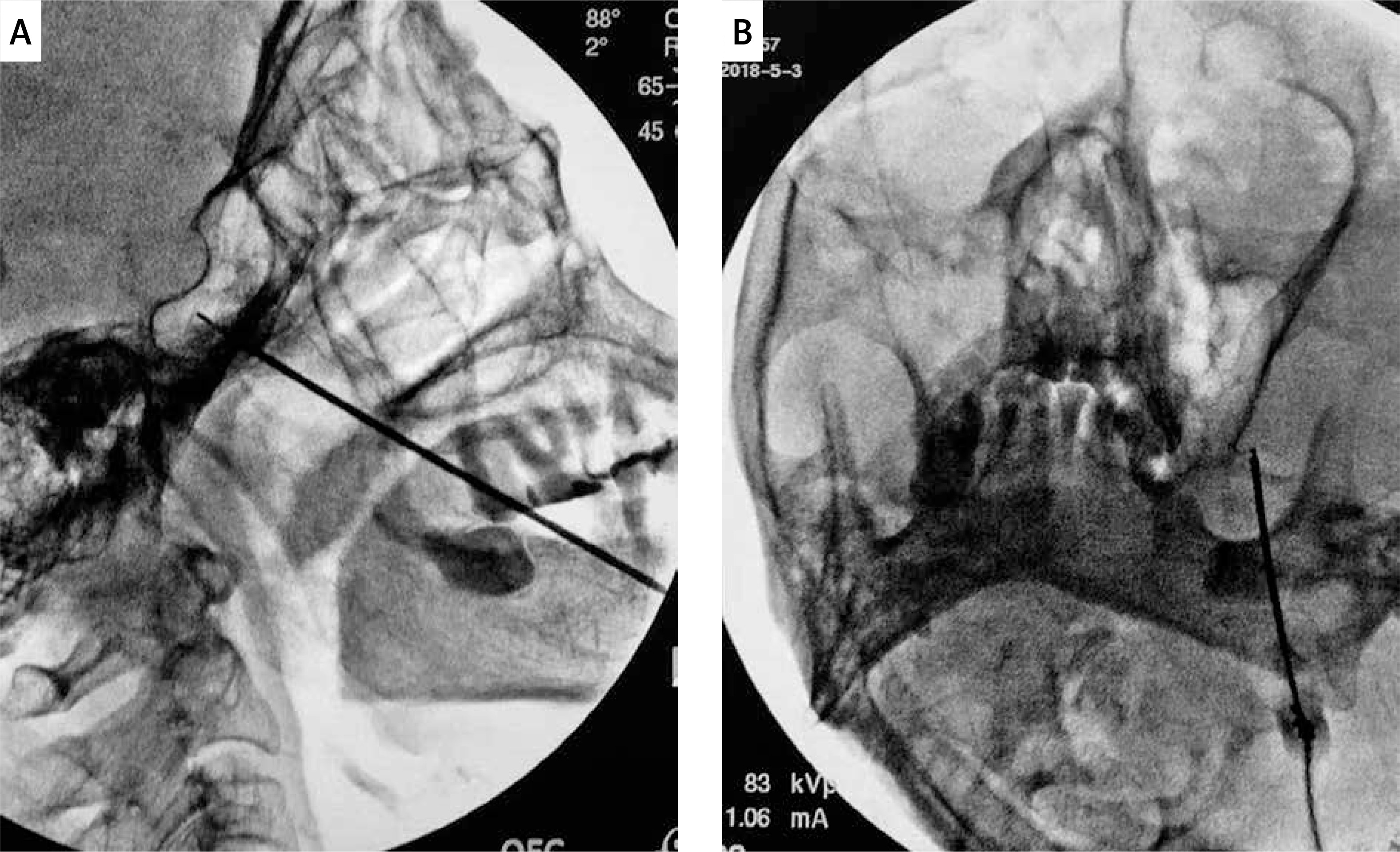
After clearly visualizing the FO, an 18-gauge, 8-cm, guide needle was inserted through the sterilized skin after local anesthesia with 0.5% lidocaine with the “Haertel” approach. During the puncture procedure, advancement was stopped when the needle entered the FO, and the coblation wand (UNITEC, China America United Technology (Beijing) Co. Ltd, Beijing, China) was inserted into the guide needle and extended approximately 5 mm beyond its tip. The correct coblation wand position was checked radiologically in coaxial and lateral views, and the depth of the tip of the coblation wand was not beyond the clivus. Test coagulation for 0.5–1 s, with the radiofrequency controller set at intensity setting #1, was performed to re-adjust the coblation wand position with the patient awake and responsive. Intravenous anesthesia with propofol (1–2 mg/kg) and fentanyl (50 µg) was administered after verifying the final position of the wand tip, and the ablation of ganglion was performed at intensity setting #2 for a duration of 30 s. Depending on the nerve branch and the physician’s judgment, ablation was performed 2 or 3 times. After PT-RFT or coblation, all patients were asked to remain in bed for 48 h to prevent intracranial hypotension headache.
Preoperative data, including age, gender, location of pain and preoperative visual analog scale (VAS) score, were recorded. Follow-up evaluation was performed on the first day and at the end of the first month, third month, sixth month and first year after surgery. To assess the degree of numbness, the numbness rating scale described in our previous report was used [8] (Table I).
Table I
Numbness rating classification
| Grade | Performance |
|---|---|
| 0 | No numbness |
| I | No obvious numbness |
| II | Mild numbness, occasionally affects daily life |
| III | Moderate numbness, frequently affects daily life |
| IV | Painful numbness, severely affect daily life |
Statistical analysis
In this study, a sample size of 25 per group was used to obtain a power of 90% to show a difference of 6 points on the VAS between the two groups at a significance level of 5% (two-tailed). Taking into account a potential dropout rate of 10% (3 patients), we increased the sample size to 28 per group. All data were analyzed with SPSS version 19.0, using mean and standard deviation, with t-test and rank-sum test for post hoc comparisons. Statistical significance was accepted at p < 0.05.
Results
A total of 50 patients with TN were ultimately included in this study (3 cases were dropped from each group for logistical reasons). The basic preoperative data for the two groups are shown in Table II. There were no significant differences in gender, age, pain location or preoperative VAS score between the two groups.
Table II
Characteristics of patients
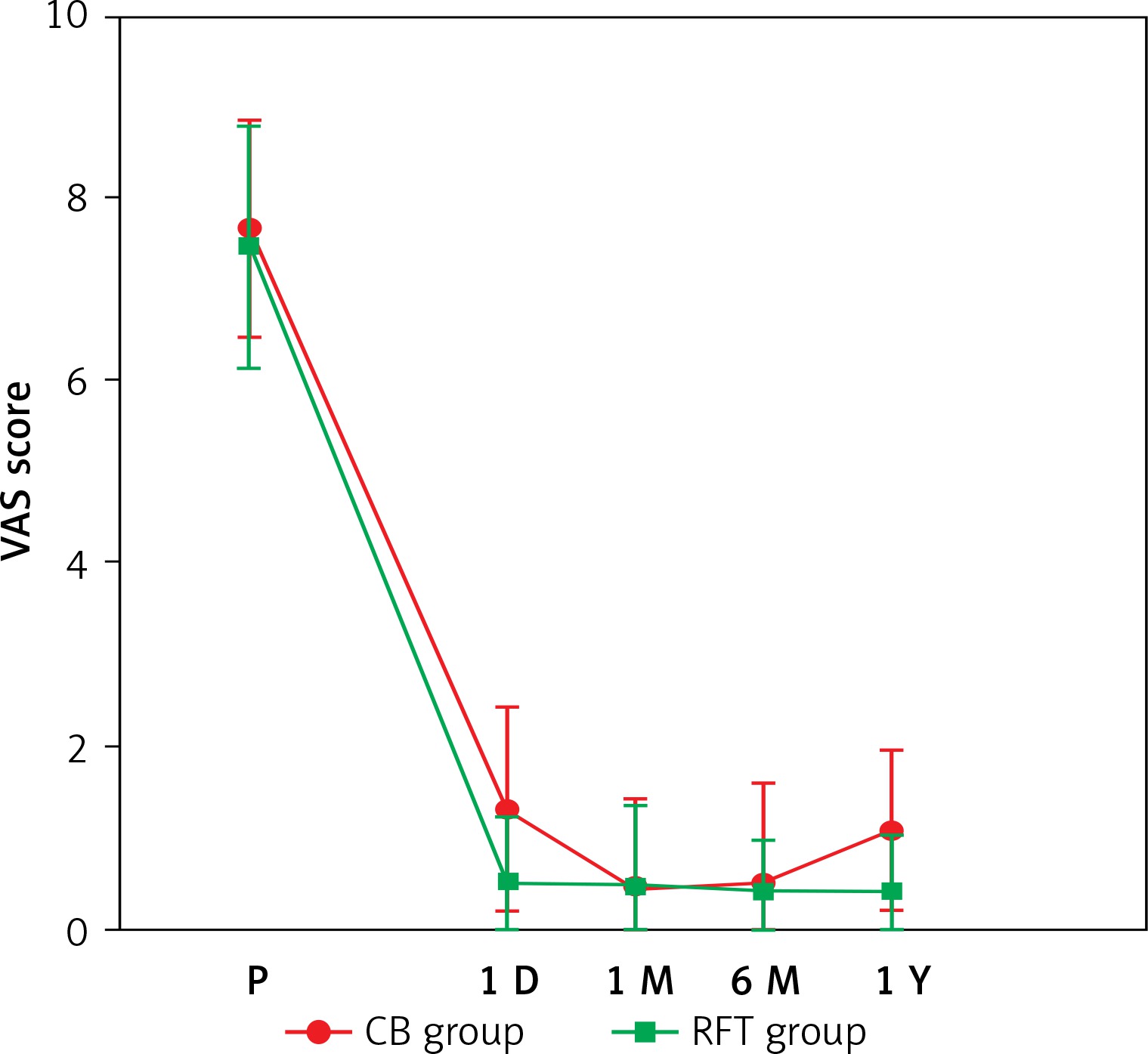
Post-surgery VAS scores were significantly lower in both groups compared with pre-surgery scores (p < 0.05), indicating that both methods effectively alleviated pain. At each time point, from 1 day to 1 year, the VAS scores and other parameters were not significantly different between the two groups (p > 0.05) (Figure 1).
Figure 1
Postprocedure VAS scores between two groups
CB – coblation, RFT – radiofrequency thermocoagulation, P – presurgery.
Among the patients, 19 (76%) developed different degrees of facial numbness (grades II–IV) after PT-RFT, while 13 (52%) experienced facial numbness after coblation. One patient in the PT-RFT group experienced painful numbness (grade IV), which subsided to grade III 1 year after surgery, while no patient exhibited painful numbness in the coblation group. The rank-sum test for facial numbness degree showed that the patients in the PT-RFT group experienced more severe numbness than the patients in the coblation group, and these differences were statistically significant (p < 0.05) (Table III).
Table III
Comparison of degree of postoperative facial numbness in the 2 groups
| Numbness degree | Group RF | Group CB | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 D | 1 M | 6 M | 1 Y | 1 D | 1 M | 6 M | 1 Y | |
| Grade 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Grade I | 6 | 6 | 6 | 6 | 12 | 13 | 19 | 19 |
| Grade II | 9 | 12 | 11 | 13 | 12 | 10 | 6 | 4 |
| Grade III | 9 | 6 | 7 | 6 | 1 | 2 | 0 | 1 |
| Grade IV | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 |
Additional post-procedural complications included masseter weakness in 4 (9.1%) patients in the PT-RFT group and in 3 patients in the coblation group. In addition, 1 patient in the PT-RFT group developed hypogeusia, and 1 patient had dysacusis after surgery. All patients improved during follow-up. No mortality was observed in these 50 patients.
Discussion
PT-RFT is widely used in the treatment of TN when drugs are ineffective or when adverse effects are intolerable [9]. As a minimally invasive technique, PT-RFT has the same efficacy as microvascular decompression (MVD), but with lower surgical risk [10]. However, postoperative facial numbness, a major complication of PT-RFT, limits this procedure [11]. The high temperatures, of over 65°C, are thought to selectively destroy the Aδand C pain fibers, as these are more susceptible to heat damage than Aα and Aβ tactile fibers [12]. Thus, the facial numbness after PT-RFT might be caused by the heat produced by the PT-RFT needle. In contrast to PT-RFT, coblation technology uses radiofrequency energy to excite the electrolytes in a conductive medium such as saline solution [13]. The coblation needle produces energized plasma that can break molecular bonds, causing tissue dissolution at a relatively low temperature (40–70°C) [14, 15].
Recently, coblation has been used in pain management for different conditions [6, 14–16]. In a case report of phantom limb pain, Li et al. found that coblation of the cervical nerve root successfully reduced the degree of pain [16]. Yang et al. reported on the efficacy of coblation of the thoracic paravertebral nerve for the treatment of thoracic neuropathic pain, and found that most patients experienced significant pain relief after surgery. Furthermore, all patients reported slight numbness after surgery, but the degree of numbness had no major impact on their daily lives [6]. Li et al. made a preliminary evaluation of the short-term efficacies of coblation and PT-RFT in treating ITN, and found that coblation reduced the risk of postoperative numbness, while reducing pain to the same degree as PT-RFT [7].
In this report, we compared the efficacy and rates of postoperative facial numbness of PT-RFT and coblation. Compared with patients in the PT-RFT group, the patients in the coblation group experienced similar pain relief, but with milder numbness; this was probably because the lower operating temperatures of coblation are less likely to damage surrounding nerves. Furthermore, the coblation needle is surrounded by normal saline as a conductive medium, which may also reduce damage to the surrounding tissue.