








Introduction
Inverted papilloma (IP) is a benign epithelial sinonasal tumor most commonly occurring in the maxillary sinus and the lateral wall of the nasal cavity. It has a potential for malignant transformation and a tendency for recurrence if incompletely removed. Multiple attachment is associated with increased risk of recurrence [1]. The majority of recurrences take place within 2 years. There is evidence suggesting that 5–10 years or even lifelong follow-up is needed, as 6% of IPs reoccur after 10 years [2]. Traditionally IP was removed using Denker’s approach or medial maxillectomy (via lateral rhinotomy or midfacial degloving). Currently the most commonly used endoscopic approach to the maxillary sinus IP is endoscopic medial maxillectomy. The endoscopic approach results in a lower recurrence rate. This can be attributed to better surgical vision compared to traditional approaches.
The potential complications of endoscopic medial maxillectomy include epiphora, crusting and empty nose syndrome. There is a growing number of studies confirming that the prelacrimal recess approach, which enables preservation of the inferior turbinate and nasolacrimal duct, is equally effective [3, 4]. Combined middle and inferior meatus antrostomies enable a good approach to the maxillary sinus including its anterior wall [5]. This approach can be insufficient in patients with prelacrimal recess involvement. However, it allows not only for preservation of the nasolacrimal duct and inferior nasal turbinate but also easy endoscopic follow-up. Currently available computed tomography (CT) and magnetic resonance imaging (MRI) imaging enables prediction of the site of tumor attachment and identification of patients who can benefit from the combined antrostomies approach [6].
Aim
The aim of this study is to evaluate combined middle and inferior meatal antrostomy approach in treatment of maxillary sinus inverted papilloma.
Material and methods
Retrospective assessment of medical records of consecutive patients operated on due to maxillary sinus inverted papilloma operated by a single operator was performed.
Exclusion criteria: recurrence of inverted papilloma after previous procedures with inferior turbinate removal. The university ethics committee approved the study.
Surgical technique
The surgical procedures were performed under general anesthesia. Pledgets soaked in adrenaline were applied in the nasal cavity, under the middle and inferior turbinate.
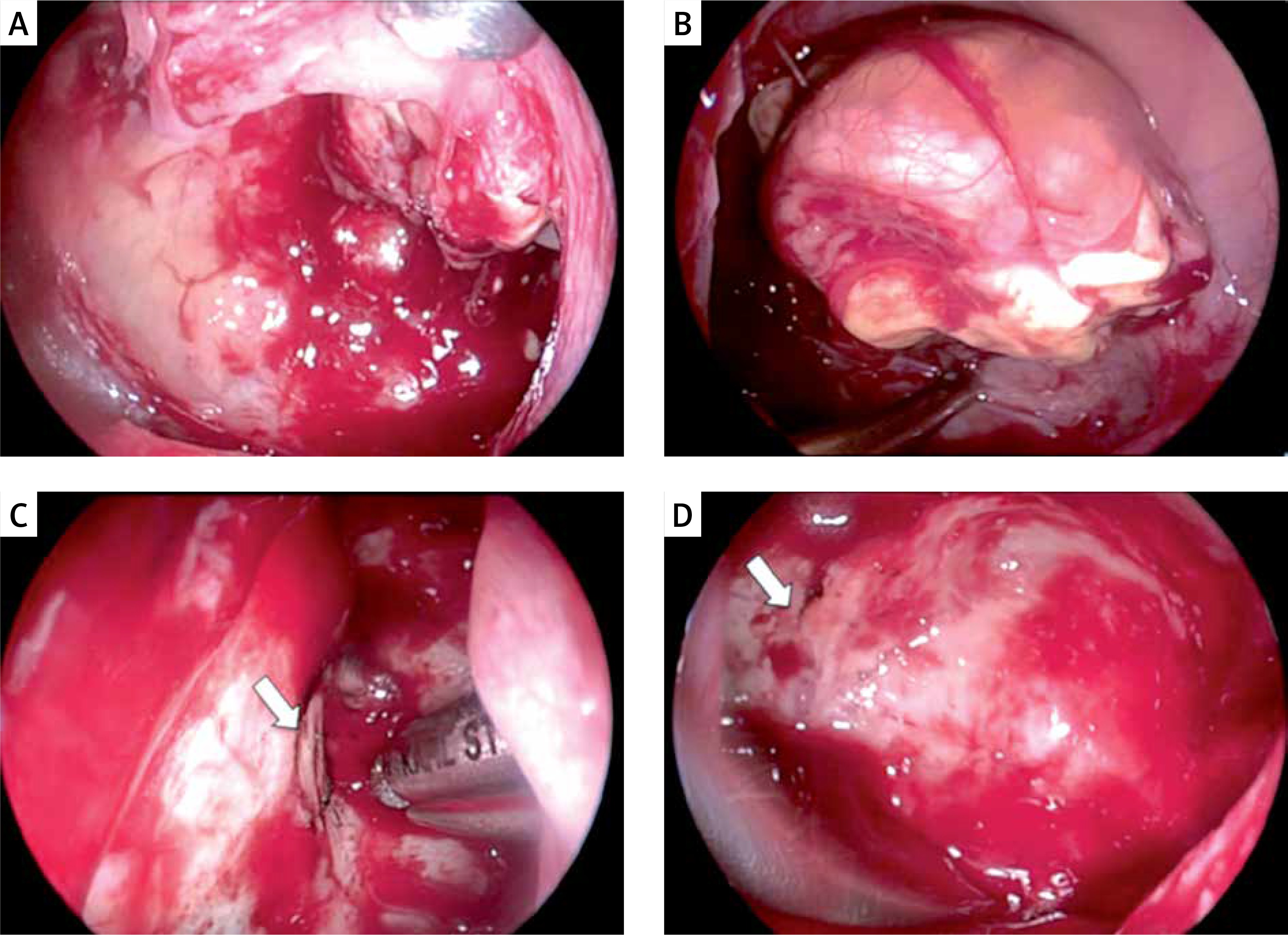
The axilla of the middle turbinate and the lateral nasal wall under the inferior turbinate were infused with 1% lidocaine and 1 : 100 000 adrenaline solution. The intranasal part of the tumor was removed (if present), then uncinectomy and wide middle meatal antrostomy (MMA) were performed (Photo 1 A). The free-floating part of the tumor was resected using angled forceps or a microdebrider. The maxillary sinus was inspected with 30, 45 and 70° rigid scopes or an adjusted viewing angle scope (0–90°). The inferior meatal antrostomy (IMA) was created typically 0.5 cm posterior to the anterior insertion of the inferior turbinate using the curette and cutting forceps. Care was taken to avoid stripping the mucosa and injuring Hasner’s valve. In case of anterior wall involvement the inferior turbinate was gently fractured and displaced medially to gain space for the endoscope and surgical tool, then the IMA was widened anteriorly using backbiting forceps and an irrigated diamond burr to the edge of the pyriform aperture. Resection of the middle wall of the sinus was tailored to the disease. If needed, middle and inferior antrostomies were merged together leaving the inferior turbinate suspended between its anterior and posterior attachment. Depending on anatomical conditions and location of the tumor attachment both antrostomies were used for sinus inspection and/or insertion of the surgical tools (Photo 1). After identification of the tumor pedicle, the surrounding mucosa was coagulated and removed, and underlying bone was drilled down with a curved diamond burr (Photos 1 C, D). Postoperative care included saline douches and debridement under endoscopic guidance 2 weeks postoperatively, and further regular endoscopic follow-up.
Photo 1
Intraoperative view of the left maxillary sinus. A – middle antrostomy view: the tumor is only partially visible, B – inferior antrostomy view: the tumor is much better exposed, C – removal of the tumor attachment: middle antrostomy view, the burr is introduced through the inferior antrostomy, D – the view through the inferior antrostomy at the end of the procedure. White arrow – infraorbital nerve
Results
From 2010 to June 2017, a total of 14 patients meeting the study criteria underwent surgery for maxillary sinus IP performed by a single operator (T.G). There were 7 women and 7 men, with a mean age 58.5 years (range: 47–76 years). Six of these patients were followed for 6 years or longer. Three patients were operated on due to IP recurrence including one after a previous Caldwell-Luc procedure and two after incomplete removal through the middle antrostomy (Table I). Preoperative imaging included CT and in 4 patients also MRI. Tumor attachment was identified on preoperative CT and/or MRI in 10 patients (Photos 2 and 3). Location of tumor pedicle and patient’s data are presented in Table I.
Table I
Summary of patient data (n = 14)
Photo 2
Preoperative CT and MRI (A, B) and postoperative CT (C) scans of patient no 8: red arrow – tumor attachment, white arrow – inferior meatal antrostomy, blue arrow – middle antrostomy
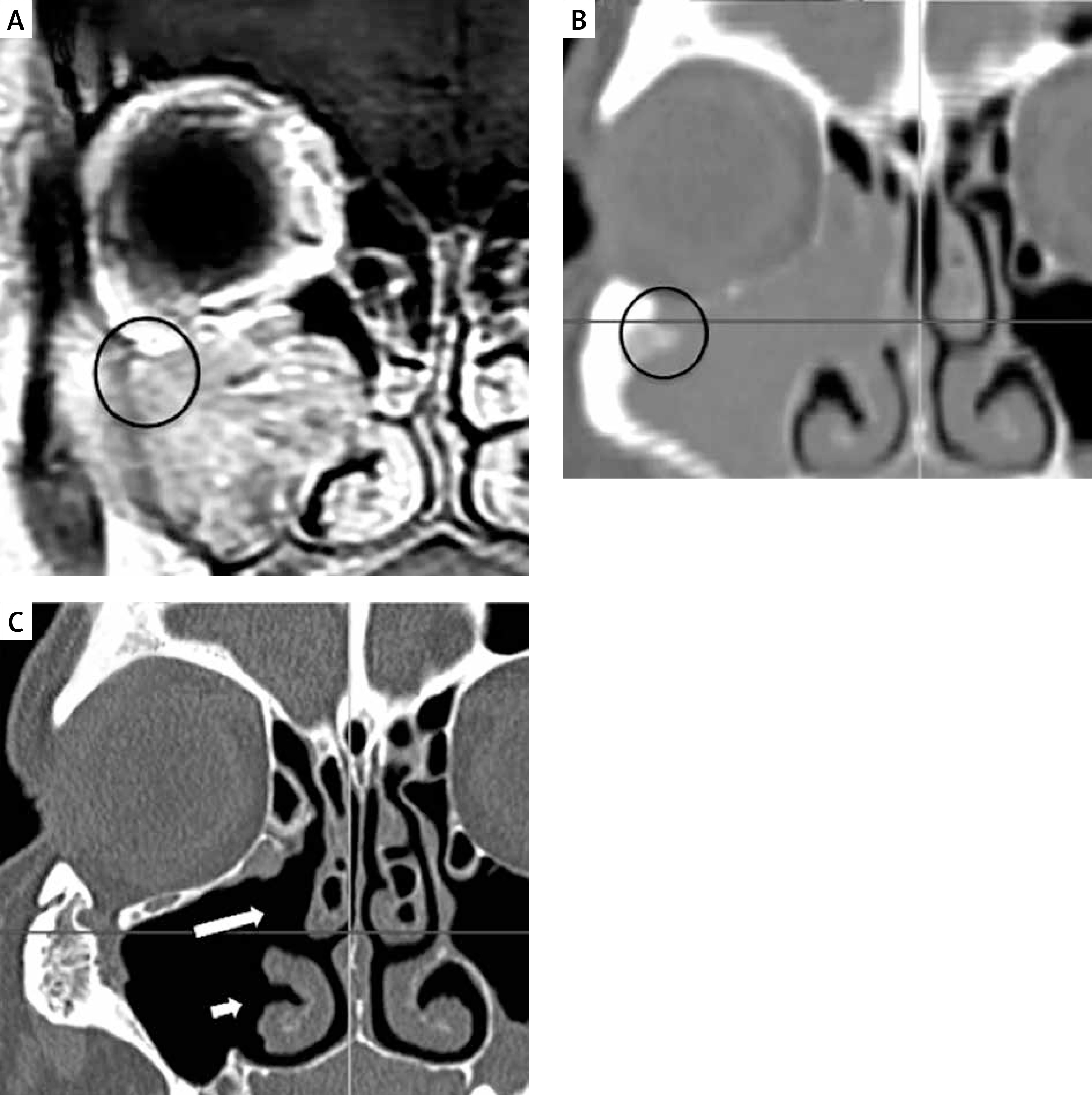
Photo 3
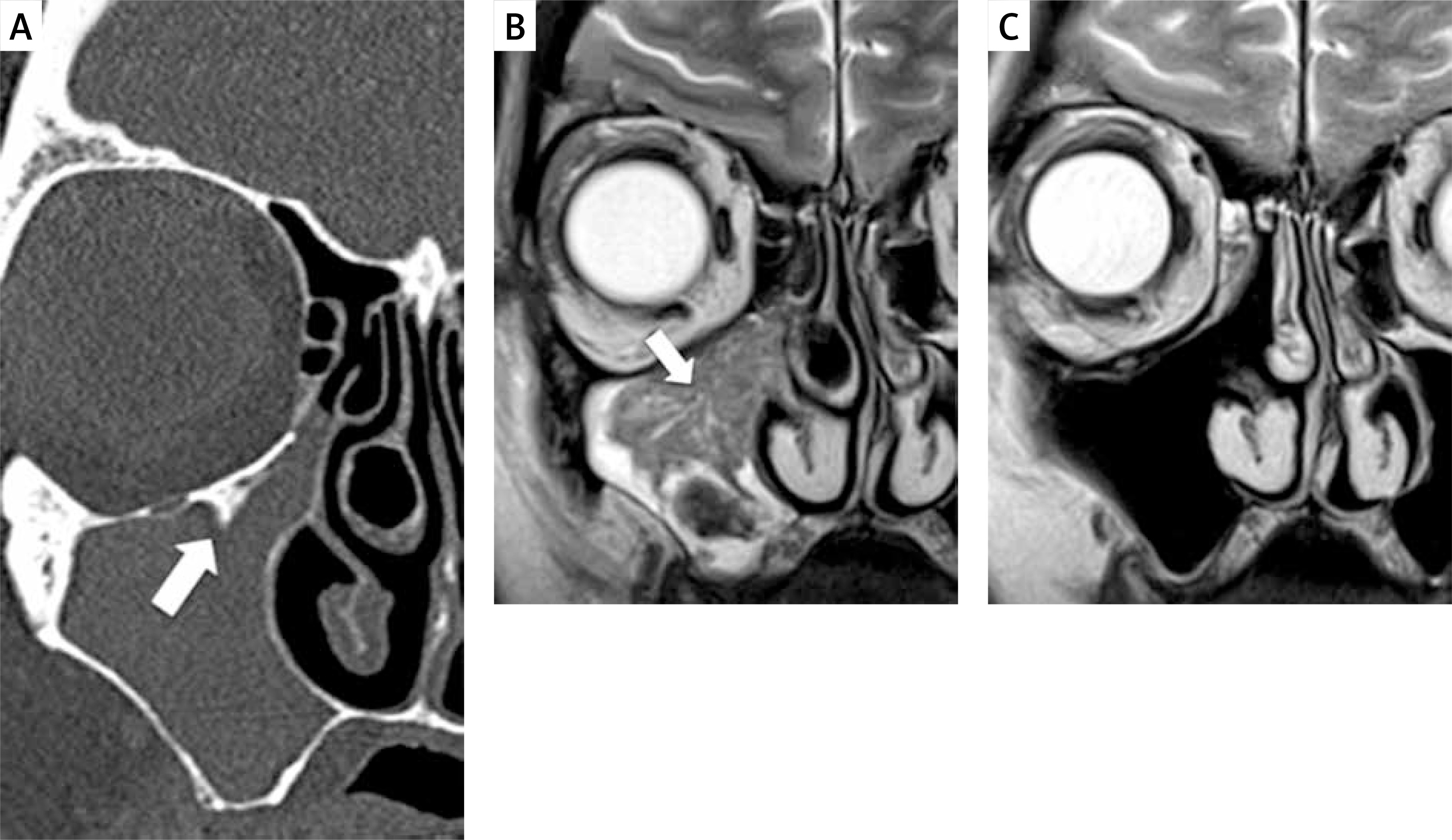
Preoperative CT (A) with dubious osteitis sign suggesting attachment – white arrow, and MRI with centripetal cerebriform pattern of attachment – white arrow (B). Postoperative MRI (C)
There were no cases with multifocal attachment or malignant transformation. In 1 of the 2 patients with prelacrimal recess involvement combined antrostomies allowed efficient control of the recess due to favorable anatomic conditions. In the second one combined antrostomies were supplemented by a prelacrimal approach.
Postoperative CT and/or MRI was performed in 11 patients. The three remaining patients were followed up with endoscopic examinations only. The postoperative follow-up was possible through IMA in 13 patients with a rigid scope. In most cases, there was no need for local anesthesia or decongestion. In 1 patient synechiae formation narrowed the middle antrostomy, making endoscopic follow-up with a rigid scope difficult.
No lacrimation, drying, empty nose syndrome, floppy turbinate or mucus recirculation was observed. Two patients with an IP pedicle attached to the infraorbital canal complained of permanent cheek numbness, which could be the result of drilling or use of diathermy. No recurrence was observed.
Discussion
The modified transnasal endoscopic medial maxillectomy (MTEMM) was described by Suzuki et al. in 2011 [7]. It provides wide access to the maxillary sinus including the prelacrimal recess and allows for removal of maxillary sinus tumors with preservation of the nasolacrimal duct and inferior nasal turbinate. Different variants of this procedure were presented in the literature in the following years.
Uniform nomenclature of these procedures is still not determined. However, it seems that the term “maxillectomy” is inappropriate since no part of the maxilla is removed.
“Prelacrimal recess approach” is currently the term most often used for this procedure. Recently Suzuki et al. presented results of treatment of 51 patients operated on for inverted papilloma using this method. The authors obtained good functional results with a low recurrence rate [3]. Piriform aperture enlargement performed to gain control over the anterior wall of the sinus in some of these procedures may cause collapse of the nasal valve and/or cosmetic deformity similarly as after the Denker approach. Zhou et al. observed this complication in 4% of 71 patients (mean observation of 37.3 months) [4].
Endoscopic postoperative follow up after the prelacrimal approach is possible only if wide MMA is performed. Visualization of the anterior part of the maxillary sinus is then possible only with the use of a fiberscope. This can be difficult due to the poor spatial orientation inside the sinus. Taking a biopsy under local anesthesia in these cases can also be problematic.
In 30% of patients the nasolacrimal duct is partially or completely fused with the anterior wall of the maxillary sinus, and the lacrimal recess is narrow or missing. In these cases the prelacrimal approach can be difficult to perform [8].
The IMA has been long known as an independent approach to the maxillary sinus or part of the Caldwell-Luc procedure. In the era of functional endoscopic sinus surgery it has been nearly abandoned, as it does not improve the natural drainage of the sinus. However, IMA offers good insight into the anterior part of the maxillary sinus [9] and provides an auxiliary aeration and drainage pathway [5, 10]. IMA does not affect natural ciliary transport from the maxillary sinus in presence of functioning natural ostium [11].
The combined antrostomies approach has been proven effective in treatment of a severely diseased maxillary sinus [10]. There were no cases of epiphora or floppy inferior turbinate in 34 patients treated with this method in 1-year observation.
This technique allowed us to use antrostomies as independent ports for the surgical tool and scope, which improved visibility and maneuverability within the sinus. In cases with attachment on the anterior wall IMA was used to introduce both the endoscope and the surgical tool. In our hands adequate visualization of the lower anterior and entire lateral wall of the maxillary sinus could be achieved at a 70–90-degree viewing angle after enlarging the IMA anteriorly to the level of the pyriform aperture.
In contrast, visualization and the possibility of introducing surgical tools to the prelacrimal recess was unsatisfactory in some patients.
In one of our patients with prelacrimal recess involvement (Photos 4 and 5) we managed to visualize the prelacrimal recess and remove the IP completely through the enlarged IMA due to favorable anatomical conditions (wide prelacrimal recess, short nasolacrimal duct). In the second patient, with a relatively narrow prelacrimal recess, we decided to extend combined antrostomies to the prelacrimal approach because of inadequate visualization of the medial wall of the nasolacrimal canal. There are no data on late functional outcomes of combination of these two approaches (combined antrostomies + prelacrimal recess) in a larger group of patients. However, the junction between the lateral wall of the nasal cavity and the floor of the nasal cavity is fractured during the pre-lacrimal approach anyway, so addition of inferior antrostomy should not be considered more destructive.
Photo 4
Intraoperative view of the right nasal cavity, maxillary sinus and prelacrimal recess (45° scope, patient 5). A, B – right nasal cavity view: yellow arrow – middle turbinate, blue arrow – inferior nasal turbinate, P – prelacrimal recess, C, D – enlarged inferior antrostomy view on the prelacrimal recess: IN – infraorbital nerve, H – Hasner’s valve
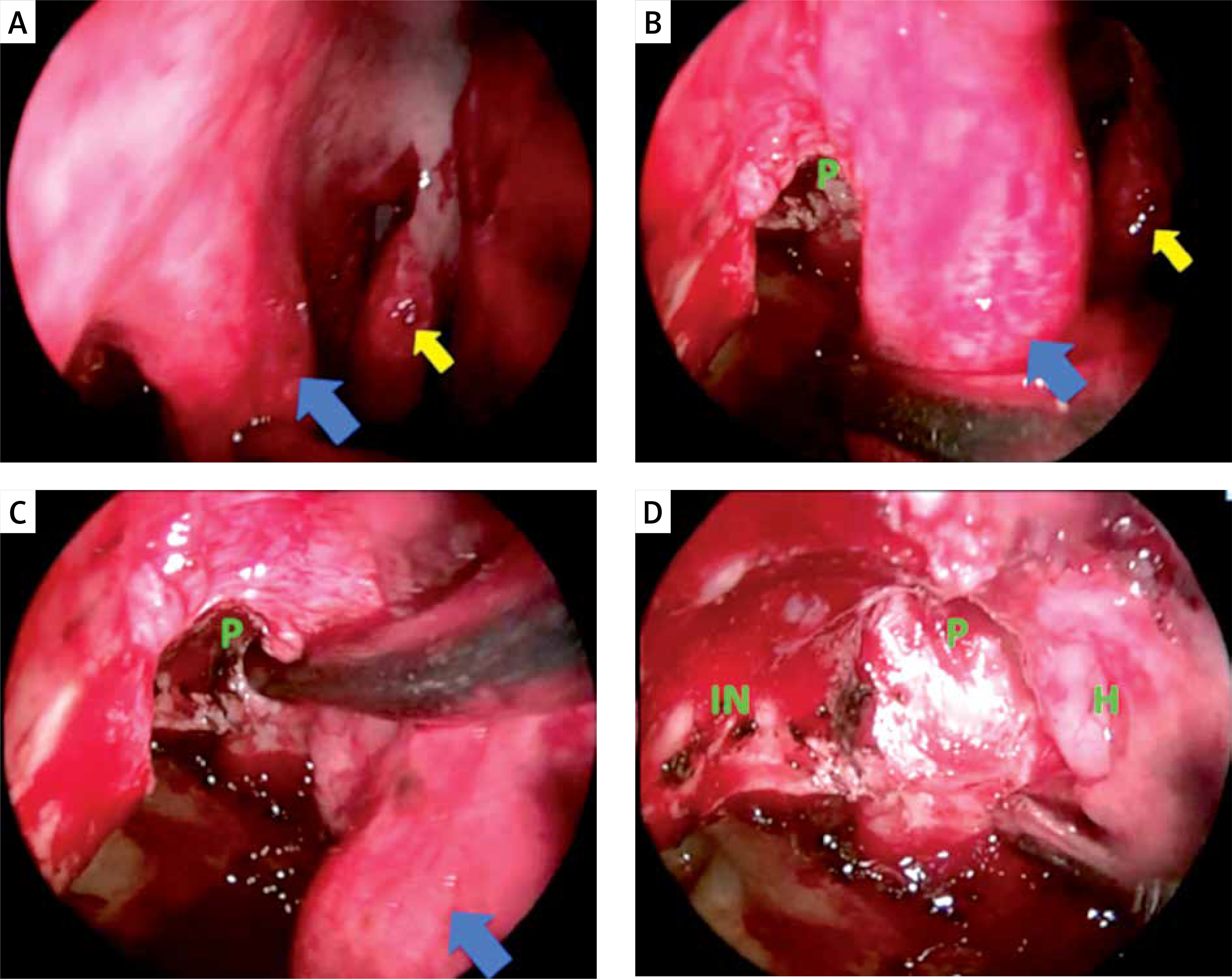
Photo 5
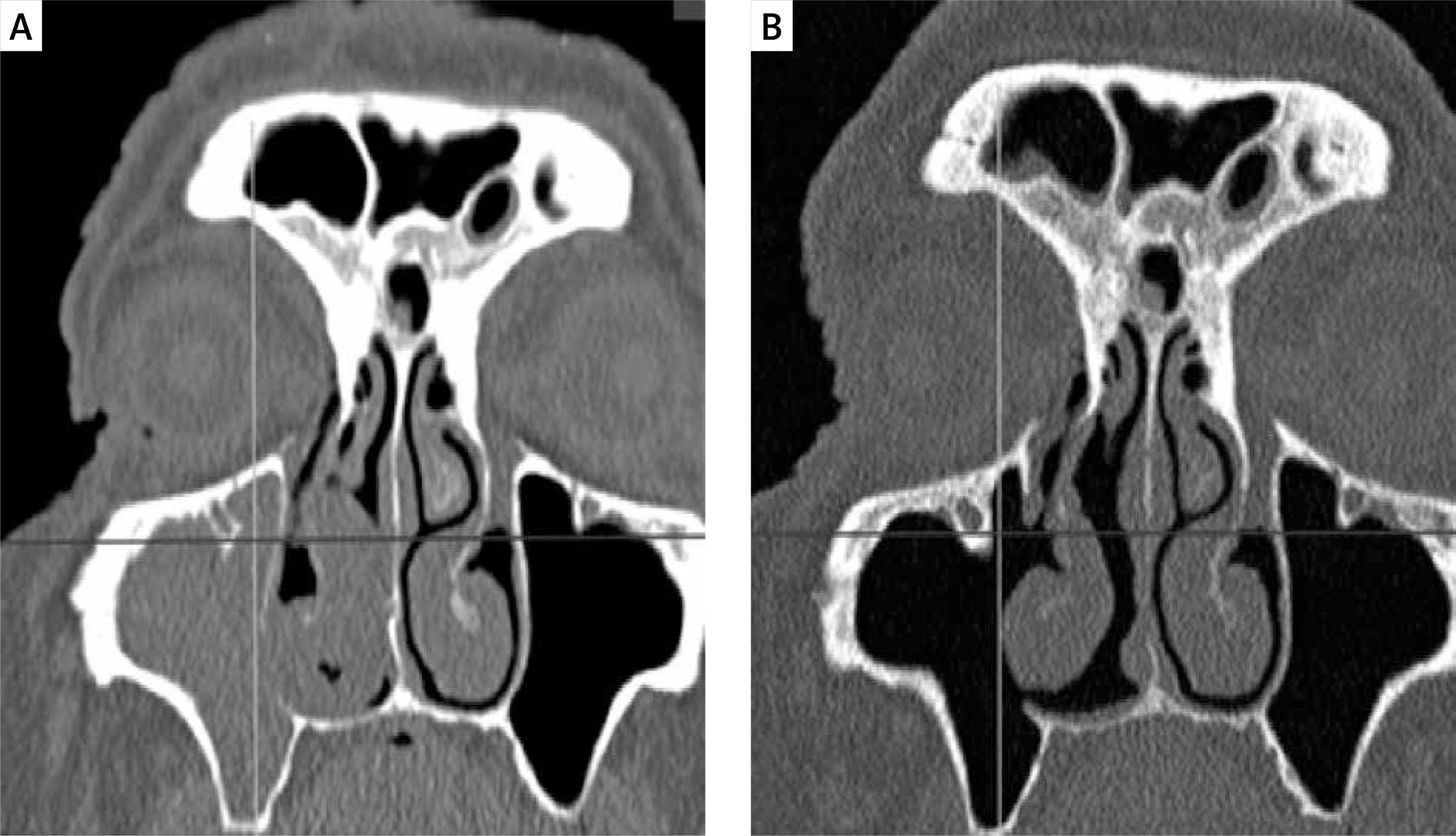
Patient with prelacrimal recess involvement from Photo 3 (patient 5): A – preoperative and B – postoperative coronal CT view
Combined CT and MRI assessment provides more useful information than using one of these techniques alone and increases the chance of identifying the attachment (Photos 2 and 3) [6]. In our study group we identified the attachment in 10 out of 14 patients preoperatively, although MR was available only in 4 of them. Thus involvement of the prelacrimal recess can be predicted in the majority of patients. In most primary IPs preoperative identification of the attachment allows for planned, patient-tailored endoscopic surgery (combined antrostomies or the prelacrimal approach). If the attachment is not visible on preoperative CT and MRI, we suggest starting the surgery with combined antrostomies. In case of inadequate prelacrimal recess control the next step should be the prelacrimal recess approach. Endoscopic middle maxillectomy should be used as the last option. There was no need for the transseptal approach, adjuvant Caldwell-Luc approach, or endoscopic middle maxillectomy in our patients. However, the small number of subjects is the major limitation of our study. In patients with involvement of the deep alveolar recess, multiple attachment sites or carpet-like growth over a large area, combined antrostomies would probably be insufficient.
Conclusions
The combined antrostomies approach is effective and safe in treatment of maxillary sinus inverted papilloma. It seems superior to medial maxillectomy, as it is associated with lower morbidity. It offers the possibility of easy endoscopic follow-up through inferior antrostomy in contrast to the prelacrimal approach. Preliminary data suggest that in case of pelacrimal recess involvement this approach can be safely extended to the prelacrimal approach.