Introduction
Respiratory distress in neonates is the commonest disorder in the first 48 to 72 hours of life, with a wide range of underlying causes. It affects up to 7% of all term newborns and is increasingly common in even modest prematurity [1]. Preventive and therapeutic measures for some of the most common underlying causes are well studied and when implemented can substantially reduce the mortality and morbidity of disease [2-4]. Transient tachypnoea of the newborn (TTN) is frequently encountered in preterm neonates with respiratory distress. It is caused due to incomplete resorption of fluid from the lung in preterm neonates, which leads to respiratory distress. It is a self-limiting condition, which usually resolves within 24 to 48 hours and only needs supportive treatment. Thus, in the early neonatal period it becomes crucial to differentiate TTN from other causes of respiratory distress.
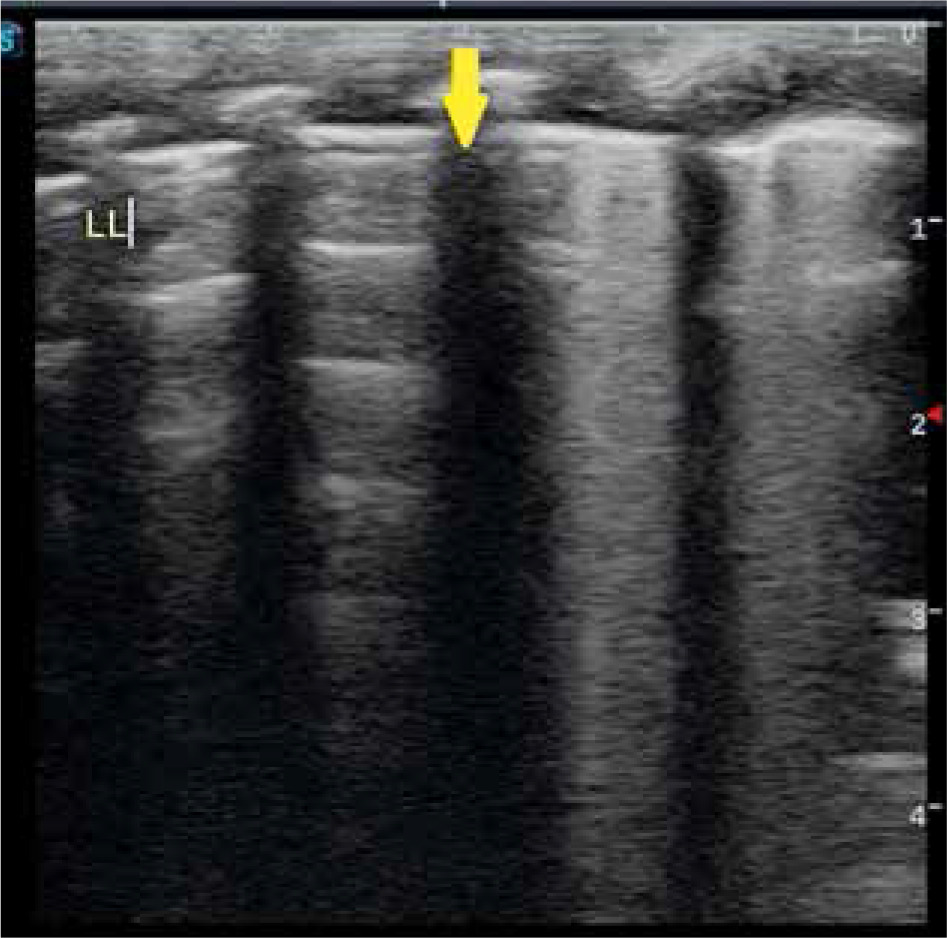
In the past, ultrasonography was not used widely for neonatal chest imaging because of the obscuring artifacts generated by the air-filled lung. Lung ultrasound (LUS) has recently emerged as a promising diagnostic tool, with studies reporting accurate results in the diagnosis of respiratory distress syndrome [5-7]. Ultrasonography also does not pose a risk of exposure to ionising radiation, unlike chest radiography. In the recent literature a new ultrasonographic finding called double lung point (DLP) sign is seen in neonates with TTN. It is seen on ultrasonography as transition in echoes between the upper and lower lung fields with a frank demarcation point (Figures 1 and 2). DLP was only observed in infants with TTNB and not in infants with RDS [8,9].
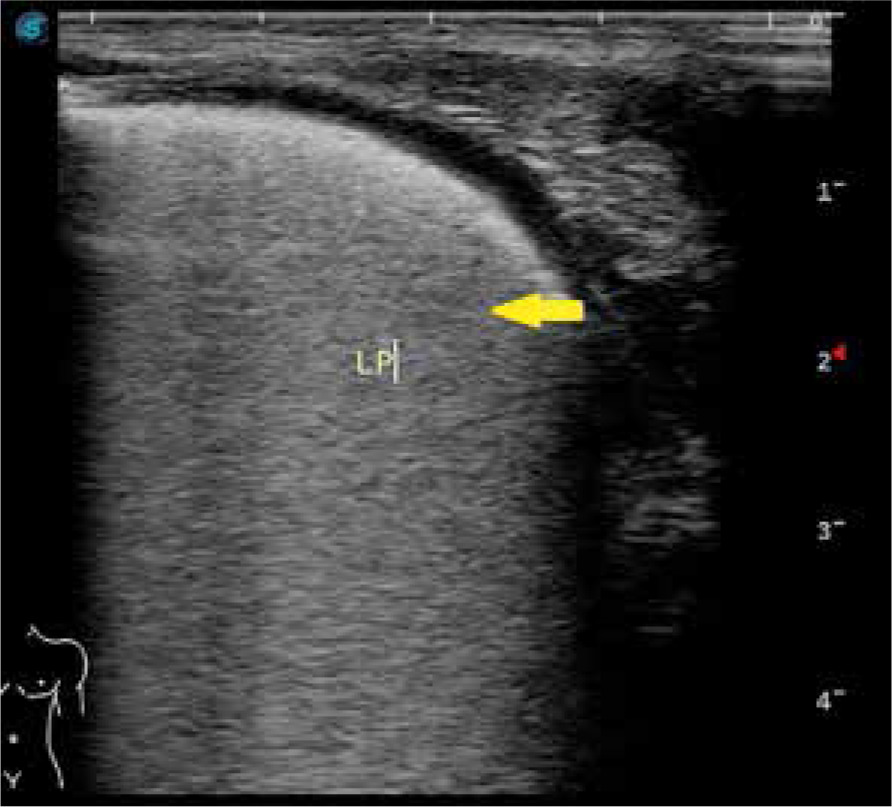
Figure 1
Longitudinal view of left posterior lung field showing abnormal B-lines in basal zone and normal A-lines in upper zone with the sudden transition point marked with the arrow, this is called as the double lung point sign
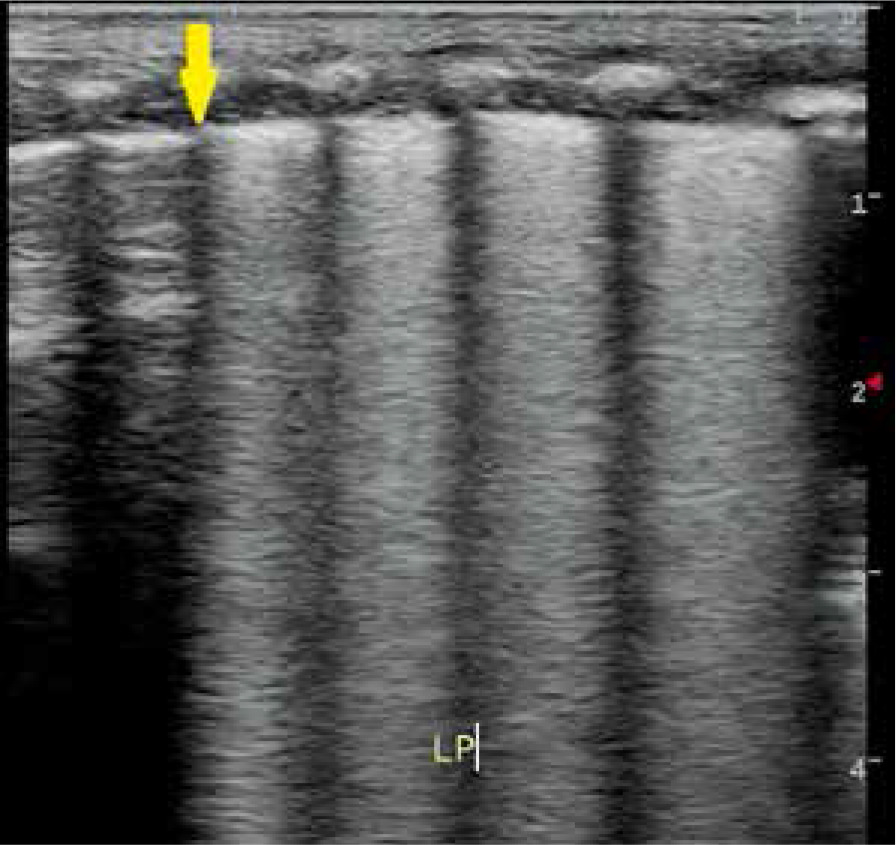
Figure 2
Longitudinal view of left posterior lung field with the arrow showing double lung point sign
Very few studies have been done in the recent past to know the role of DLP in diagnosing TTN in preterm neonates. In a study conducted by Copetti et al. [10] lung ultrasonography was performed in 32 neonates with radiological and clinical signs of TTN within the first hour of birth, and they were compared with those of 60 normal neonates. They found that the sensitivity and specificity of double lung point sign was 100% for the diagnosis of TTN, and it was also concluded that lung ultrasound is reliable for the early diagnosis of TTN. In another study conducted by Liu et al. [11] from 2013 a total of 60 infants who were clinically diagnosed with TTN were enrolled in the study, and ultrasonographic findings were compared to 40 hospitalized neonates without lung disease and with 20 neonates with respiratory distress syndrome. In their study the common ultrasonographic findings of TTN were double lung point, interstitial syndromes or white lungs, pleural line abnormalities, and A-line disappearance. The study showed that DLP had a sensitivity and specificity of 76.7% and 100%, respectively, for diagnosis of TTN.
In a recent study aimed to evaluate the diagnostic value of lung ultrasonography for early diagnosis of TTN and to differentiate it from other causes of neonatal respiratory distress, conducted by Ibrahim et al. [12], 65 neonates were enrolled. Lung ultrasonography was performed within 12-24 hours of admission in NICU. It was found that double lung point had a sensitivity of 69.6% and specificity of 100% for detecting TTN. Thus, this study was done to evaluate the diagnostic accuracy of DLP in diagnosing TTN and to calculate its sensitivity and specificity.
Material and methods
All preterm neonates with respiratory distress as defined by tachypnoea (RR > 60/min), retractions and/or grunting were considered eligible for the study. After obtaining informed written consent, detailed history regarding the gestational age at the time of delivery, mode of delivery, antenatal history of any maternal illness, and antepartum haemorrhage, clinical diagnosis was made by the paediatrician using a combination of clinical indicators like presentation, vital signs, auscultation, laboratory blood gas analysis, and chest X-rays (CXR). Bilateral chest ultrasonography was performed with a multifrequency linear transducer with a bandwidth of 6-12 MHz using a Philips HD7 XE and a Sonoscape S2 portable colour ultrasound machine, using a 6-12 MHz linear probe in the neonatal intensive care unit of the paediatric department within 6 hours of birth. In resting state, each patient was placed in supine, lateral, or prone position (Figure 3). Using the anterior and posterior axillary lines as boundaries, each side of the lung was divided into 3 regions: anterior, lateral, and posterior. The probe was placed parallel and perpendicular to the ribs, and each region of both sides of the lung was carefully scanned in longitudinal and transverse plane. All the ultrasonography examinations were performed by one doctor. To prevent hypothermia the babies were put under a radiant warmer or incubator during the scans. The observations were recorded. Based on the ultrasound findings, the diagnosis was suggested.
Figure 3
Chest X ray AP view of a neonate. Prominent vascular markings are seen in perihilar region (yellow arrow) consistent with TTNB

Statistical analysis
Study data were collected using a specially designed and tested proforma. Data were entered in a spreadsheet and checked for accuracy and incompleteness. Data were imported into and analysed using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, version 15.0 for Windows). Continuous variables that were normally distributed were expressed as mean and standard deviation. Categorical variables were expressed as number and proportion. The mean was calculated for all quantitative variables. Parametric or non-parametric tests of comparison were used to compare ultrasound and CXR diagnoses. The diagnostic accuracy of ultrasound was estimated by calculating the sensitivity, specificity, and positive and negative predictive values. Qualitative or categorical variables were described as frequencies and proportions. Proportions were compared by using the likelihood ratio or c2 test, whichever was applicable.
Results
A total of 104 preterm neonates of either sex, who presented with respiratory distress at the time of birth from December 2017 to June 2019 were enrolled in the present study, out of whom 100 were included in the study. Two preterm neonates were excluded from the study because they died before CXR could be performed. Two preterm neonates left against medical advice within 6 hours of birth, before ultrasonography. Lung ultrasonography of 55 preterm neonates with radiological and clinical signs of TTN within the 6 hours of birth were compared with those of 45 non-TTNB neonates. The method used by Copetti et al. [10] was used as a reference method in our study.
Frequency charts were computed for demographic data, such as gestational age, sex, and mode of delivery. Cross tables were made to compare the ultrasound diagnosis with the clinical diagnosis (Table 1). The diagnosis made using clinical signs, symptoms, arterial blood gas analysis, and CXR was established as a reference standard.
Table 1
Diagnostic test characterization of ultrasound with clinical diagnosis of transient tachypnoea of newborn (TTN)
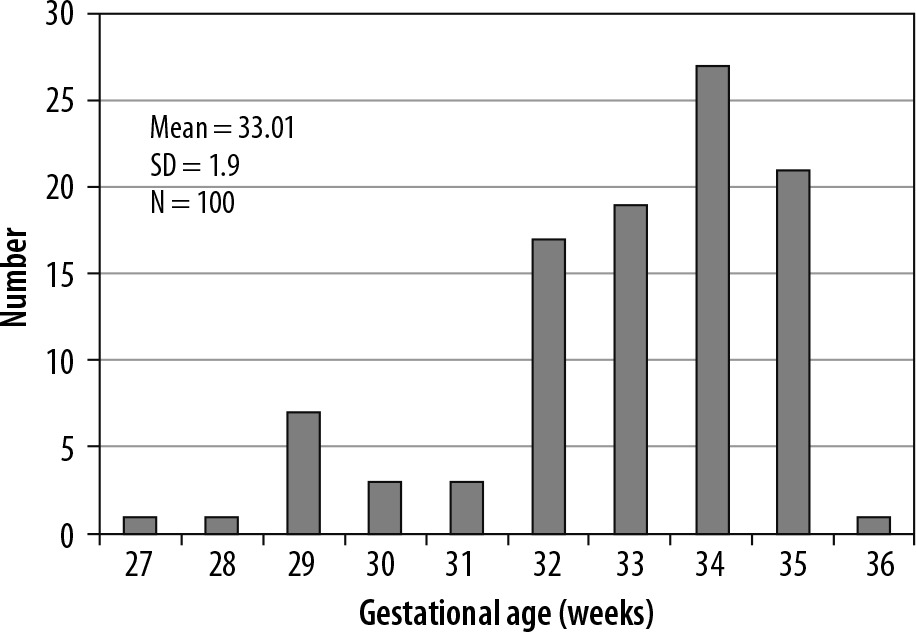
The gestational age of these preterm neonates ranged between 27 weeks and 36 weeks (Figure 4). The mean gestational age was 33 ± 1.9 weeks, and 80% of the cases belonged to the gestational age group 32-35 weeks.
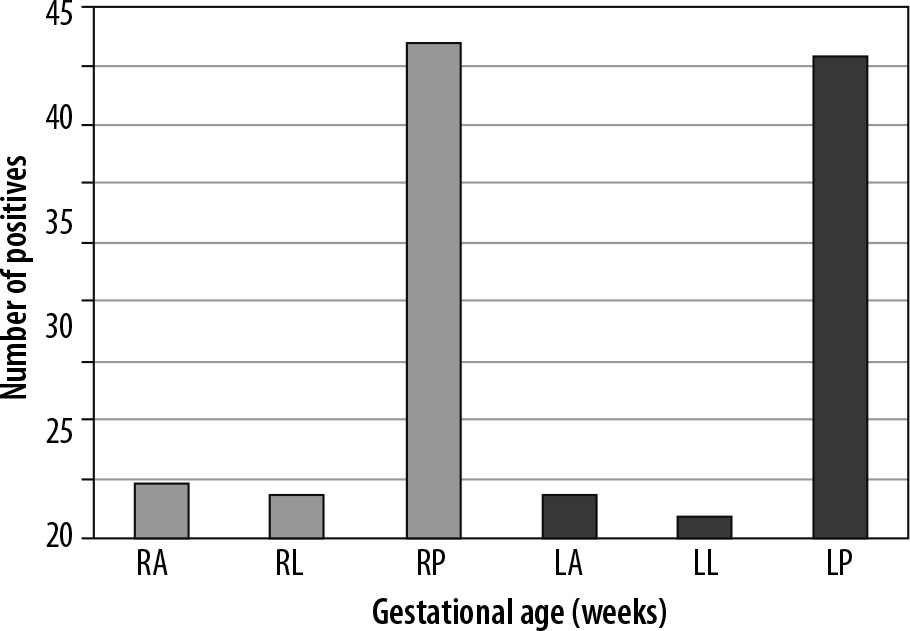
The majority of preterm neonates in our study were delivered via caesarean section (n = 76), and the remaining 24 preterm neonates were born through normal vaginal delivery. Double lung point sign was present in 50 preterm neonates in our study. It was most common in bilateral posterior lung fields. Approximately 41% of neonates showed double lung point sign in posterior lung fields (right posterior = 42; left posterior = 41). Double lung point was seen least often in left lateral lung field (n = 2) (Figure 5).
On comparing the ultrasonographic diagnosis with clinical diagnosis, the sensitivity and specificity of ultrasound in diagnosing TTNB was 85.9% and 94.4%, respectively. The positive predictive value was 96.4% and negative predictive value was 79%. The positive likelihood ratio was 15.339 and negative likelihood ratio was 0.148.
Discussion
TTNB often creates a diagnostic dilemma for clinicians because its pattern of presentation and clinical signs is similar to that of other neonatal respiratory diseases. Hence, it is crucial to correctly diagnose the cause of respiratory distress in the early neonatal period, which further helps in providing appropriate treatment such as lung surfactant therapy or antibiotics. In our study we used a transthoracic method of lung ultrasonography in the early neonatal period because the size of neonatal chest and chest wall muscles is less than that of adults; high-quality images were obtained. In previous studies using lung ultrasound in newborns, Avni et al. [13, 14] and Pieper et al. [15] utilized an abdominal approach of ultra-sonography to diagnose respiratory distress syndrome.
The mean gestational age of the patients enrolled in the study was 33 ± 1.9 weeks (range: 27-36 weeks). Most of the patients belonged to the age group 32-35 weeks, constituting about 80% of the total study population. There was no significant association between the ultrasound diagnosis and the age of the patient. This is in agreement with the observation made by Abdelsadek et al. [10]. In their study, 40 preterm neonates were evaluated, and the mean gestational age in the studied groups ranged from 28 weeks to 36 weeks with the mean of 32.9 ± 2.057 weeks 33 weeks; the incidence and severity were inversely related to the gestational age of the neonate. A total of 58 males and 42 females were included in the study. The male-to-female ratio was 1.4 : 1. There was higher predominance of respiratory distress in males as compared to females. This is in agreement with observations made by Mlay and Maitji [16], who in their study found that respiratory distress syndrome is more in males than in females. A study done by Abdelsadek et al. [17] revealed the predominance of respiratory distress syndrome, in which 27 out of 40 neonates were male. The study also revealed a significant difference between male and female neonates, with a p-value < 0.013.
Out of 100 preterm neonates enrolled in the present study, 76 were delivered through caesarean section, and the remaining 24 neonates were delivered through normal vaginal delivery. On ultrasonography, normal lung shows A-lines, which are the horizontal, echogenic, reverberation artifacts that occur beneath the pleural line (Figures 6 and 7). The abnormal B lines were seen in 52 (68%) neo-nates, 76 of whom were delivered through caesarean section. This is in concordance with the study done by Levine et al. [18], who found that newborns delivered by caesarean section have a fivefold increase in the incidence of respiratory disorders and persistent pulmonary hypertension than those delivered vaginally.
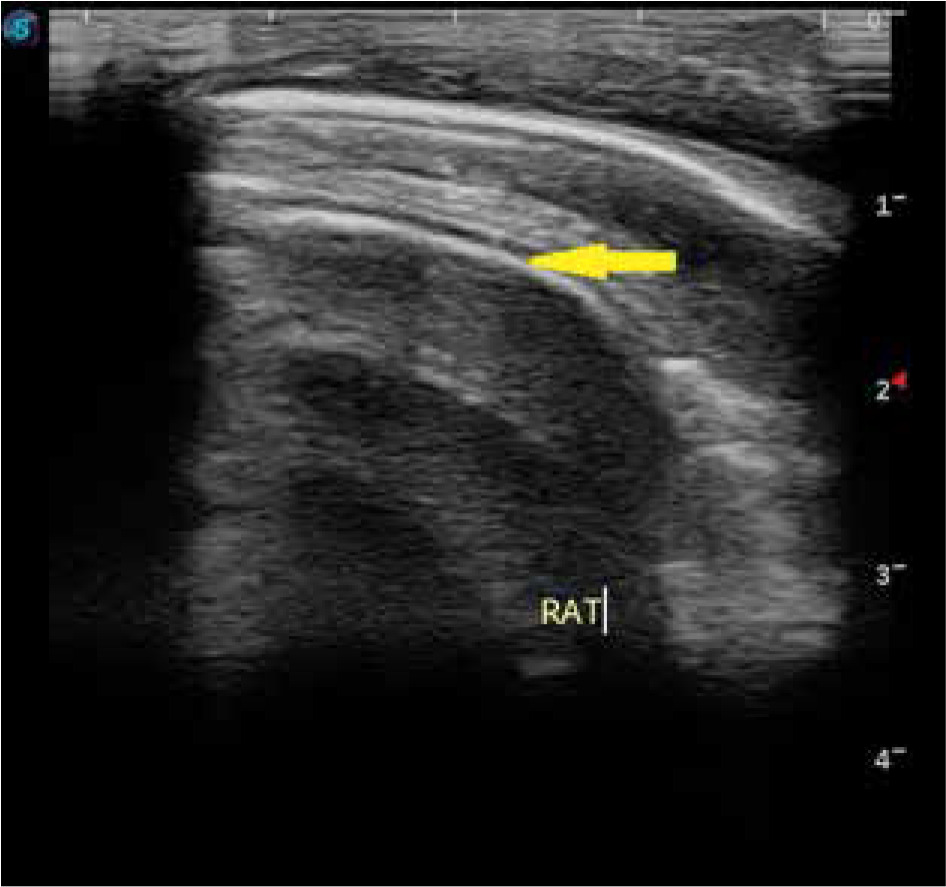
Figure 6
Transthoracic longitudinal view of right anterior lung field. A-line marked with blue arrow and yellow arrow shows rib shadow
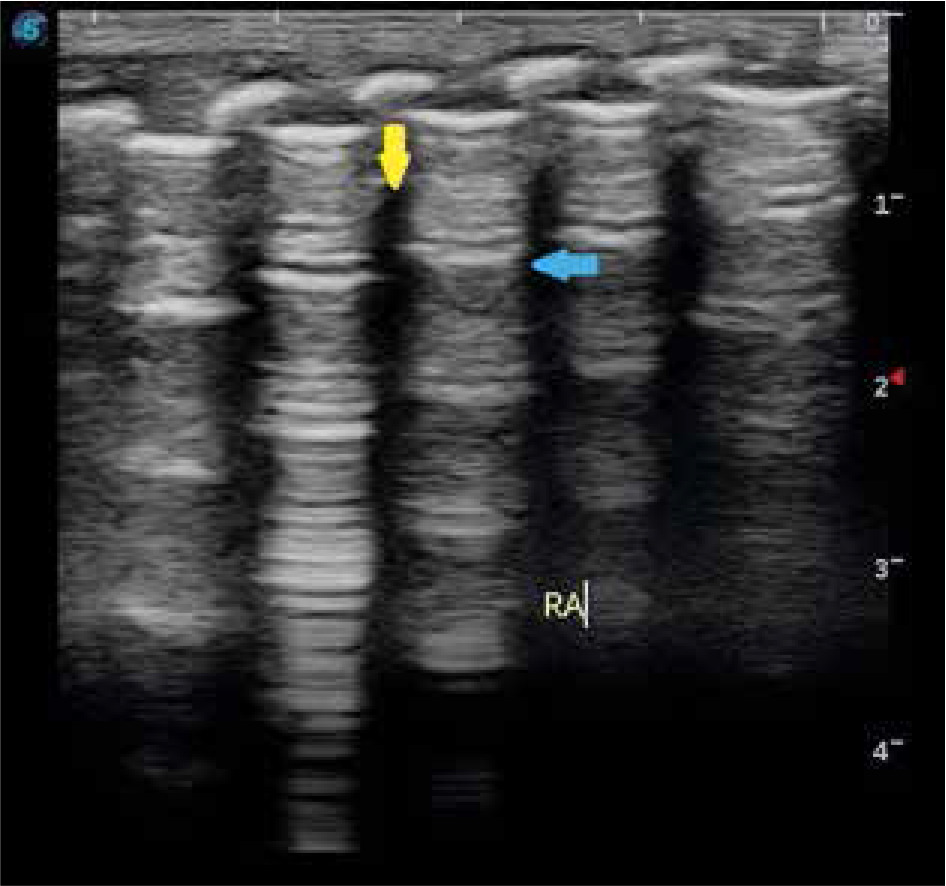
Figure 7
Transthoracic transverse view of right anterior lung field with the arrow showing normal A-lines
B-lines are abnormal line-like artifacts arising from, and perpendicular to, the pleural line, which present as radial divergences to the deep parts of the lung field [19]. In the present study more than two-thirds of the patients showed the presence of B-lines distributed in all the 6 regions (Figures 8 and 9). In our study B-lines were seen predominantly in the bilateral posterior lung fields. However, in a study conducted by Copetti et al. [20], 40 newborns underwent ultrasound, and it was observed that B lines were predominant at the lung base at 36 weeks gestational age in infants who did not receive oxygen therapy at that age. On the other hand, in the infants with oxygen therapy, nonhomogeneous distribution of B-lines was observed.
Figure 8
Transthoracic longitudinal view of right posterior lung field showing multiple B-lines with disappearance of normal A-lines

Double lung point (DLP) sign was the main diagnostic index for TTN in our study, and it was present in 55 premature neonates on ultrasound. The sensitivity and specificity of DLP in diagnosing TTN in our study was 85.9% and 94.4%, respectively (Table 1). It was most commonly present in bilateral posterior lung fields (Figures 5, 8, and 9). DLP was seen least in the left lateral lung field (n = 2). This is in concordance with a study by Liu et al. [11], which reported the sensitivity and specificity of DLP in diagnosing TTN as 76.7% and 100%, respectively. However, in a large sample study conducted by Liu et al. [17], it was found that DLP was not specific for TTN, as DLP was also seen in other conditions like RDS and pneumonia. The sensitivity and specificity of DLP in diagnosing TTN in their study was reported to be 45.6% and 94.8%, respectively. This variability may be due to the larger sample size of their study. In a study conducted by Copetti et al. [10], it was found that DLP was present in all infants with TTN, with a high the sensitivity and specificity of this sign, i.e. 100%.
Limitations of study: Although high sensitivity and specificity of DLP was found in diagnosing TTN, careful blinding is required, and it should include significant numbers of neonates with a variety of other respiratory disorders. In cases of TTN that are associated with consolidation (pneumonia) DLP sign cannot be seen on ultrasonography, thus leading to false negative results. Because of these limitations in the present study, we believe that further multicentric large-scale studies are required to confirm the sensitivity and specificity of DLP.
Conclusions
It was found in our study that double lung point is the primary ultrasound characteristic of TTN and ultrasound findings were more predominant in bilateral posterior lung fields. Lung ultrasound can accurately and reliably diagnose TTN using DLP. Thus, lung ultrasound could be used as a screening tool in NICUs for lung and it can substitute the use of CXR in certain lung pathologies like TTN and RDS. However LUS techniques require properly trained staff with the appropriate equipment before it can be routinely used.