
Introduction
In many clinical situations, a quick diagnosis is required, and the introduction of more user-friendly miniature ultrasound scanners can significantly influence the outcomes. Recently, a new class of pocket size imaging devices (PSID) became available – an ultrasonic probe that can be connected directly to a personal mobile device such as a mobile telephone or a tablet with a dedicated application. Studies concerning the use of the previous generation of PSID have shown that although they do not provide all imaging modes, such as the pulsed wave Doppler technique, the benefits of their use in clinical practice are clear. An unquestionable advantage is the ability to immediately obtain information about morphology and heart function in practically every possible clinical environment [1, 2]. The recommendations of the European Association of Cardiovascular Imaging regarding pocket echocardiography indicate that this device can be used as a quick screening tool and as a supplement to physical examination [3]. Echocardiography performed at bedside using the PSID can immediately complement the results of physical examination and improve its diagnostic accuracy.
A new interesting feature is tele-echocardiography – a possibility of internet connection with other users and collaboration in real time by sharing devices’ camera, voice, and ultrasound images. Therefore, we have attempted to investigate the feasibility and clinical utility of focused echocardiographic examination performed by an inexperienced operator using PSID and collaborating remotely in real time with a cardiologist by means of tele-consultation.
Material and methods
Study population
The study group consisted of 30 patients (18 men and 12 women; mean age: 54 ±14 years (24–74 years; mean body mass index (BMI): 27 ±6 kg/m2), 12 of whom were admitted to the Department of Infectious Diseases, 10 were admitted to the Department of Internal Diseases and 8 were patients of the Department of Cardiology. Study population characteristics and main indications for echocardiographic examinations are listed in Table I.
Table I
Study population characteristics and indications for echocardiographic examinations (n = 30)
Pocket size imaging device
We used a Lumify echocardiograph (Philips Healthcare, Andover, USA), which is a PSID based on the microUSB probe S4-1 (4 to 1 MHz extended operating frequency range) which can be connected to a personal mobile device (tablet or smartphone, Figure 1) with a dedicated application. In our study the microUSB probe was connected to a tablet with a 10.1-inch screen. It includes an integrated tele-ultrasound solution (Reacts) that allows real-time transfer of the image to an Android-based phone and collaboration with an experienced cardiologist, as well as sharing of the camera image and voice recording. The PSID was connected to the internet by Wi-Fi, whereas the cardiologist’s mobile device was connected by means of the telephone network.
Figure 1
Personal mobile device-based pocket echocardiograph – microUSB probe S4-1 connected to a tablet

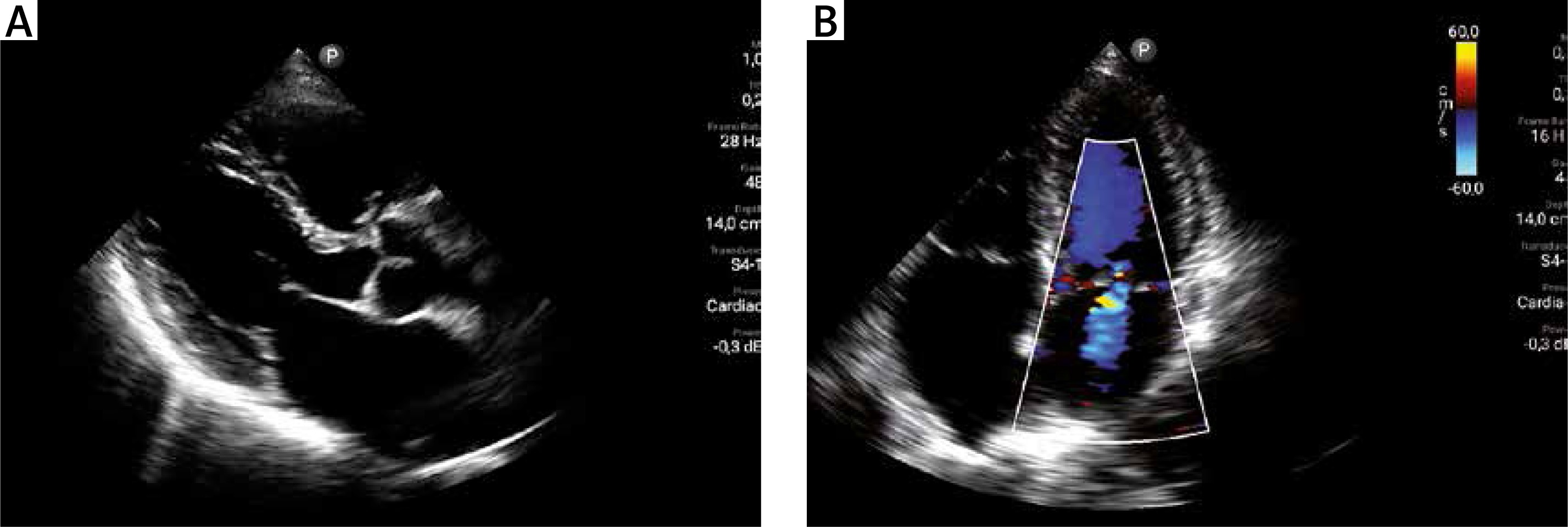
The available imaging modes included two-dimensional greyscale multivariate harmonic imaging (with a possibility of linear measurement), color Doppler mode (Figures 2 A and B), and additionally M-mode imaging – an option not available so far in PSID. Images can also be digitally stored and later reviewed.
Study protocol
All patients underwent a focused transthoracic echocardiographic examination (fTTE) performed with the use of PSID by one of three persons who were not previously trained in the field of echocardiography: a nurse and two students (each performed ten fTTEs). Before commencing the examination, the operators underwent 1 h of training in use of the Lumify application and placing the probe in typical sites on the chest to obtain the apical and parasternal views.
During the fTTE an operator collaborated in real time with an experienced cardiologist by means of tele-echocardiography. The cardiologist viewing the echo images provided feedback on how to arrange the probe to get a better view, e.g. “tilt the probe more to the right”, “move it closer to the sternum”, etc.
Each examination included standard parasternal and apical views. The feasibility of obtaining diagnostic quality of 4 basic views (parasternal long axis view, and apical: 4-chamber view, 2-chamber view and 3-chamber view) was noted. Quality (the possibility of interpretation) of acquired images was graded as acceptable or unacceptable. The duration of the examination was recorded. Basic, approximate measurements and major findings were saved and noted. As exemplary linear measurements (only three measurements so as not to extend the test time), aortic, left atrial and left ventricular diastolic dimensions were measured by the operator. The person collecting the images also measured the tricuspid annular plane systolic excursion (TAPSE) to assess the right ventricular function. The measurements were performed manually by the operator collecting echocardiographic images, but this process was remotely supervised in real time and guided verbally by an experienced cardiologist. Left ventricular (LV) function was evaluated visually (by a cardiologist) and regional wall motion abnormalities were described (hypokinesis, akinesis or dyskinesis). Evaluation of the heart valves was done by a cardiologist and was based on a visual assessment of the presence of organic lesions (such as valve thickening, calcification, reduced leaflet mobility or prolapse) and using the color Doppler mode. Turbulence or the presence of regurgitant jet was also noted and together with valve morphology interpreted as valvular regurgitation or stenosis.
Within 24 h of fTTE, beside examination, all patients underwent standard transthoracic echocardiographic (TTE) examination, which was performed by another experienced cardiologist (level III of the ASE), blinded to the results of the fTTE, using a full sized high-end echocardiograph and all imaging modes available (M-mode, grayscale imaging, color Doppler, pulsed wave Doppler, continuous wave Doppler, tissue Doppler imaging).
Statistical analysis
Continuous and categorical variables are expressed as mean ± SD and as percentages (%), respectively. Continuous variables were initially tested for normality of data distribution by the Kolmogorov-Smirnov test. Parametric Pearson correlation (r) was used for the continuous values to estimate correlation coefficients between the analyzed groups. The results were considered to be statistically significant at p less than 0.05. For the evaluation of parametric data the inter-rater agreement κ test was used.
Results
Focused TTE was feasible in all patients. However, all basic views (parasternal PLAX view and 3 apical views) could be obtained only in 70% patients. Acceptable image quality – sufficient for diagnostic use – for parasternal view was obtained in 21 (70%) patients, for 4-chamber view in 24 (80%) patients, for 3-chamber view in 22 (73%) patients and for 2-chamber view in 18 (60%) patients. The most common problem was obtaining the correct 2-chamber view without shortening the LV apex.
The average time required for fTTE was 720 ±240 s. The differences between the time of examination for three operators were not statistically significant (p < 0.05). A slight reduction in the time needed for the examination was noted in the course of this study (for tests 8–10 compared to tests 1–3), but without a statistically significant difference.
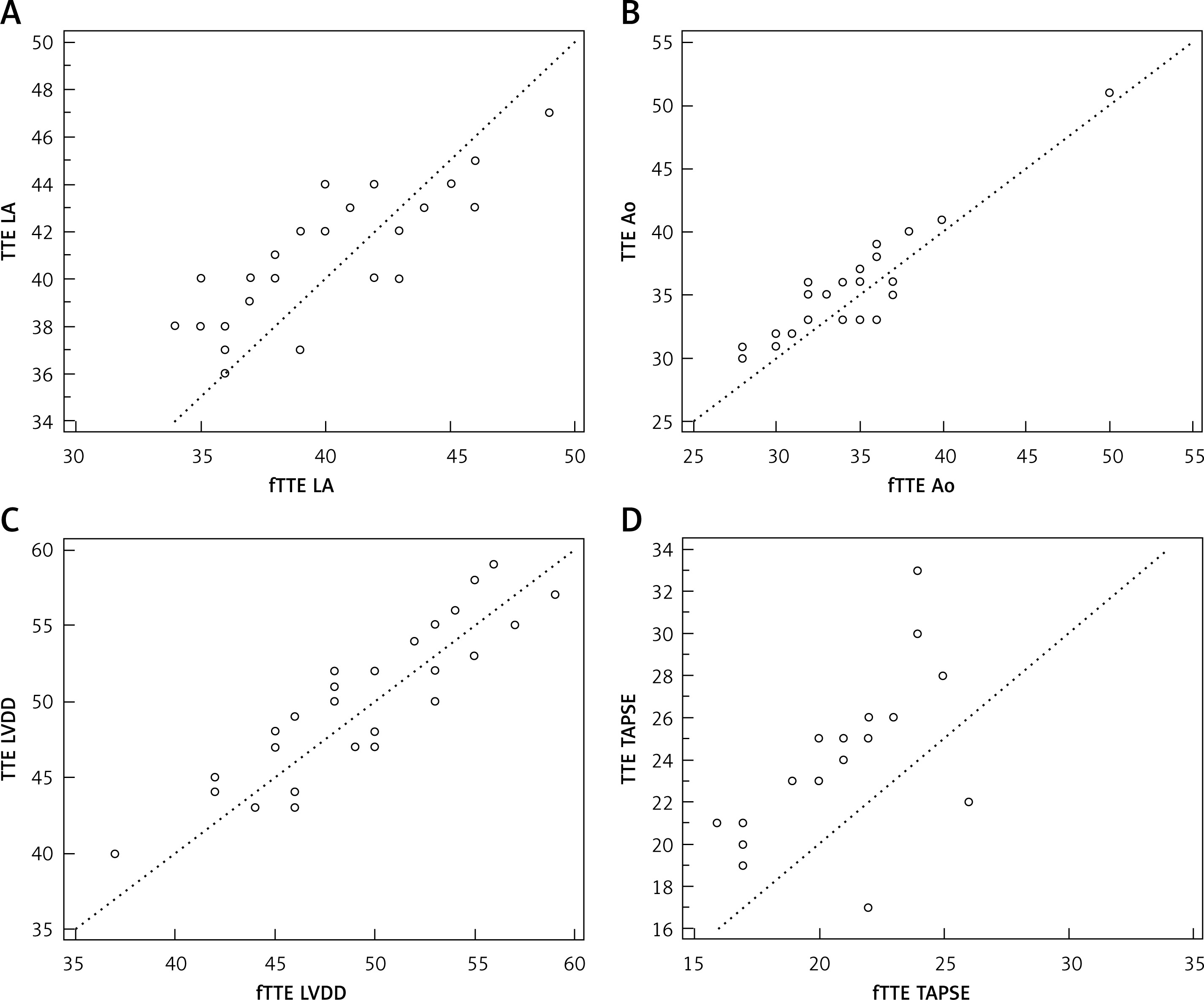
The dimensions of the left ventricle in diastole, the left atrium and the aorta obtained during the fTTE showed a good correlation with standard echocardiography (r = 0.89, r = 0.82 and r = 0.92 respectively, p < 0.001), but the correlation for TAPSE measurement was less pronounced (Table II, Figure 3). It should be noted that during the fTTE aortic dilatation up to 50 mm – aortic aneurysm – was detected in one asymptomatic patient with arterial hypertension.
Table II
Correlations between the measurements obtained by fTTE and TTE
Figure 3
Linear correlations for measurements obtained by focused echocardiographic examination (fTTE) and by standard transthoracic echocardiographic examination (TTE)
LA – left atrial dimension, Ao – ascending aorta diameter, LVDD – left ventricular diastolic dimension, TAPSE – tricuspid annular plane systolic excursion.
Wall motion abnormalities (WMA) were identified in 7 (23%) patients during fTTE and in 9 (30%) patients with the TTE. One patient had moderately reduced ejection fraction of the left ventricle (40%), 6 patients had mildly abnormal left ventricular ejection fraction (41–51%), whereas the remaining 23 patients had normal left ventricular ejection fraction (> 51%) [4]. The agreement for the evaluation of other cardiovascular findings, such as morphological and functional valvular abnormalities for fTTE and TTE, was also very good. Evaluation of valves was based on abnormal valve morphology and the presence of turbulent flow or regurgitation of the valve on the basis of a color Doppler. Table III presents the agreement of the results of echocardiographic examination regarding the evaluation of wall motion abnormalities and functional valvular abnormalities.
Table III
Agreement in qualitative echocardiographic assessment for fTTE and TTE
Discussion
Our study is the first to show that tele-echocardiography in real time by PSID (an ultrasound probe that can be plugged directly into a personal mobile device, such as a mobile telephone or tablet with a dedicated application) is feasible and may be clinically useful. It is an innovation among other pocket echocardiographs – an integrated tele-ultrasonic solution that allows for collaboration in real time by sharing devices’ camera, voice, and ultrasound examination. The study showed that operators who were not previously trained in the field of echocardiography – nurses, students, or doctors from departments other than cardiology after brief training – can perform a focused echocardiographic examination under the remote supervision of a cardiologist. None of the previous studies used a personal mobile device-based echocardiograph. Furthermore, echocardiographic images were collected by operators who were familiar at least with the basics of acquiring views.
Rouse et al. described the use tele-echocardiography which can provide quick diagnosis and prevent unnecessary patient transport, but in their study echocardiographic data could be sent only after the examination and the median time of the tele-echocardiogram request to the charted echo report was 18.6 h (range: 0.8–109 h) [5]. The PSID tested in our study allows real-time collaboration, which is an undoubted advantage. The cardiologist’s interpretation at the time of acquisition enables the clinician to quickly make a bedside diagnosis.
Previous studies over the past decade on the use of other PSID have shown that they enable the detection of serious abnormalities with an acceptable diagnostic value and can provide accurate responses to basic clinical problems [6–9]. Their use complements and improves the diagnostic efficiency of physical examination in the field of morphology and heart function [8]. With regard to measurements, it should be emphasized that our study confirms other reports based on other PSID, in which fTTE results show excellent correlation with standard TTE [10, 11].
In our study, measurements were taken only for LV, LA and Ao dimensions so as not to prolong the duration of fTTE. They showed good agreement with the TTE. This indicates that such measurements can be used and useful in some clinical situations requiring rapid bedside echocardiography. A good example is the detection of aortic aneurysm in an asymptomatic patient with arterial hypertension who has not had an echocardiographic diagnosis so far. However, greater difficulties were experienced with TAPSE.
It is known that a reliable assessment of heart morphology and function, including a visual assessment of global and regional left ventricular function, done within a few minutes with cardiologist consultation, can be a huge advantage, especially in patients with suspected cardiovascular disease [12]. Mjolstad et al. screened patients admitted to a medical department by performing short, pocket-sized ultrasound scans, which allowed correction of the initial diagnosis in 1 of 5 patients, resulting in a completely different treatment strategy without delay in many of the patients [1]. In our study, fTTE was performed by operators after only a short (1 h) training session on the use of the device and standard acoustic windows. The optimization of views acquired during fTTE was possible by communicating with the cardiologist and his feedback regarding the position and orientation of the ultrasound probe.
One of the main limitations of the PSID is the lack of a pulsed wave Doppler mode, which prevents an in-depth analysis of intracardiac flows. However, the combination of color Doppler imaging and grayscale imaging, which allows one to assess the density, calcification and mobility of leaflets, provides good sensitivity in the event of a valvular disease.
This study was based on a small group of patients examined in one center. The fTTE images were collected by an inexperienced operator. It can be assumed that the test results would be different if the fTTE was performed by a more experienced specialist. However, the published articles show that briefly trained non-experts in the field of echocardiography, including medical students, can obtain an acceptable diagnostic value to detect basic structural and functional results [13].
In conclusion, PSID allows efficient tele-echocardiographic examination by an inexperienced operator under the real-time supervision of an experienced cardiologist. The introduction of this new technology can revolutionize access to this imaging technique.