Introduction
Graves’ disease (GD) is an autoimmune disorder characterized by diffuse follicular cell hyperplasia and excessive production of thyroid hormone [1]. Graves’ disease is treated with antithyroid drugs, radionuclide therapies, and surgery. The common surgical indications for GD include non-responsiveness to medical or radioablative therapies, a large goiter with compressive symptoms, and worsening of ophthalmopathy.
The frequency of palpable thyroid nodules is 5% in the population and 15% in patients with GD [2, 3]. Thyroid ultrasonography (USG) is the most reliable method for detecting thyroid nodules, and with the advances in imaging methods, it is being used more frequently in patients with GD. Nodular lesions may be found in GD with thyroid USG in the preoperative period. The potential malignancy risk of thyroid nodules and the predictive factors for the development of incidental thyroid cancer in GD remain unknown. In previous studies, the incidence of papillary thyroid carcinoma (PTC) in patients with GD has been reported to be in the range of 2–17% [4–11]. Recently, Boutzios et al. and Wei et al. reported incidences of 33.7% and 32% of PTC in patients with GD respectively [12, 13]. Even though this issue is still controversial, these studies and other earlier studies suggest an increased risk of thyroid cancer in patients with GD, with the vast majority being incidentally detected micropapillary thyroid cancers. Also, Pellegriti et al. showed that the clinical course of thyroid cancer is more aggressive in patients with GD than in euthyroid control subjects [3]. The mechanisms responsible for the increased thyroid cancer incidence in patients with GD have not been clearly established yet. It is thought that thyroid stimulating antibodies may be responsible for this increase [14, 15].
The aim of this study was to evaluate the prevalence of thyroid nodules and thyroid cancer (TC) in patients who were surgically treated for GD. Another aim of the study was to determine the incidence of incidental thyroid cancer and its clinical course in these patients.
Material and methods
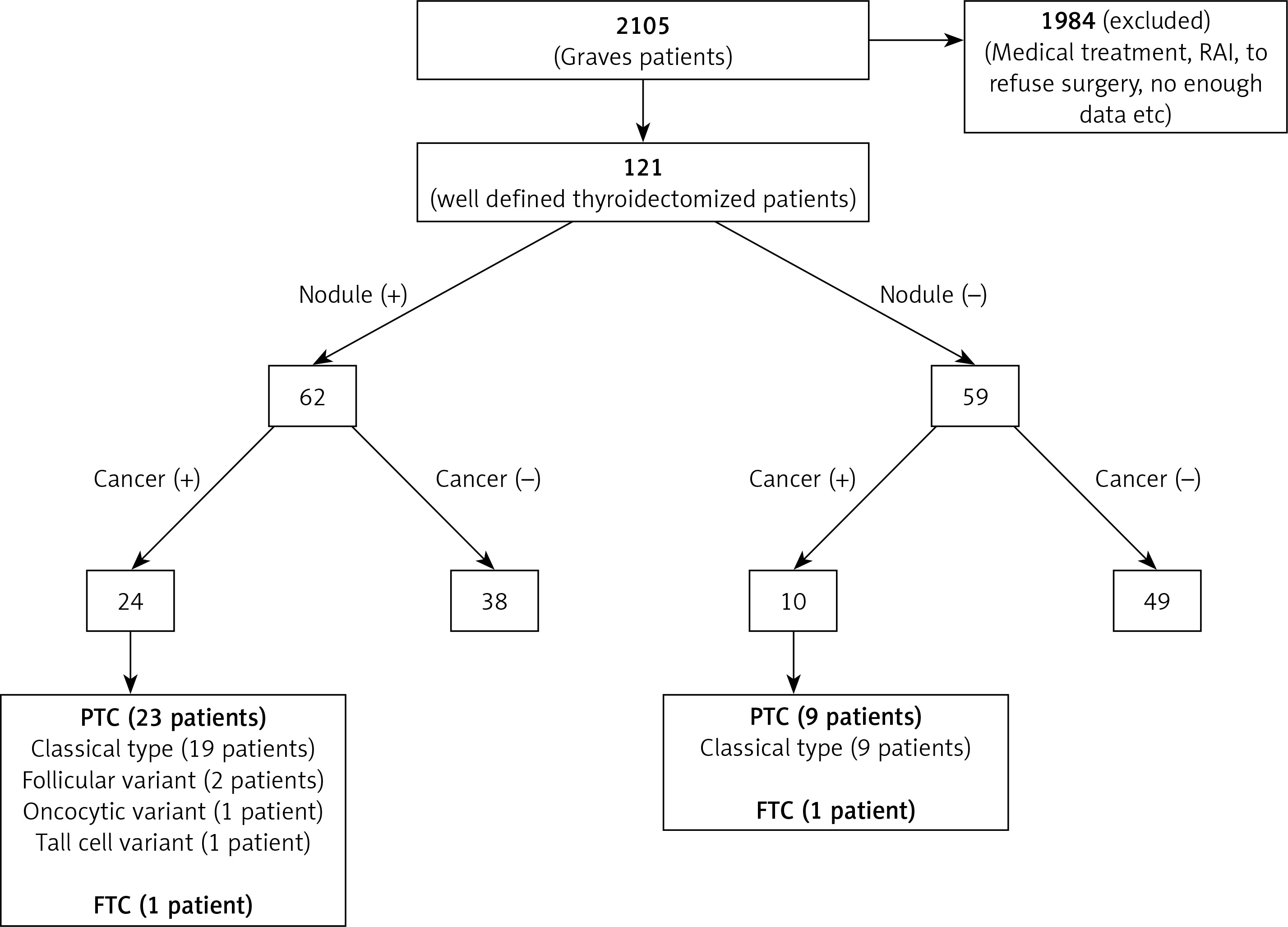
This is a retrospective, population-based study. The GD database of the Department of Endocrinology and Metabolic Diseases at Ankara University, Faculty of Medicine was used to identify patients who were operated on for GD. Out of 2105 patients with a diagnosis of GD, 121 patients who had a history of total thyroidectomy with or without central lymph node (LN) dissection during 2005–2015 were retrieved for this analysis (Figure 1). Demographic data, laboratory values, preoperative thyroid USG findings, thyroid autoantibodies, fine-needle aspiration cytology (FNAC) and postoperative pathology results were collected retrospectively.
The diagnosis of GD was made with typical symptoms and laboratory findings that included increased serum triiodothyronine (T3) and thyroxine (T4) levels, decreased thyroid stimulating hormone (TSH) levels, and diffuse uptake on thyroid scintigraphy. In most cases, the diagnosis was supported with increased thyroid stimulating antibody (TRAb) levels. None of the patients had previously received external irradiation to the neck, a family history of thyroid cancer, or an autoimmune thyroid disease.
The main indications for GD surgery included failure of antithyroid drug treatment or development of side effects with these drugs (n = 65, 53%), severe ophthalmopathy (n = 39, 32.3%), suspicion of malignancy on FNAC (n = 13, 10.7%), or a goiter that caused compression symptoms in the trachea or esophagus (n = 4, 3.3%).
All patients were examined using high-resolution B-mode grayscale USG (BUS), power Doppler USG (PD), and real-time ultrasound elastography (USE) (Hitachi EUB 7000 HV machine with 6–13-MHz linear transducer).
Statistical analysis
The frequency distribution of categorical variables between subgroups was compared by the χ2 test. Numerical variables were compared by the unpaired t-test. Statistically significant results obtained from univariate analysis were submitted to multivariate logistic regression. A p-value 0.05 was considered to be statistically significant. SPSS software version 22 (IBM) was used for statistical analysis.
Results
One hundred twenty-one patients were included in this study. Ninety patients (90/121, 74.4%) were female, and 31 were male (31/121, 25.6%). The median age at the time of diagnosis was 39 years (range: 17–79). Preoperative thyroid USG revealed a nodular goiter in 62 (51.2%) patients. No nodule was detected in the remaining 59 (48.8%) patients with GD. Median age at diagnosis was significantly higher in patients with nodules compared to those without a nodule (45 (19–79) vs. 34 (17–67; p < 0.001)). Other parameters (gender, TSH, fT3, fT4, autoantibody titers) did not differ between the two groups (Table I). The percentage of nodules that measured less than 1 cm and larger than 1 cm was 14.5% and 85.5% respectively.
Table I
Clinicopathological characteristics of patients
Thyroid cancer was identified in postoperative pathology specimens of 34 (28.1%) patients. The frequency of thyroid cancer was significantly higher in patients with nodules compared to patients without a nodule (38% vs. 16%; p = 0.009). Patients with thyroid cancer were older than the patients without thyroid cancer (45 (19–79) vs. 37 (17–69); p = 0.029). There was not a statistically significant difference in thyroid cancer incidence in male gender compared with female gender (5/31, 16% vs. 29/90, 32%; p = 0.086). Thyroid stimulating hormone receptor antibody and thyroid peroxidase antibody (anti-TPO) titers were significantly lower in patients with thyroid cancer (Table II).
Table II
Comparison of patients with and without thyroid cancer
By multivariate analysis, the presence of nodules (OR = 3.00, 95% CI: 1.25–7.2) and lower TRab serum levels were independent predictors of thyroid cancer in surgically treated patients with GD (OR = 1.01, 95% CI: 1.0–1.02) (Table III). All TC patients had differentiated TC. Of the 34 cancer patients, 32 had papillary thyroid cancer (PTC) and 2 had follicular thyroid cancer (FTC). In 21 of 34 differentiated thyroid cancer (DTC) patients (61%), tumor size was less than 10 mm in diameter (microcarcinoma). Of the 32 PTC cases, 28 were classical type, 2 were the follicular variant, 1 was the oncocytic variant and 1 was tall cell variant PTC (Table IV). Lymph node involvement was present in 3 (9%) of 34 patients with TC. There were 5 cases with extrathyroidal extension (15%), 2 cases with lymphovascular invasion (6%), and 19 cases with capsular invasion (56%) (Table IV).
Table III
Multivariate analysis for the prediction of TC in surgically treated GD patients
| Variable | OR (95% CI) | P-value |
|---|---|---|
| To have a nodule | 3.00 (1.25–7.2) | 0.01 |
| Lower TRab level | 1.01 (1.00–1.02) | 0.04 |
Table IV
Clinicopathological characteristics of thyroid cancer patients
Thirteen (38%) DTC cases showed multiple tumor foci. TC was detected in 28% of all thyroidectomized patients, and of them 38% of patients with nodular goiter. The prevalence of incidental TC without nodules was 8% (10/121). Nine of them were PTC and 1 was FTC. Of the 24 thyroid cancer patients with a nodular goiter, 23 had PTC and 1 had FTC.
Discussion
In this study, TC was frequently detected (28% (34/121)) in thyroidectomized patients with GD, and a significant portion (8%; 10/121) was detected incidentally. Most of the cases were low-risk papillary thyroid microcarcinoma (9/10; 90%). There has been an increasing interest in the coexistence of thyroid cancer and GD in recent years. In many cases, thyroid cancer is detected incidentally in pathological examinations. It is controversial whether this is an actual increase or a consequence of selection bias. We found that the incidence of thyroid cancer in patients with GD was higher than previously reported incidences in earlier studies. In a review by Belfiore et al., the rate of thyroid cancer in GD patients with palpable thyroid nodules varied from 2% to 46% [16]. Gabriele et al. reported that among 425 patients who underwent thyroidectomy for hyperthyroidism, only 7 had thyroid cancer. In the same study, thyroid cancer was not detected in any of the 64 patients with GD [14]. Our results are similar to rates reported by Boutzios et al. and Wei et al., which were 33.7% and 32% respectively, but higher than the rates reported by Ren et al. (13.7%) and Tam et al. (8%) [17, 18]. Wei et al. also reported a 69% rate of thyroid cancer in patients with nodular GD. In a meta-analysis of frequency of thyroid cancer in GD by Staniforth et al., patients with nodular GD were found to be approximately 5 times more likely to be diagnosed with thyroid carcinoma than those without nodules [19]. In accordance with these studies, our results showed that presence of nodule was an independent predictor for thyroid cancer in thyroidectomized patients with GD. The nodular GD group had more local invasive features than the nodule-free group in terms of multifocality, lymph node metastasis, and lymphovascular invasion.
The frequency of incidental thyroid cancer among all thyroid cancer cases was 29% in our study. Similarly, this frequency was found to be 20% in the study conducted by Ren et al. Erbil et al. found a 67% incidence of incidental thyroid cancer in GD patients who were diagnosed with thyroid cancer [20]. Although these results may indicate that the risk of developing thyroid cancer is high, it should be noted that selection bias may also cause this condition. Further randomized control studies are needed to make clearer comments on this issue.
Due to our analysis, frequency of nodule and thyroid cancer risk may increase with age in GD. These results are consistent with the literature. There are studies in the literature showing that thyroid cancers diagnosed at a younger age are more aggressive, but we did not find such a result in our study.
In our study, there was no significant difference in thyroid cancer incidence in male gender compared with female gender (5/31, 16% vs. 29/90, 32%; p = 0.086). This study was conducted only for patients with GD and therefore the number of women in the study group was significantly higher than the number of men.
Patients with papillary microcarcinoma nearly always have a good clinical outcome and no metastatic disease. Micrometastasis to lymph nodes rarely occurs and needs further investigations [11, 21]. In our study, the majority of cases were micropapillary thyroid cancer which did not have a lymph node metastasis or extrathyroidal invasion. Two previous studies performed with a euthyroid control group did not follow a worse clinical course in patients with DTC and GD [7, 22]. In contrast to these studies, in a study conducted by Pellegriti et al. over a 14-year median follow-up, patients with non-occult differentiated thyroid cancer and GD were shown to have a higher disease-specific mortality rate than the euthyroid control group [3]. Ren et al. identified 12 patients with incidental thyroid carcinomas from 347 patients with GD (4%) and detected distant metastases in two of them.
Furthermore, it is uncertain how an approach will be implemented in the treatment of microcarcinoma. It is known that microcarcinomas have a good clinical course. Some authors argue that advanced examination and treatment protocols for these clinically insignificant incidental lesions are not cost effective.
Another issue is whether to choose more aggressive treatment approaches in patients with nodular GD. According to some authors, early thyroidectomy is the most appropriate choice for these patients [10]. In fact, total thyroidectomy is considered the most effective and definitive treatment, even in patients with non-nodular GD. Nevertheless, total thyroidectomy carries some risks including permanent hypoparathyroidism and vocal cord dysfunction. Also surgeons can experience difficulties during surgery, especially due to the increased vascularity and chronic inflammation in the thyroid tissue of GD. Therefore, surgical treatment still remains a less preferred method than medical and radioactive iodine treatments in GD. Complications of surgery are rarely encountered when thyroidectomy is performed by experienced surgeons in tertiary care centers [23].
These results suggest that thyroidectomy, if performed by experienced surgeons, would be a suitable approach in patients with nodular GD. In patients without nodules, it may be more appropriate to decide according to conventional surgical indications to avoid over-treatment. Because of the increased frequency of incidental thyroid cancer in GD, surgery would be a good alternative in selected patients.
The causal relationship between GD and thyroid cancer has not been clearly elucidated. It is known that thyroid cancers seen in GD patients follow a worse clinical course than thyroid cancers seen in euthyroid patients [3, 24]. Belfiore et al. and Pellegriti et al. previously reported that thyroid carcinomas associated with GD are more aggressive than those in euthyroid patients and patients with non-autoimmune hyperthyroidism [24, 25]. However, there is a limited number of studies that examine the effects of TRab titers on the development of thyroid cancer in patients with GD. Ergin et al. found no significant association between thyroid stimulating immunoglobulin (TSI) titers and DTC development in a study with 248 surgically treated GD patients [26]. In contrast to the earlier literature, a lower TRab level was an independent predictor of thyroid cancer in our study. This was also the most remarkable result of our study, because in previous studies it was hypothesized that the level of TRab titers was responsible for the increased incidence of thyroid cancer in patients with GD. We believe that the different binding pattern of TRab to TSH receptors and heterogeneous biological effects on thyroid follicles may be responsible for this surprising result. Perhaps, antibody-mediated thyroid stimulation may be less effective for cancer development than TSH-mediated stimulation. Due to the fact that TSH suppression is more pronounced in patients with high antibody titers, the angiogenic effect on thyroid may be smaller. Furthermore, there may be other factors besides TRAB that are responsible for the development of cancer in patients with GD, such as anti-TPO and anti-TG titers, and environmental and genetic factors.
One important point to emphasize is that we investigated the risk of developing thyroid cancer in patients who underwent thyroidectomy for GD. It is not possible to generalize these results to all patients with GD.
Boutzios et al. found that 11 of 61 patients with GD and PTC had tall cell variant PTC (18%) [12]. Unlike this study, we detected only 1 tall cell variant PTC in 34 PTC patients.
In conclusion, our findings are concordant with previous studies and suggest that careful evaluation of all thyroid nodules in GD patients is essential. It seems reasonable to check GD patients for the development of possible incidental TC, even if they are nodule free. This is because we found a higher DTC incidence in operated GD patients without nodules.
Limitations of this study include the fact that this study is a retrospective analysis and nodule characteristics are not clearly known in USG performed in the preoperative period.