
Bullous pemphigoid (BP) is the most prevalent autoimmune blistering skin disorder, distinguished by a complex etiopathogenesis and a diverse clinical presentation [1]. Clinical professionals must acknowledge the extensive spectrum of clinical manifestations associated with BP and effectively tailor the diagnostic and therapeutic approaches to meet the individual needs of affected patients.
A 78-year-old female patient presented to the Clinic of Dermatology due to blistering lesions located on the right lower limb. According to the patient, the lesions first appeared over 6 months ago and were accompanied by severe itching. Notably, the patient had a history of right knee joint arthroplasty a year before. On admission, there were disseminated erosions and serous fluid-filled blisters present solely on the skin of the right knee and the right shin, with no involvement of mucous membranes (Figures 1 A, B). Following a physical examination, a thorough diagnostic evaluation was performed. Histopathological examination of a biopsy obtained from lesional skin revealed a subepidermal blister with an intact epidermal roof without signs of necrosis; the blister content included fibrin and isolated inflammatory cells. In the upper dermis, a diffuse inflammatory infiltrate with individual eosinophils was observed (Figures 1 C, D). Direct immunofluorescence (DIF) of perilesional skin using a short-arc mercury lamp-operated microscope (BX40, Olympus, Japan) was used to assess the intensity of deposits on the slides, which were graded using a semiquantitative 4-point scale (from “-” to “+++”) at the original objective magnification of ×40. The imaging revealed linear deposits of IgG4 (+++) (Figure 2) and C3 (++) along the dermo-epidermal junction. A six-parameter ELISA (Euroimmun, Lübeck, Germany) test showed a positive IgG antibody titre against BP180 (2.51 with a cut-off value 1.00). Considering the patient’s history of lower limb orthopaedic surgery and the immunopathological findings, a diagnosis of localized, trauma-induced bullous pemphigoid was established. During hospitalization, the patient was treated with intravenous methylprednisolone at a cumulative dose of 1250 mg and doxycycline 100 mg twice daily. In addition, oral nicotinic acid (vitamin PP) was administered. Discharge recommendations comprised oral treatment, specifically doxycycline 100 mg twice daily, methylprednisolone 24 mg daily with gradual tapering to 4 mg, and continued supplementation with vitamin PP, as well as topical treatment with clobetasol propionate ointment applied twice daily for 14 days, then once daily.
Figure 1
Clinical and histopathological features of a patient with localized surgery-induced bullous pemphigoid. The scar after knee surgery (A) and disseminated erosions and serous fluid-filled blisters on the skin of the right shin (B) were seen. Histopathological H + E staining revealed a subepidermal blister with an intact epidermal roof without signs of necrosis; the blister content included fibrin and isolated inflammatory cells (original magnification ×200) (C). A diffuse inflammatory infiltrate with individual eosinophils was observed in the upper dermis (original magnification ×400) (D)
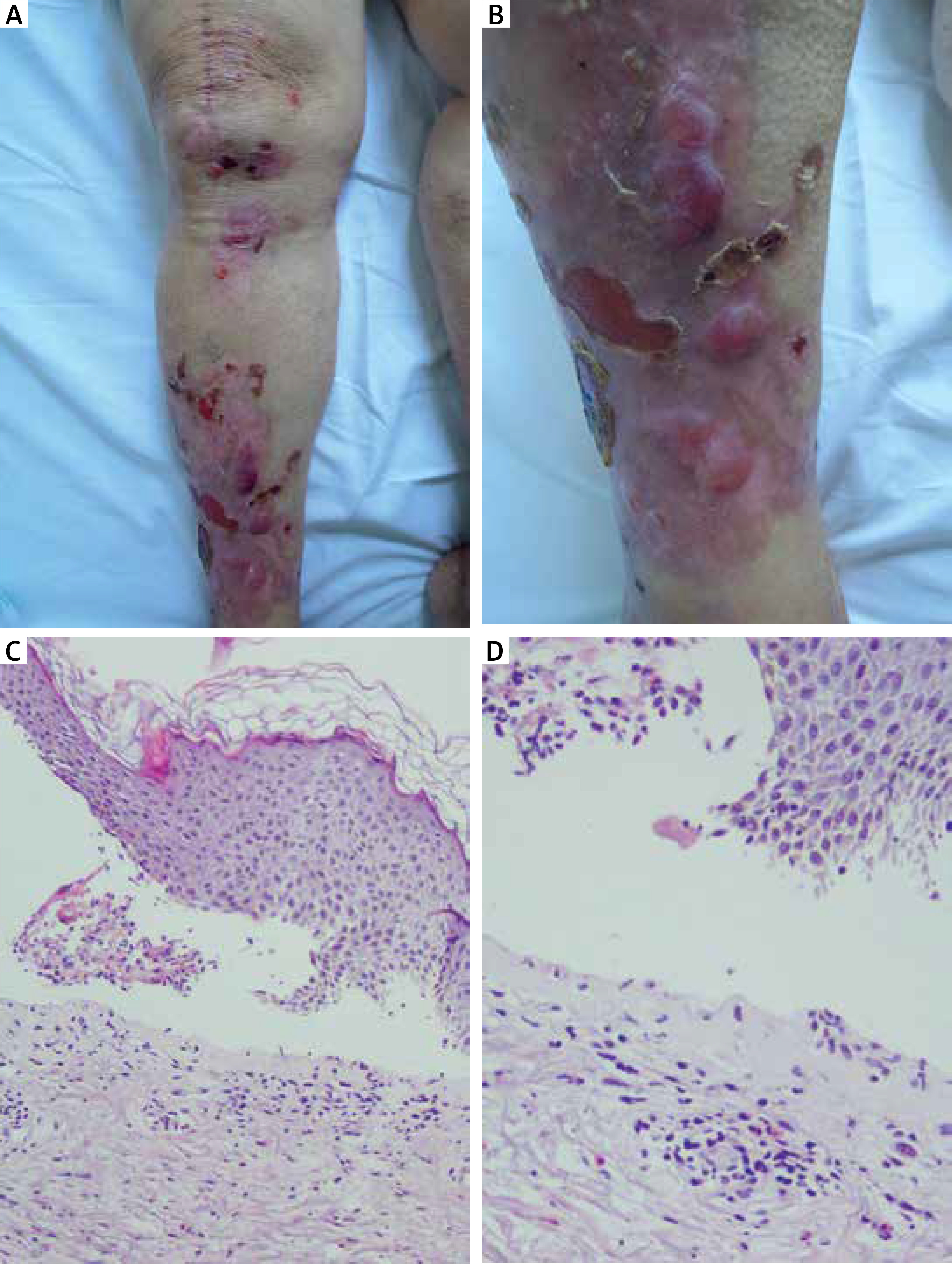
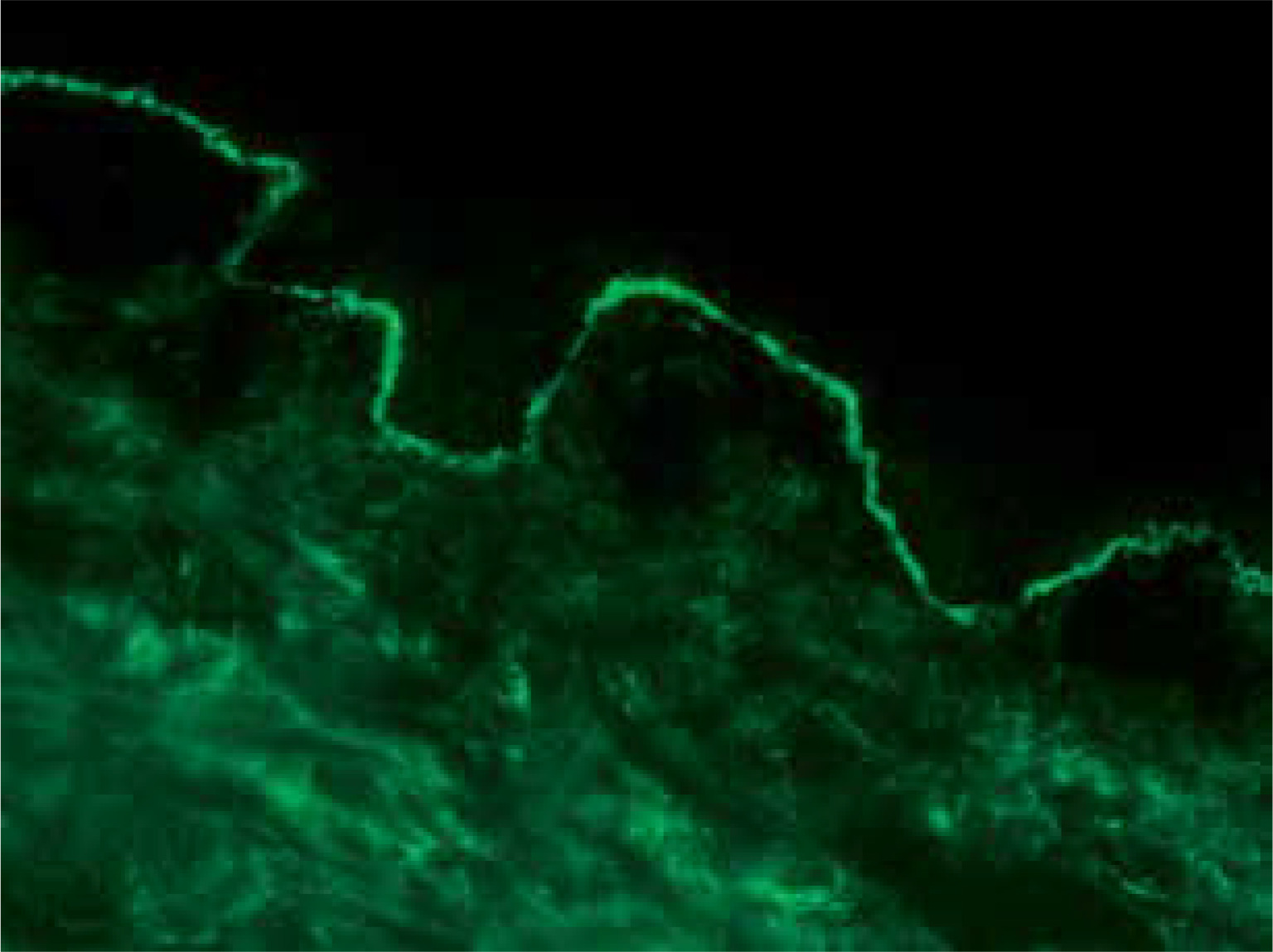
Figure 2
Linear deposits of IgG4 (+++) along the dermo-epidermal junction visible in direct immunofluorescence (DIF) of perilesional skin (original objective magnification ×40)
BP exhibits a broad clinical spectrum and may be triggered by various external factors, including surgical trauma. The pathomechanism of trauma-induced BP remains incompletely understood. It is hypothesized that tissue injury initiates an inflammatory cascade, leading to autoreactivity against basement membrane components, particularly BP180 [2]. Isomorphic phenomenon (Köbner phenomenon) or similar cutaneous reactions are plausible in this clinical setting [3]. Alternatively, trauma may directly alter the structure of basement membrane proteins, thereby increasing their affinity for specific human leukocyte antigen (HLA) alleles [4]. Localized oedema, a common consequence of orthopaedic surgeries, likely triggers the pathogenesis of localized BP [5]. Notably, over 7% of individuals may have circulating BP180 and/or BP230 antibodies without any clinical manifestations of BP and with negative results of indirect immunofluorescence; however, these autoantibodies dose-dependently activate neutrophils in vitro [6, 7]. The oedema and vascular congestion resulting from the orthopaedic surgeries increased the local concentration of BP180 and BP230 antibodies, inflammatory mediators, and immune cells, ultimately leading to the localized formation of blisters [5]. Currently, no epidemiological studies evaluate surgery-induced BP, and the available data are derived solely from case reports. An analysis of reported cases revealed that out of 147 instances of pemphigoid diseases triggered by physical factors, 22 were induced by surgery [8]. The clinical-laboratory features of surgery-induced cases of localized pemphigoid diseases are presented in Table 1 [9–22]. In this context, the term “pemphigoid diseases” was used as the term “bullous pemphigoid, acronym BP” should be reserved only for patients in whom IgG antibodies to BP180 and/or BP230 were identified. The timing of onset can vary significantly, and several patterns emerge from case reports. Immediate-onset BP occurs within the first days or weeks after surgery and is likely a result of the aforementioned Köbner phenomenon. Interestingly, there are several cases of localized BP developing several months to even years after surgery. Such cases may arise from chronic subclinical inflammation or structural alterations at the dermal-epidermal junction following skin trauma, which predispose the affected area to subsequent immune-mediated attacks. In our patient, the lesions appeared 1 year after the knee joint arthroplasty. When suspecting autoimmune bullous dermatoses, DIF and molecular-biochemical serum studies to identify protein epitopes targeted by the autoimmune response represent the minimal and sufficient laboratory diagnostic examinations [1].
Table 1
Summary of cases of localized pemphigoid diseases caused by surgical trauma
| Sex | Age | Surgery type | Disease localization | Time from surgery to lesion appearance | Diagnosis | Treatment | Reference |
|---|---|---|---|---|---|---|---|
| Female | 79 | Abdominal surgery | Abdomen | UA | DIF and histology (detailed results UA) | UA | [9] |
| Female | 85 | Total knee arthroplasty | Right leg | 2 days | DIF linear deposits of IgG and C3 along basement membrane; ELISA: anti-BP180 negative, anti-BP230 negative | Topical betamethasone and fusidic acid, followed by clobetasol propionate, nystatin and oxytetracycline cream; emollients and non-silicone, non-adhesive dressings | [10] |
| Female | 72 | Prosthetic graft placement in the left forearm | Skin over the graft subsequently spreading to the ventral side of the right arm and the medial side of both thighs | 3 days | DIF linear deposits of IgG and C3 along basement membrane; Immunoperoxidase staining showed type IV collagen at the bulla base | Graft removal, systemic treatment with prednisone, tetracycline, and niacinamide | [11] |
| Female | 79 | Hemiarthroplasty for humerus fracture | Left shoulder | 1 year | DIF linear band-like deposition of IgG andC3 along the roof of the split; biopsy of a vesicle showed mild irregular acanthosis, a subepidermal blister, and an infiltrate of eosinophils, lymphoid cells and histiocytes | Topical corticosteroids | [12] |
| Male | 66 | Coronary artery bypass grafting | Chest and saphenous vein harvest site on the lower right leg | 2 weeks | DIF depositions of IgM and C3 on the hemidesmosomal region of the basal cells and C3 along the dermal side of salt-split skin; IIF titre > 1/20 | Systemic tetracycline and clobetasol propionate cream | [12] |
| Male | 73 | Insertion of a left brachio-basilic fistula and a right permanent infra-clavicular central venous line | Right neck side and left arm | 2 weeks | DIF linear deposits of IgG and C3 along dermo-epidermal junction; IIF titre 1 : 160; Immunoperoxidase staining showed type IV collagen at the blister base | Topical clobetasol propionate and systemic flucloxacillin | [13] |
| Male | 76 | Abdominal hernia surgery | Generalized | 2 months | DIF and skin biopsy | Prednisone 60 mg/day | [14] |
| Female | 39 | Bilateral leg surgery after traffic accident | Surgical scars on the legs | 15 years | DIF linear complement C3 deposition at the epidermal basement membrane | Topical clobetasol propionate | [15] |
| Female | 65 | Arthropro-thesis for coxarthrosis | Generalized | UA | DIF linear deposits of IgG and C3 at basement membrane zone; anti-BP180 positive, anti-BP230 negative | Azathioprine (100 mg/day) and betamethasone (15 mg/day) | [16] |
| Female | 61 | Right femur fracture surgery | Surgical scar, followed by generalized lesions | 1 month | DIF clear band of IgG-deposition at the dermo-epidermal junction; IIF titre 1 : 20; anti-BP180 positive | Methylprednisolone (1 mg/kg daily) | [17] |
| Male | 80 | Abdominal surgery | Incision sites on the abdomen | UA | DIF and skin biopsy | UA | [18] |
| Female | 73 | Laparoscopic cholecystectomy | Periumbilical area around the scar | 7 days | DIF linear deposits of IgG and C3 | Topical clobetasol propionate | [19] |
| Female | 78 | Pacemaker insertion | Cleavage skin around the scar | 5 days | DIF linear deposits of IgG and C3 | Topical clobetasol propionate | [19] |
| Female | 76 | Bilateral forefoot surgery | Both forefeet | 2 weeks | DIF and skin biopsy | Prednisolone 60 mg/day | [20] |
| Male | 62 | Coronary artery bypass surgery | Left shin at the site of vein graft harvesting | Soon after surgery (exact number of days UA) | DIF linear deposits of IgG along the roof and C3 complement on the roof and floor of the blister | Prednisolone 40 mg/day | [21] |
| Female | 57 | Right total knee replacement | The surgical scar and surrounding skin on the right anterior knee | 3 months | DIF linear IgG and C3 deposition at the dermal-epidermal junction, skin biopsy | Betamethasone dipropionate 0.05% ointment twice daily | [22] |







