
The right to gender identity is one that amounts to contouring an individual’s personality. The present hour calls for an understanding of the meaning that the term transgender holds. It needs to be recognized that sex and gender although often used interchangeably are quite distinct. Sex refers to the physical characteristics (e.g. reproductive organs, chromosomes, hormones) employed to assign people to be female, male, or intersex. However, gender is more of a social construct, sprouting from cultural expectations that shape an individual’s external appearance and conduct [1]. Gender identity disorders have been frowned upon throughout their existence, making their treatment quite controversial. Gender dysphoria, earlier known as gender identity disorder, describes a heterogeneous group of individuals having the desire to possess secondary sexual characteristics of the opposite sex and possessing varying degrees of dissatisfaction regarding their anatomical gender [2]. Gender reassignment surgery (GRS) has proven to be a revolutionary intervention for patients with gender dysphoria, hence playing a pivotal role in alleviating their psychological discomfort. GRS is a multidisciplinary endeavour requiring a collaborative effort of psychology, psychiatry, family medicine, plastic surgery, endocrinology, otolaryngology, urology, gynaecology, maxillofacial surgery, and, last but not least, anaesthesiology.
Though GRS is becoming popular and more acceptable, there is still a relative lack of awareness of the process and its associated challenges amongst healthcare professionals. GRS has been performed with various approaches, single and multiple settings, hence imposing the need for anaesthetists to search for better and more efficient modes of anaesthesia to improve prognosis and minimize the associated morbidity. Just as surgeons develop areas of specialization to better care for their patients, anaesthesiologists have specialized in out- and inpatient surgery, both cosmetic and reconstructive.
The vanishing stigma, increasing demographic and acceptance of transgender and gender non-binary (TGNB) individuals calls for the field of medicine to catch up too. Hence, it is only discerning to expect that in coming times, they will present more frequently in general surgical settings and as they do, we would be well prepared to provide them high-quality peri-operative care. The ardent need to review this topic is rooted in the acknowledgement that although there are articles discussing the surgical and peri-operative outlooks of this procedure, there is scarce literature about the role, considerations, and strategies for anaesthesia in these procedures. This substantial shortfall in the published literature regarding the holistic concerns of GRS demands further strategies to be explored. We have discussed the anaesthetist strategy governed by consideration of the psychological aspects, effects of hormone therapy, optimal modes for anaesthesia and cautious watch for complications along with timely intervention for handling the same for providing high-quality anaesthetic care. In this article, we aim to analyse, understand, and formulate an approach for the entire procedure from an anaesthesiologist’s perspective.
RESEARCH METHODS
For this review, we retrieved data by a systematic literature search carried out in the research databases including PubMed, EMBASE, and Google Scholar. We included review articles, original studies, and case reports in our search.
History and current scenario
Dr Alan L. Hart, a TB specialist in the US, became one of the first female-to-male transgender persons who underwent gonadectomy and hysterectomy for his gender dysphoria in 1917 [3]. According to the 2018 census, nearly 0.6% of adults in the United States, or 1.5 million individuals, make up the transgender community. The estimated transgender population worldwide in the 2018 census ranged between 1% and 2% of the total population, which is nearly 900 million people. The American Society for Plastic Surgeons (ASPS) has reported an expeditious rise in GRS of up to 155% within the span of 2016 to 2017 [4]. With the legalization of transgender in most of the countries throughout the globe, the curve of GRS surgery is probably going to run further upslope.
OVERVIEW OF THE PROCEDURE
As already described, GRS requires a multidisciplinary approach. To begin with, the guidelines for the Recommendation of GRS indicate that the patient should be physically and psychologically prepared for surgery and should have a clear perception of the interventions to be performed along with the risks and possible complications [5]. Preparation for GRS is a multistage process that includes an elaborate psychological and wellbeing assessment of the patient. This may take nearly 12 months for complete psychosocial preparation of the patient to deal with the transition. Psychological evaluation is then followed by feminizing or masculinizing hormone replacement therapy (HRT) prescribed by a consulting endocrinologist. There should be documented “real-life experience in the desired role” for at least a whole year [5]. GRS ensues at the end of this process. The algorithm for the entire procedure is summarized in Figure 1.
INITIAL EVALUATION
What is required is having an elaborate understanding and assessment of the patient’s psychological, medical, legal, and social concerns. In developing countries, a substantial proportion of this relates to social and psychological aspects. The mental wellbeing assessment aims at evaluating and treating the mental health issues, offering suggestions with peer support with or without family therapy, assessing the gender expression level and the readiness of the patient for fully or partially reversible and irreversible interventions [6]. A reassuring and sensitive attitude towards the patient affirming that they would receive the best available care without any judgment aids in alleviating their anxiety and concerns. A holistic approach to assessment involves the multidisciplinary effort of various medical teams.
ANAESTHETIC PLAN OF CARE
Pre-operative assessment
Apart from the routine preoperative assessment as for any other surgery, here we need to address specific history, examination, and investigations. The aim should be at the optimization of the patient care through risk reduction and informed consent [7]. It also caters to efficiently preparing the patient for surgery and anaesthesia while encouraging their compliance and participation.
General assessment
The biological sex and current gender identity of the patient should be noted.
In the absence of specific gender assignment, measurements and calculations with gender specificity become tricky, e.g. ideal body weight, target-controlled propofol infusion using Schneider mode [8].
Medical concerns.
Patient’s preferred form of address (i.e., title, name, pronouns).
Assessment of co-morbidities
History of use of anti-depressants, anti-anxiety, and other psychotropic drugs should be derived.
Higher risk of tobacco, substance abuse, and sexually transmitted diseases (STDs) should be taken into consideration [9]. The prevalence of HIV was found to be 8.2% in the Indian transgender community as compared to 0.31% national HIV prevalence in India [10].
History of multiple silicone injections can cue towards the existence of granulomatous disease, pneumonitis, organ failure, and infection [11, 12].
History of hormone replacement therapy
Clinical examination
Should be done with due respect to the privacy and dignity of the patient while maintaining professionalism.
A chaperone of the gender of the patient’s choice should be present during physical examination.
Should include assessment of any restrictive lung disease (common in female-to-male [FTM] chronic chest binders) [8].
Laboratory evaluation and investigations
Most of the parameters should be evaluated as per the patient’s biological sex.
However, for patients who have received HRT for more than six months, it has been suggested to compare the laboratory values to their cis-counterparts rather than their biological sex [13].
There is still limited evidence regarding interpretations in different stages of gender transition.
A pregnancy test should be mandatorily taken for FTM transgender in childbearing age as per the American Society of Anesthesiologists (ASA) recom-mendation [14].
Investigations to evaluate effects of HRT:
Counselling, consent, and pre-operative care
Recognition and management of depression, anxiety, and regret.
Advice on quitting smoking and explanation of its implications.
Discontinuation of HRT for nearly 2-4 weeks before surgery in consultation with the endocrinologist and surgeon, keeping in consideration that prolonged withdrawal of hormones may culminate in the reversal of desirable effects [17].
Considering the use of low-dose aspirin along HRT to reduce the risk of thromboembolism.
Patients should be well informed regarding the overall cost, duration of hospitalization, surgical and anaesthetic options, complications, and post-operative care, and consent should be obtained.
Anaesthetic implications and concerns of HRT
It is not only relevant but imperative for an anaes-thesiologist to be aware of the various effects of HRT as it can guide the formulation of an efficient plan for anaesthesia. The various medications given in feminizing hormonal therapy include gonadotropin-releasing hormone agonists such as leuprolide and goserelin, spironolactone (androgen blockers), oral, parenteral or transdermal oestrogens and 5-α-reductase inhibitors such as finasteride. These medications can pose a higher risk of endocrine (e.g., diabetes) and cardiovascular (e.g., hypertension, venous thromboembolism [VTE]) implications. Testosterone therapy has been associated with derangements in liver function, which in turn complicate the drug metabolism. These risks are higher in the patients receiving oral formulations, hence necessitating the discontinuation of HRT for a few weeks prior to the surgery [16]. However, the withdrawal of hormone therapy can potentially make these patients more emotional, with rapid mood swings. This in turn can pose certain challenges for the anaesthetist in patient handling in the perioperative window (Table 1). Incidence of postoperative delirium and post-operative nausea and vomiting (PONV) has also been found to be higher in patients on HRT. Some cases have revealed the occurrence of migraines in patients on anti-androgens. It is important to remember that in many cases these patients require lifelong administration of HRT unless curtailed by severe adverse effects.
TABLE 1
Anaesthetic implications and concerns of hormone replacement therapy
Intra-operative considerations
The intra-operative care of these patients is distinctive as it needs the discernment of special anatomical, psychological, physiological, and pharmacological issues as numerated in Figure 2. An anaesthesiologist needs to pay close attention to the following considerations:
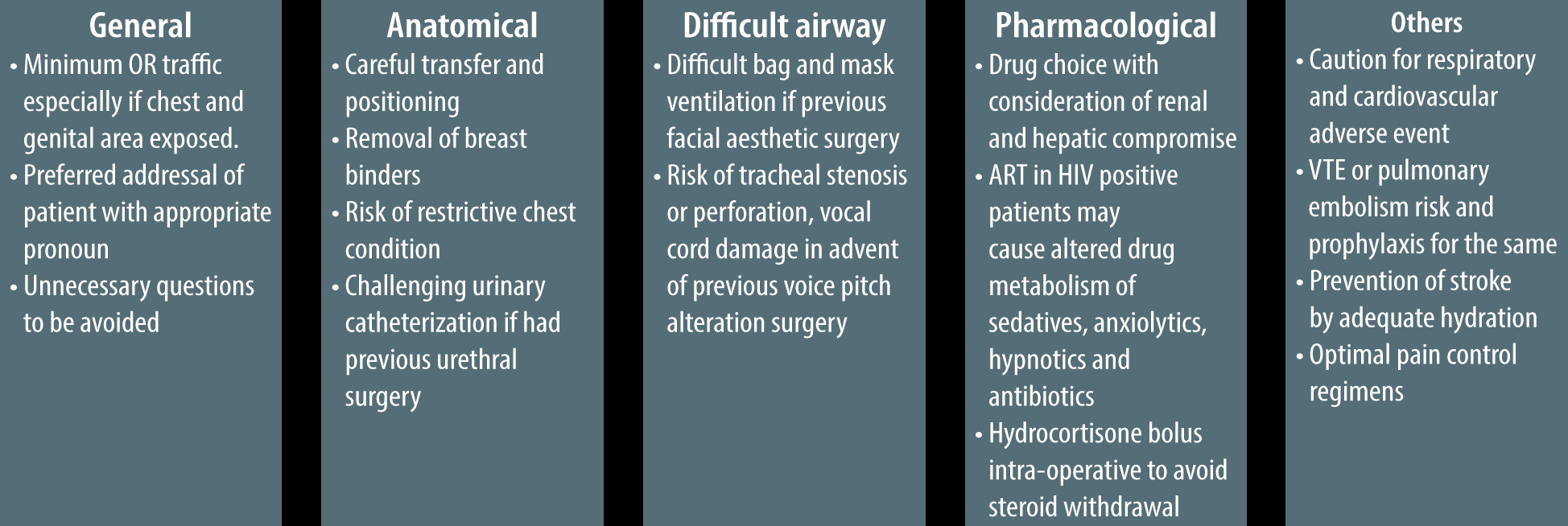
General
There should be clear instructions to the peri-operative team to maintain minimum traffic within the operating room (OR), particularly when the surgery involves exposure of the chest and/or genital regions.
The patient’s preferred pronouns should be known and used at all times by the peri-operative staff when addressing the patient and any unnecessary questions should be discouraged.
The choice of modes of anaesthesia should be made after a cautious evaluation of the procedure, patient’s expectation, and their best interests (Table 2).
Anatomical considerations
Transfer and positioning of the transgender patients who have undergone external body contouring procedures can be challenging and needs to be done with utmost caution.
FTM transgenders may be using chest wraps and breast binders that need to be removed beforehand. Though there is still insufficient literature on the topic, chronic use of these tight chest binders can pose the risk of a restrictive respiratory pattern [14].
Interestingly, even the most routine procedure of urinary catheterization can get tricky and challenging in the patients who have already had GRS concerning the urethra done, e.g. metoidioplasty with urethral lengthening, phalloplasty, or vaginoplasty.
Difficult airway
Patients who have recently had various facial aesthetic procedures such as rhinoplasty or jaw reconstruction may pose a challenge during bag and mask ventilation and should be handled with care and caution.
Patients who have had previous voice pitch altering surgery such as chondroplasty or laryngoplasty may present as a difficult airway scenario as they pose the risk of tracheal stenosis or perforation, vocal cord damage, and dysphagia. Hence, a difficult airway cart should be kept ready [22].
Pharmacological considerations
It needs to be taken into consideration that transgender women suffer from higher rates of HIV infection and might be on anti-retroviral therapy (ART). The various sedatives, anxiolytics, hypnotics, and antibiotics may present significant interactions with antiretroviral agents and result in altered drug metabolism [23].
As these patients have been off steroid therapy for few weeks, they might experience steroid withdrawal syndrome. This can be prevented by administering a steroid bolus of 100-200 mg hydrocortisone intra-operatively.
Other
An anaesthetist needs to be vigilant for elevated intraoperative risks due to the possible existing respiratory, renal, cardiovascular, and hepatic compromise of the patient.
VTE is a major perioperative concern due to the use of HRT medications and needs to be looked out for and relevant preventive interventions should be adopted. Cautious haemodynamic monitoring needs to be done for the early identification and management of this dreaded complication. Intraoperative prophylaxis should be provided with subcutaneous heparin and graded compression devices.
Higher incidence of stroke has been linked to greater erythropoietin production and haematocrit and hence increased blood viscosity, attributed to parenteral testosterone therapy. Therefore, adequate hydration should be maintained for the patient [24].
Considering the extensive nature of surgery, efficient pain control is imperative.
TABLE 2
Modes of anaesthesia
COMPLICATIONS
GRS presents with its arena of complications to be looked out for and dealt with. Amongst them, certain complications demand the anaesthesiologist’s ardent attention (Table 3). These patients may be suffering from anaemia owing to the multiple and prolonged operations they undergo over some time. This needs to be taken care of by adopting appropriate pre-operative optimizing and perioperative blood loss reducing strategies. Two of the dreaded complications that the patients on oestrogen therapy should be monitored for are pulmonary embolism (PE) and deep vein thrombosis (DVT) [25]. These haematological events are attributed to peri-operative immobility, but due to the thrombotic effects of transgender HRT, there is a considerably higher risk of the same in these patients. The range of occurrence of VTE in transgender women on oestrogen therapy is from 0% to 6% [26]. The hypercoagulable state resulting due to HRT medications (both male-to-female and FTM) can precipitate cerebrovascular accidents and myocardial infarction and also aggravate any pre-existing coronary disease. This in turn warrants maintenance of adequate hydration at all times along with utmost care during all the phases of anaesthesia, supplemented by cautious intra-operative monitoring.
TABLE 3
Complications in gender reassignment surgery, associated risk factors and preventive measures
The extensive wound surface, adverse effects of steroid therapy, and repeated surgery make these patients more susceptible to various infections, necrotizing fasciitis, and septicaemia [27]. The various other surgical complications include gastrointestinal events (e.g., rectal injury and rectovaginal fistula) and urinary tract complications (e.g., urethral stricture, fistula, and incontinence). Some unspecific events such as inguinal hernia, compartment syndrome, and asymmetry can also be witnessed after the surgery.
POSTOPERATIVE CONSIDERATIONS
The challenges continue after the completion of surgery, as the post-operative period in these patients has its concerns of postoperative pain, anxiety, depression, withdrawal, and at times regret [28]. Amongst the other parts of a detailed handover to the post-operative care team, one of the most important is validation of the patient’s preferred pronoun and name to avoid any unnecessary and repeated questioning [8]. It should be ensured that there is a multi-pronged approach with optimal analgesic strategies to manage post-operative pain. This can include epidural anaesthesia, intravenous analgesics, peripheral nerve blocks, parenteral therapy, and patient-controlled analgesia (PCA). There should be a collaborative approach to tend to the patient’s mental health, as well as social and spiritual needs. Canner et al. [29] reported that transgender patients require a higher level of care, highlighting the significance of formal training of health care providers for best practices to encourage and achieve a respectful and holistic approach towards anaesthesia delivery. Early implementation of social work and community support in the postoperative period plays a major part to smoothen the process of discharge while assisting the transition to patient recovery.
IMPORTANCE OF TEAMWORK AND COLLABORATION
As already mentioned, the complex procedure of gender reassignment involves a multidisciplinary effort of psychology, psychiatry, family medicine, plastic surgery, endocrinology, otolaryngology, urology, gynaecology, maxillofacial surgery, and anaesthesia. Evaluation by mental health professionals for eligibility criteria is a precondition for GRS as it can be a physically, emotionally, financially, and socially overwhelming procedure. The plastic surgeons, otolaryngologists, urologists and all other contributing surgeons need to have clear and competent participation in this long-term therapy. The surgeon and endocrinologist should also collaborate in optimizing HRT withdrawal and restart in the peri-operative period. The current state of affairs is still lacking such a closed loop inter-disciplinary approach. Hence, an efficient and especially dedicated team can help in achieving the ultimate goal of quality management to harness favourable outcomes for the patient.
CONCLUSIONS
Various parts of the world still suffer through an under-representation of the transgender community which stays confined to the margins of society. However, there is no denying the fact that with the changing tide and rising acceptability of transgender persons, the field of medicine is going to be presented with an increased proportion of these patients. The specific emotional, physiological, and pharmacological concerns coupled with the collaborative interplay of multiple disciplines make this class of patients a challenging lot. It is the attitude, preparedness and prudence of the medical team that can bring about a favourable outcome. Proper training of various health care professionals appears imperative here to empathetically handle and efficiently treat these patients. We would not be wrong in believing that the quality care provided before, during and after surgery has a substantial impact on patient outcomes after GRS. This simultaneously deserves acknowledgement of the fact that extensive studies and evidence are needed to understand and define better strategies for perioperative care in patients presenting for GRS.