
INTRODUCTION
Pemphigus comprises a group of autoimmune vesiculobullous diseases affecting skin and mucous membranes, histologically characterized by intraepidermal blister formation due to acantholysis. This results from IgG autoantibodies targeting desmogleins, which are essential for keratinocyte cell–cell adhesion. In pemphigus vulgaris (PV), blistering occurs in the lower epidermis, just above the basal layer. PV is associated with IgG autoantibodies directed against desmoglein 3 and desmoglein 1 [1, 2].
The rare and infrequent variant of PV is pemphigus vegetans (Pveg). The epidemiology of Pveg has not been established yet. According to reports, it accounts for 1–2% of all pemphigus cases, and the global incidence of PV is around 0.7 per 100,000 individuals [3, 4]. Clinically, lesions are predominantly found in intertriginous areas, where flaccid blisters evolve into erosions, and subsequently develop into vegetating papules that coalesce into erythematous, moist, malodorous plaques, often with purulent discharge [5]. Oral involvement is also common.
Histopathological features include the suprabasal acantholysis with papillomatosis of the dermal papillae, downward proliferation of epidermal strands into the dermis, hyperkeratosis with scale-crust formation, and intraepidermal eosinophilic or neutrophilic abscesses.
The differential diagnosis includes conditions with similar clinical presentation, such as secondary syphilis, Hailey-Hailey disease, and lymphogranuloma venereum (LGV) [2].
OBJECTIVE
A case of Pveg in a 72-year-old male is presented, characterized by extensive erythematous verrucous lesions in the intertriginous genital area, scalp involvement, and oral mucosal lesions, accompanied by an intense malodorous discharge.
CASE REPORT
A 72-year-old male was admitted to the Department of Dermatology on an emergency basis due to extensive verrucous lesions in the groin, oral mucosa, and erythematous lesions on the scalp, clinically resembling condyloma lata.
In 2011, the patient had been diagnosed with linear IgA dermatosis. Histopathological examination at that time revealed epidermal hyperplasia with elongated rete ridges and eosinophilic microabscesses, findings suggestive of pemphigus vegetans (Pveg). Direct immunofluorescence (DIF) demonstrated linear deposition of IgA (+++), fibrinogen (+), and C3c (+) along the basement membrane zone. Systemic treatment with prednisone 40 mg/day was initiated. The patient continued prednisone therapy for 12 years, currently at a dose of 10 mg/day, prescribed by a general practitioner without dermatological follow-up.
On admission, extensive cauliflower-like vegetations and numerous erosions covered with fibrin and mucous exudate were observed in the intergluteal and perianal regions, including the glans penis. Erythematous and erosive lesions covered with crusts were present on the scalp. Oral examination revealed hyperkeratotic plaques on the tongue with a cerebriform appearance. The lesions were associated with an intense malodorous discharge.
The patient had a history of hypertension treated with perindopril and indapamide. He denied any drug allergies (figs. 1–3).

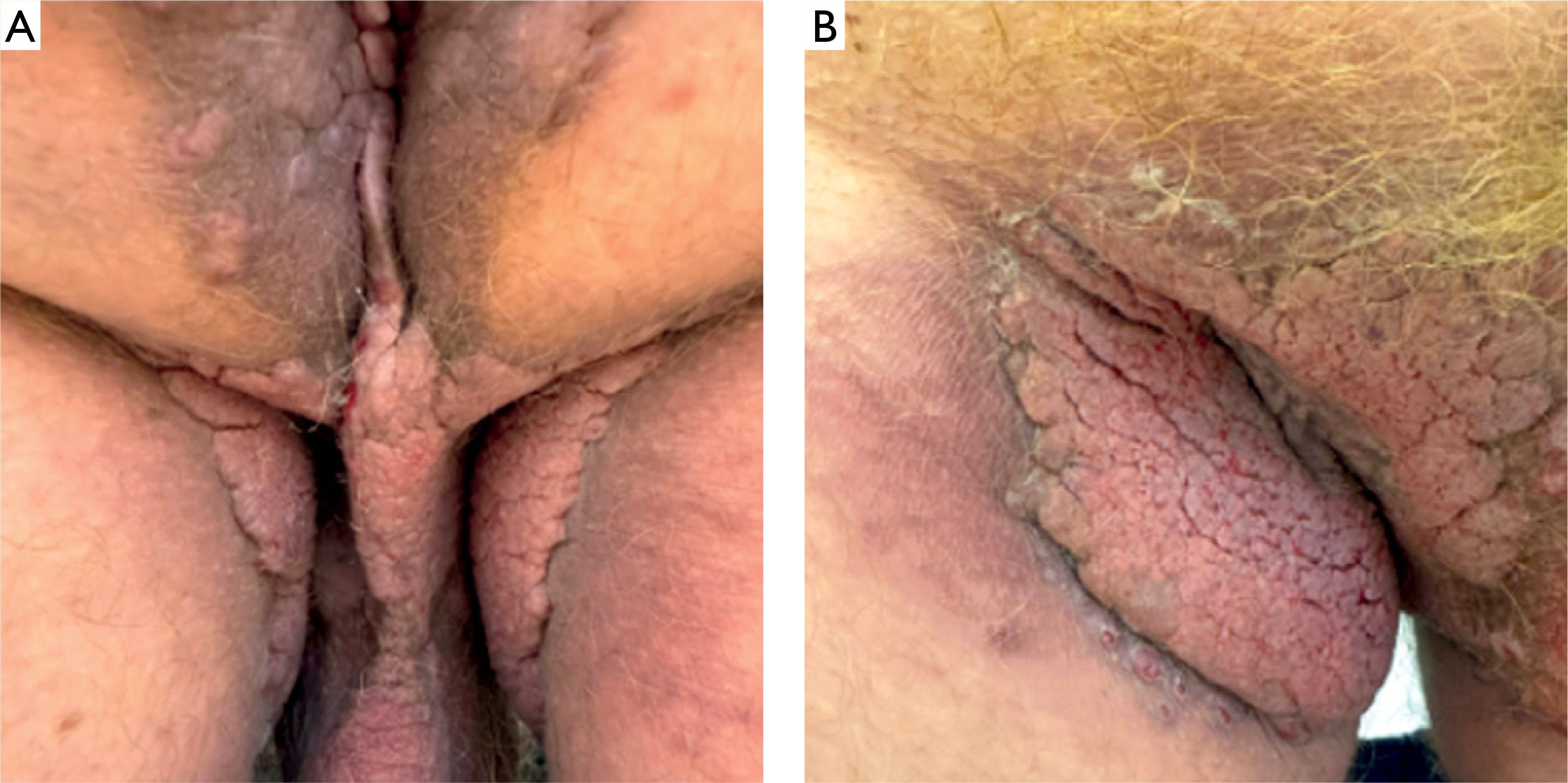
Figure 2
A, B – Erythematous verrucous lesions in the groins covered with exudate associated with intense malodour

Laboratory investigations performed on admission, and repeated 3 days and 1 week after, revealed elevated inflammatory markers, such as C-reactive protein (CRP) 53.3 mg/l, leukocytosis 11.01 × 103/µl, thrombocytosis 396 × 103/µl, and mildly increased procalcitonin 0.38%. Serological tests for syphilis (TPHA and VDRL) were negative. Swab cultures from the groin detected abundant growth of Staphylococcus aureus.
Chest X-ray revealed parenchymal opacities in both lungs. Abdominal ultrasound was unremarkable.
The histopathological examination of three skin biopsies from the groin, perianal area, and scalp demonstrated similar findings consisting of epidermal acanthosis with papillomatosis, hyperkeratosis with focal parakeratosis, and discrete suprabasal acantholysis. Eosinophilic infiltrates were present within the epidermis forming abscesses. The findings were consistent across all samples and supported the diagnosis of Pveg (figs. 4, 5).
Figure 4
Low-power view showing a suprabasal intraepidermal cleft (asterisk). The overlying epidermis demonstrates florid hyperplasia with eosinophilic microabscesses; a dense inflammatory infiltrate within the epidermis and the superficial dermis is present (H&E, ×4)
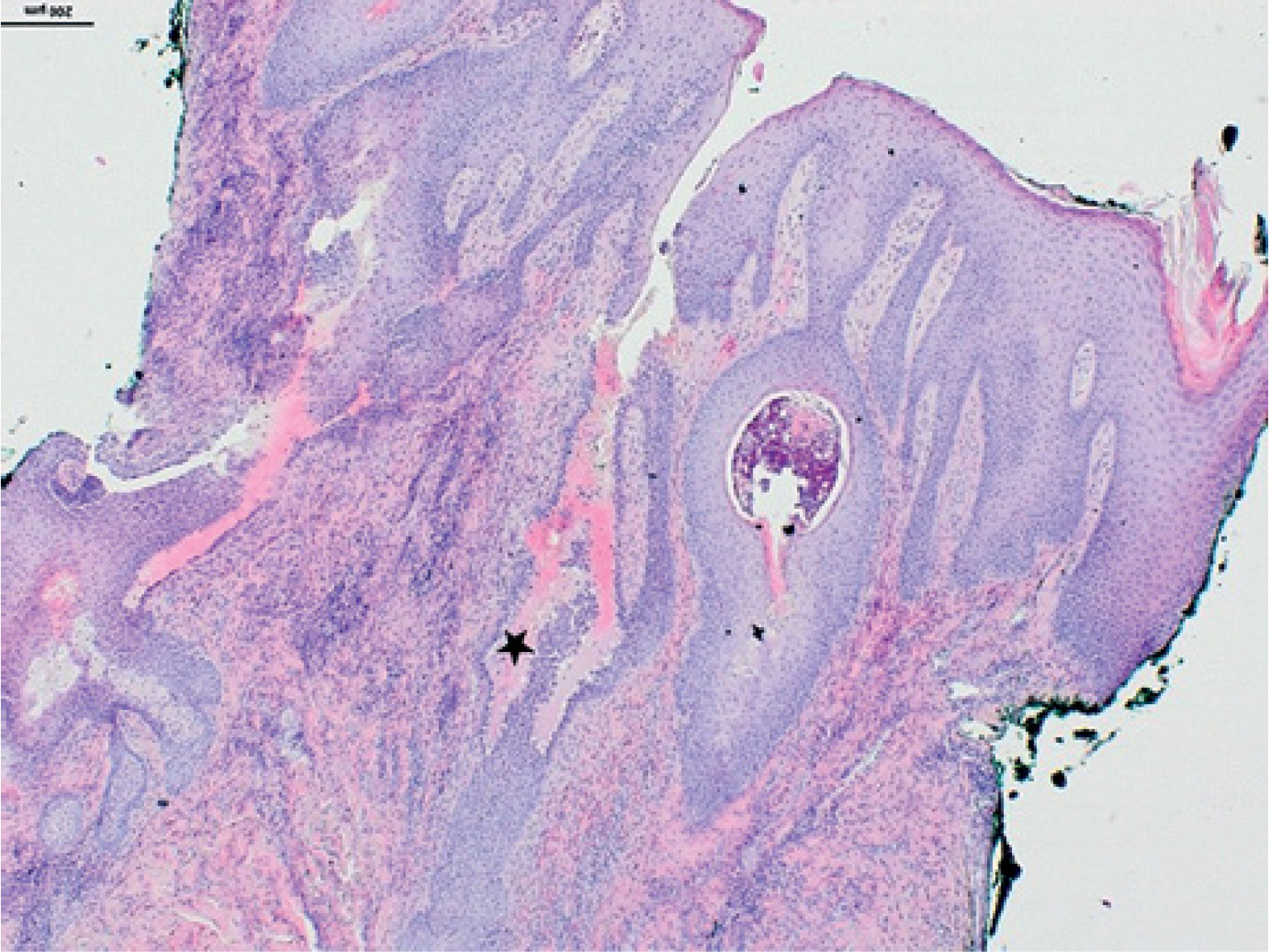
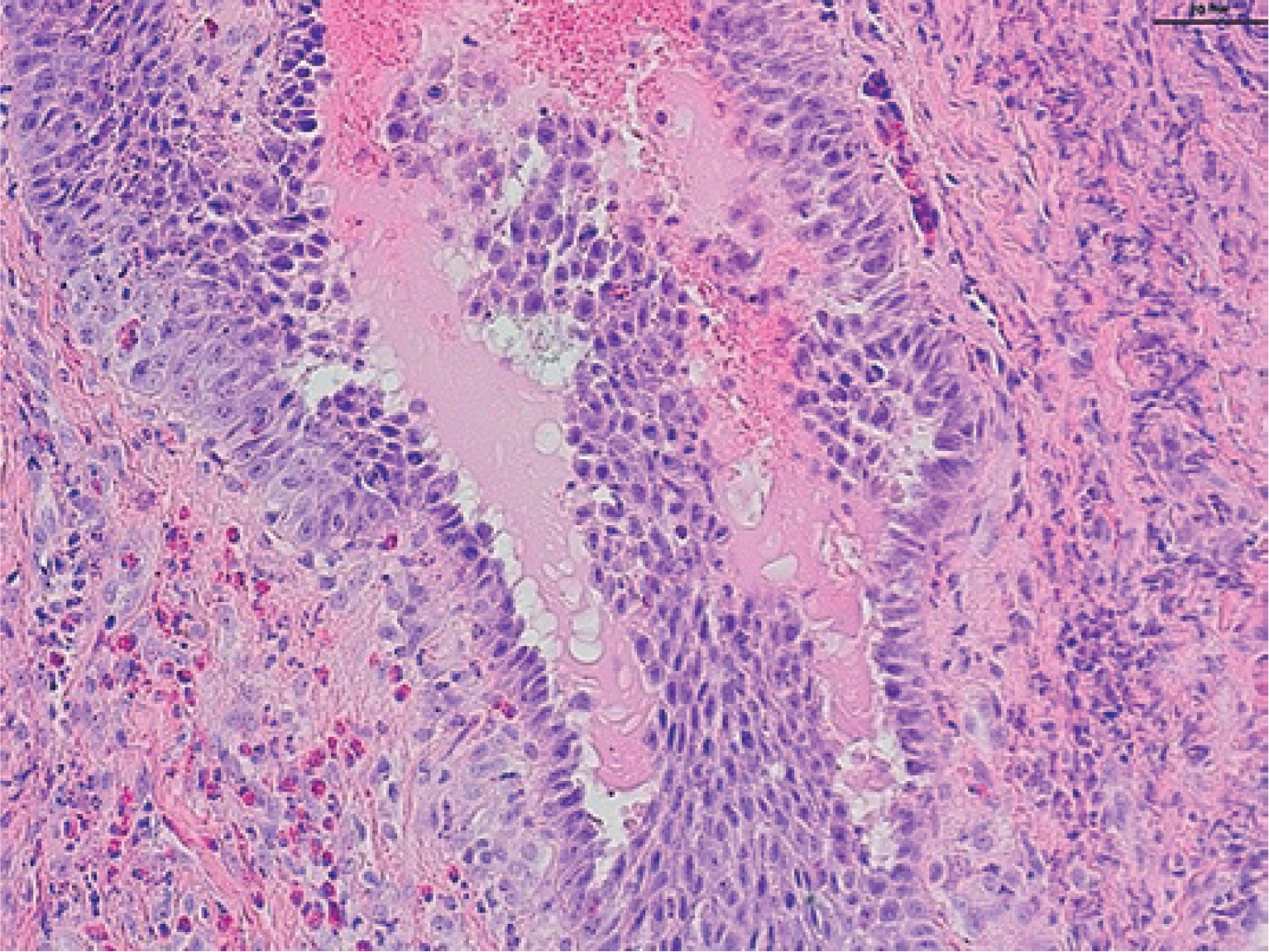
Figure 5
High-power view showing a suprabasal blister with detached and acantholytic keratinocytes. The basal layer remains attached to the dermoepidermal junction, forming the characteristic “row of tombstone” appearance. In the dermis mixed cell type infiltrate rich in eosinophils is visible (H&E, ×20)
DIF demonstrated intercellular IgG4 deposits with a characteristic “fishnet” pattern (fig. 6). Indirect immunofluorescence (IIF) revealed circulating pemphigus antibodies at a titer of 1 : 160. Enzyme-linked immunosorbent assay (ELISA) confirmed the presence of IgG autoantibodies against desmoglein 3.
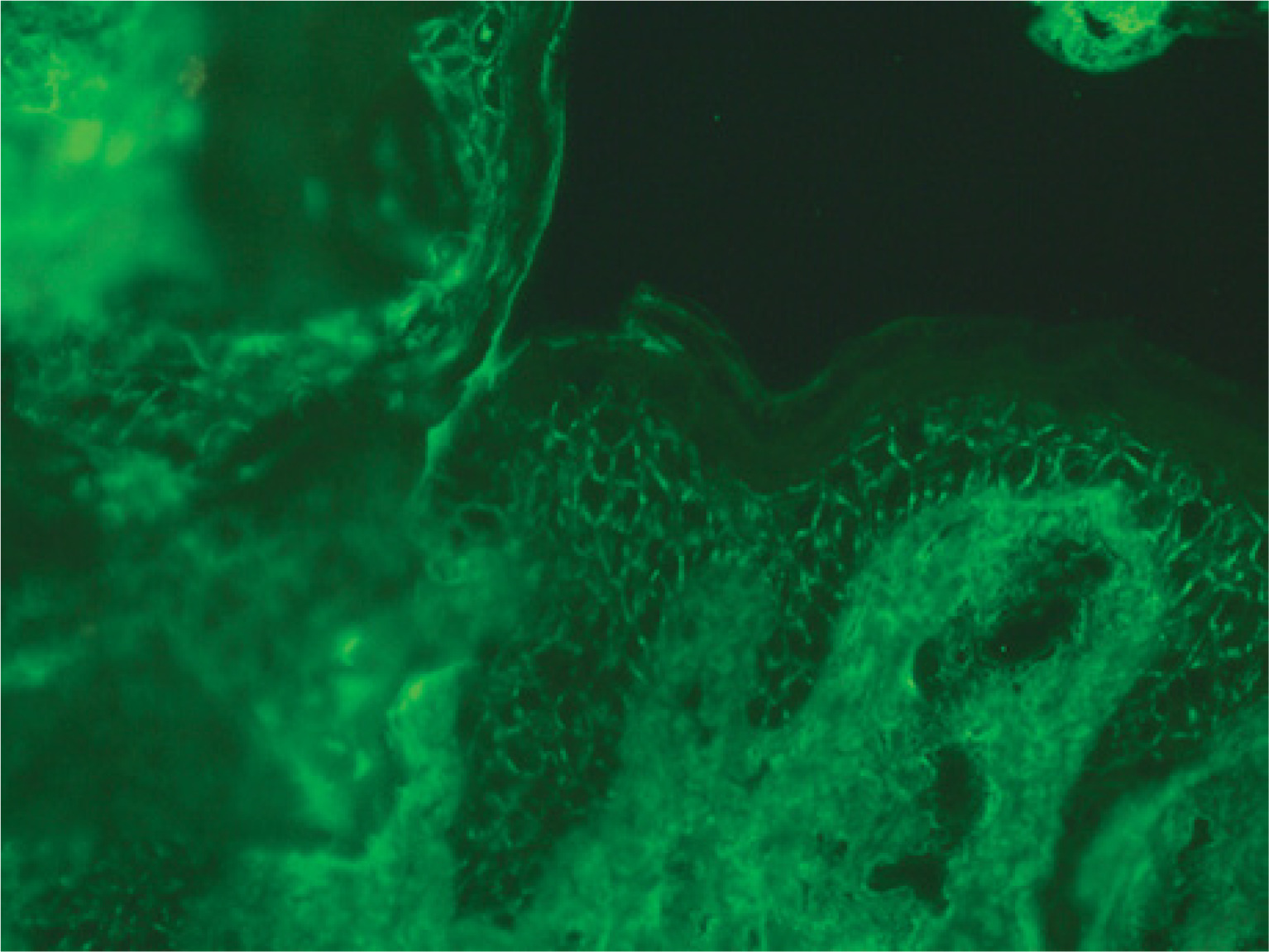
Figure 6
Direct immunofluorescence demonstrating intercellular IgG4 deposits in a characteristic fishnet pattern
Based on clinical, pathological presentation and additional investigations, Pveg, Hallopeau subtype, was diagnosed.
The patient was treated with prednisone 40 mg once daily, doxycycline 100 mg twice daily, fluconazole 50 mg once daily, and dapsone 100 mg once daily. Topical therapy included clotrimazole cream and metronidazole paste.
A rapid clinical improvement was observed within the first week of treatment, including reduction of exudate, resolution of malodour, and flattening of the lesions (figs. 7–9).



DISCUSSION
Pemphigus vegetans (Pveg) is the least common clinical form of pemphigus. It is considered a subtype of pemphigus vulgaris, accounting for 1–2% of all cases [6]. It is frequently difficult to diagnose and may be clinically misleading due to its variable presentation and the presence of verrucous vegetations [7]. It is characterized by flaccid blisters that evolve into erosions and eventually form fungoid vegetations or papillomatous proliferations, most commonly in intertriginous regions and on the scalp or face; however, the trunk, arms, legs, and flexural areas may also be affected. A few weeks to months after mucosal blistering, early lesions may appear as pustules rather than vesicles, but they rapidly develop into vegetative plaques [1]. The development of vegetating lesions in intertriginous areas may be related to occlusion and maceration, followed by bacterial infection, suggesting a reaction to superinfection. Immunopathological factors, including Th2-mediated immune responses, IgG4–IgG2 autoantibody profiles, and cytokines, contribute to epithelial proliferation and eosinophil chemotaxis [8]. Two clinical subtypes of Pveg are recognized: Hallopeau and Neumann. The Hallopeau type progresses more slowly and is characterized by pustules that evolve into vegetative plaques, whereas the Neumann type is more severe and resistant to treatment, with vegetations arising during vesiculobullous eruptions [9].
Lesions most commonly affect large skin folds (axillary, inframammary, inguinocrural, and intergluteal), where semi-occlusion, maceration, and mixed infections promote exudation and granulation tissue formation. Smaller folds, such as the nasolabial, labial, and periumbilical regions, may also be involved [5]. The oral mucosa is typically affected, and involvement of the vermilion border may serve as a clinical indicator. In the oral cavity, hyperkeratotic plaques may appear on the tongue in a cerebriform pattern. The exuberant cobblestone pattern of the lips and oral mucosa observed in the present case, together with significant weight loss, emphasizes the clinical relevance of oral involvement in Pveg [10, 11].
The etiopathogenesis of pemphigus remains not fully understood. Various triggers have been implicated, including medications, infections, surgery, trauma, and stress. Some reports suggest that Pveg may develop after surgical procedures, such as Mohs micrographic surgery or cryosurgery. Several mechanisms have been proposed to explain how surgical stress induces pemphigus, including Koebnerization of pre-existing disease. The Koebner phenomenon (KP) refers to the development of lesions typical of certain dermatoses in previously unaffected skin following trauma and is rarely reported in pemphigus. Epidermal damage may expose desmogleins 1 and 3, leading to the production of new autoantibodies in genetically predisposed individuals or activation of pre-existing subclinical antibodies. Furthermore, surgical trauma may trigger epitope spreading, resulting in an immune response directed against pemphigus-related antigens [12, 13].
We report a patient with Pveg who developed a cauliflower-shaped, nodular, brilliant red masses in the intertriginous genital area, surrounded by extensive erythematous lesions covered with exudate. On the scalp, erythematous and erosive plaques covered with crusts were observed. These lesions were accompanied by an intense malodorous discharge [14]. Although pemphigus lesions are typically associated with a “mousy” odor, the sweet odor observed in this patient may be attributed to secondary infection with Staphylococcus aureus, which produces volatile compounds contributing to wound odor [15]. Moreover, hyperkeratotic plaques on the tongue in a cerebriform pattern suggest long-standing disease. These findings are consistent with previous reports, including cases of the Hallopeau subtype, characterized by pustules that coalesce, erode, and evolve into moist vegetating plaques [14].
Dapsone was selected as pharmacological therapy due to its established efficacy in immunobullous diseases, particularly those involving neutrophilic infiltration. It acts as both an anti-inflammatory and antimicrobial agent. The inhibition of neutrophil activity by dapsone, combined with the broad anti-inflammatory effects of prednisone, may result in a synergistic therapeutic effect [16]. Its use may also help reduce steroid dependence and limit long-term adverse effects associated with systemic corticosteroids and other immunosuppressive agents [17]. Dapsone is administered at the doses of 100–200 mg daily and may be combined with other agents, such as mycophenolate mofetil or azathioprine [18]. Clinical improvement is often observed within 2–3 weeks, followed by gradual reduction of corticosteroid doses within 1–3 months. Reported efficacy rates of dapsone as an adjunctive therapy range from 71% to 83.3% [19].
In this patient, treatment with oral prednisone (40 mg/day) and dapsone (100 mg/day) resulted in progressive clinical improvement. The lesions improved steadily, and the therapy was well tolerated, with no reported adverse effects. These findings support the diagnosis of Hallopeau-type Pveg.
There are cases in the literature in which prednisone monotherapy resulted in only partial improvement, requiring the addition of dapsone and dose escalation of corticosteroids. However, dapsone therapy may be associated with adverse effects, including hepatotoxicity. Cases of dapsone-induced hepatitis have been reported, emphasizing the importance of regular monitoring, including complete blood count, renal and liver function tests, and abdominal ultrasound when indicated [20].
Pemphigus if left untreated can be potentially life-threatening condition, due to extensive skin involvement, secondary infections, and malnutrition. Common secondary infections include Staphylococcus aureus, MRSA, herpes viruses, and fungal pathogens. Oral involvement may lead to reduced oral intake, weight loss, and nutritional deficiencies. Mortality rates are estimated at 5–15% annually [21, 22].
The limitation of this report is the lack of the access to the original histopathologic and DIF materials from 2011, which precludes definitive retrospective confirmation of the initial diagnosis. It is possible that the patient was misdiagnosed at that time or that an overlap or sequential evolution between autoimmune blistering diseases occurred. Nevertheless, current histopathological and immunopathological findings strongly support the diagnosis of Hallopeau-type Pveg.
CONCLUSIONS
Pemphigus vegetans (Pveg) is a rare subtype of pemphigus vulgaris that remains diagnostically challenging due to its variable clinical presentation and resemblance to other dermatoses. It typically evolves from flaccid blisters into erosions and subsequently forms vegetating or papillomatous lesions, most commonly in intertriginous areas.
Treatment with oral prednisone (40 mg/day) combined with dapsone (100 mg/day) resulted in marked clinical improvement, including reduction of lesions in the groin and scalp. The patient was discharged after 10 days of hospitalization and continues treatment on an outpatient basis.










