
Introduction
Osteoarthritis (OA) of the hip is one of the most common musculoskeletal diseases that significantlyaffect the patients’ quality of life (QOL) [1]. Total hip arthroplasty (THA) has been considered the gold standard in the treatment of end-stage OA of this joint, and one of the most effective operations in modern surgery [2]. In most cases, the surgery makes it possible to restore the joint function, increase physical activity, relieve pain and improve the quality of life (QOL) [3, 4]. Total hip arthroplasty can be performed using a variety of surgical approaches – each with its own benefits and risks. It is believed that the use of minimally invasive (MIS) approaches, e.g. anterior MIS, reduces blood loss, surgery-related pain, hospital stay and the recovery period due to the potential reduction of soft tissue damage [5–7]. The opponents of these methods state that MIS approaches, through less exposure of the joint, may increase the risk of complications such as nerve or muscle damage, fracture, or dislocation [8].
Overall, THA is associated with a low rate of complications and long life of the prostheses [9]. One of the complications is heterotopic ossification (HO), which is defined as the ectopic formation of bone in non-bone tissue [10]. Heterotopic ossification is believed to be a result of osteoinductive growth factors released due to the trauma of soft tissues [11]. The risk of ossification is estimated at 24% to as high as 32% [12]. Prophylaxis options include selective and non-selective non-steroid anti-inflammatory drugs (i.e. etoricoxib, indomethacin or diclofenac) and radiation therapy, which is the only prophylactic method that can be administered locally [13–15]. Heterotopic ossification prophylaxis should be administered shortly after surgery, during the initial inflammatory response [13]. However, there is no consensus as to which prophylactic protocol is the most effective. In most cases, HO is asymptomatic. It is estimated that 2–7% of patients experience symptoms such as limited range of mobility (ROM) and function of the hip joint, and pain [11, 16]. In symptomatic cases, treatment may be necessary. The methods include rest, nonsteroidal anti- inflammatory drugs, physical therapy, and possibly a steroid injection [17]. Some patients require revision surgery of the hip and removal of ossification [5]. The first radiological features of HO appear within 4–6 weeks of surgery [13]. The lesions mature for the first 6 months and generally do not further progress in the later stages [11]. The surgical approach used may affect the incidence and degree of HO [5].
We present a comparison of the results of total hip arthroplasty using two surgical approaches: anterior MIS and anterolateral (Watson-Jones – WJ) in terms of HO and the QOL and functional scores. Prior to the study, the authors formulated the hypothesis that the anterior MIS approach may favor better clinical and functional outcomes of surgery, and reduce the frequency and severity of HO.
Material and methods
Characteristics of study population
The study was retrospective and it consisted of medical data analysis of consecutive patients operated on at the Department of Orthopedics and Traumatology, Medical University of Warsaw in the years 2009–2013, as well as the results of those who came for an ambulatory follow-up visit in 2016. At the beginning, 597 patients were included. The inclusion and exclusion criteria are listed in Table I. Baseline data were obtained from medical records in the form of medical history and X-ray images of consecutive patients operated on in 2009–2013 with the WJ or MIS approach. All patients received similar perioperative care. None of them received prophylaxis of ossification in the form of radiotherapy or non-steroidal anti-inflammatory drugs. All procedures were performed in accordance with the guidelines of the Declaration of Helsinki (DoH) and were approved by the ethical review board (ERB) of Warsaw University of Medicine. Informed consent was obtained for all of the study participants.
Table I
Study inclusion and exclusion criteria
Description of operative methods
All patients were hospitalized in the Department of Orthopedics and Traumatology, 1st Faculty of Medicine at the Medical University of Warsaw. Operations were performed in the same surgical theatre and with the same personnel. All patients were operated on by two senior orthopedic surgeons (Ph.D. degree) experienced in total hip arthroplasty performed with both the Watson-Jones approach and the anterior mini-invasive approach. The only contraindication for the minimally invasive approach was developmental of hip dysplasia with significant shortening of the limb. In all other cases the selection was random. Length of the incision was 12 cm in the WJ approach and 8 in MIS.
WJ approach
The incision line began at a point located approximately 3 cm laterally and distally from the anterior superior iliac spine (ASIS), and followed a curve towards the greater trochanter. Over its top, the incision direction was consistent with the femoral axis, and it reached 10–15 cm along the femur. The approach was made by identification of the fascial compartment that exists between the tensor muscle of the broad fascia and the gluteus medius muscle.
Anterior MIS approach
Typically, the incision was started 2 cm distally and laterally from the ASIS and continued distally and laterally, along with the tensor muscle of the broad fascia and its fascia. The fascia was dissected along the course of the muscle fibers. Then the space between the tensor muscle of the broad fascia and the sartorius muscle was located and they were separated from one another to expose the hip joint capsule [18].
Follow-up methods
Complete follow-up (clinical and HO assessment) involved 238 patients who returned for follow-up visits in 2016. A group of 3 senior orthopedic surgeons (Ph.D. degree) work in the out-patient clinic. During the FU visit, standard X-ray of hip joints and questionnaires of objective and subjective hip function assessment were applied. The functional parameters of the operated limb were evaluated using the following scales: The Western Ontario and McMaster Universities Arthritis Index (WOMAC), the Visual Analogue Scale (VAS), the Harris Hip Score (HHS), and the Hip and Knee Arthroplasty Satisfaction Scale (HKASS). The HHS scale was completed by the doctor on the basis of previously conducted physical examination and medical interview; thus blinding was impossible. VAS, WOMAC and HKASS were completed by patients themselves, thus eliminating a potential source of bias. The patients had been informed to ask questions when in doubt. All examinations, both in WJ and MIS groups, were identical. A full orthopedic physical examination was also performed with measurement of the ROM of the operated limb, and FU anteroposterior (AP) X-ray scan of the hip joint was obtained to assess prosthesis positioning. Doctors assessed HO after the FO visit and only on the basis of previously prepared X-rays. Demographic data (name, surname and ID number) had been removed by an independent person. Assessment on Brooker’s scale and ossification was extended to people who did not return for FU visits but had an X-ray done at least 6 months after surgery (n = 331).
The Brooker’s scale assessment results are presented in Table II.
Table II
Description of classes in Brooker’s scale, used to assess heterotopic ossification
Statistical analysis
Continuous variables were described using range, mean, standard deviation, and median, with minimum and maximum values for the distribution. The χ2 test was used to compare categorical variables. The Mann-Whitney U test was used to compare the medians of continuous variables between independent groups of observations. Pearson’s correlation was used to compare correlations between quantitative variables. The level of significance was set at 0.05. For multivariate modeling of the data, linear regression and the step elimination method were used to obtain the significant parameters of the model. All calculations were performed using the R statistical software, version 3.2, and SPSS, version 24.
Results
The study population consisted of patients operated on using the anterior MIS approach (47.1%, n = 282), and operated on using the classic WJ approach (52.9%, n = 315). Women slightly prevailed (58.4%, n = 348) over men (41.6%, n = 248). The oldest participant was 88 years old, and the youngest one was 18 years old. Mean age was 63.10 ±13.44 years. Mean BMI was 27.55 ±4.75. The most common reason for THA was primary OA of the hip. The number of patients who returned for a follow-up (FU) visit was 238 out of 597 (39.9%). On average, the FU visit occurred approximately 3.5 years (1273.5 days) after the procedure. The number of reporting patients who had been operated on using the anterior MIS approach (n = 116) was nearly equal to the number of patients who had been operated on using the WJ approach (n = 122).
The presence of HO after THA was compared between the surgical approaches used. In the entire population with an X-ray performed at least 6 months after surgery, ossification was present in 168 (50.76%) patients. The frequency of ossification was slightly higher in the anterior MIS arm (63/120, 52.5%) compared to the WJ arm (105/211, 49.76%). Taking into account only patients with ossification, it can be seen that higher classes of ossification were seen with the WJ approach. However, the differences were not statistically significant (p > 0.05).
For the score assessing the degree of ossification after the procedure, a higher score was obtained in older people (R2 = 0.02, Pearson’s r = 0.02 ±0.01, p < 0.05).
In addition, the score was higher when osteoarthritis was not the reason for surgery, but not statistically significant (R2 = 0.02, Pearson’s r = –0.45 ±0.30, p = 0.14). The detailed results relating to the presence of HO for the two approaches are presented in Table III.
Table III
Percentage distribution of the frequency of each ossification class for the compared approaches
Patients who underwent THA using the WJ surgical approach had higher WOMAC scores, indicating a higher severity of post-operative symptoms. The multivariate model for the WOMAC scale indicates that the most important parameters determining the WOMAC score include the type of surgical approach (R2 = 0.05, Pearson’s r = 6.31 ±2.24, p < 0.05) and BMI (R2 = 0.05, Pearson’s r = –0.37 ±0.24, p = 0.11), although only the former of these factors was statistically significant.
On the VAS scale, 34% of patients, among those who assessed the severity of pain, reported no pain. In the case of the MIS approach, women rated pain as significantly lower than men. Using this scale, the strong effect of using the WJ approach on this score is visible (R2 = 0.05, Pearson’s r = 8.54 ±2.85, p < 0.05). Patients who underwent THA using the WJ method had higher VAS scores, which could indicate a lower severity of pain in patients operated on using the ASI approach. However, the Mann-Whitney U test did not confirm the statistical significance of these differences (p = 0.059).
Patients in whom the procedure was performed using the MIS approach more often rated the outcomes of surgery as good or very good on the HHS scale. With the WJ method, moderate or poor efficacy of the performed surgery was more common (the score was 70–80 or less, respectively) compared to the MIS approach. Men rated the function of the prosthesis when performing everyday activities higher than women (the median HHS scores were 39 and 41 points, respectively). The significance of the differences was confirmed by the Mann-Whitney U test (p < 0.01). However, for the MIS approach, there were virtually no sex-related differences in the function of the hip prosthesis. The situation was different for WJ surgery, where women rated the prosthesis function as significantly lower. The multivariate model for the HHS scale indicated an important role of the surgical approach, also in favor of the MIS approach (R2 = 0.07, Pearson’s r = –4.82 ±1.90, p = 0.01). In the HHS scale use of cement reduces the average score by 5.86 points (R2 = 0.07, Pearson’s r = –5.86 ±2.08, p = 0.01).
The HKASS scores indicate that patients undergoing surgery using the MIS approach were more satisfied with the results of the procedure than patients in whom the WJ approach was used (R2 = 0.05, Pearson’s r = –10.13 ±3.01, p < 0.05). The use of bone cement decreases the score, but it is not statistically significant (R2 = 0.05, Pearson’s r = –7.30 ±4.09, p = 0.08). In addition, there is a positive correlation between age and the scale (R2 = 0.05, Pearson’s r = 0.31 ±0.15, p < 0.05), indicating that older people are more likely to have higher scores on the scale.
The exact results on each scale depending on the approach used are presented in Table IV and Figure 1.
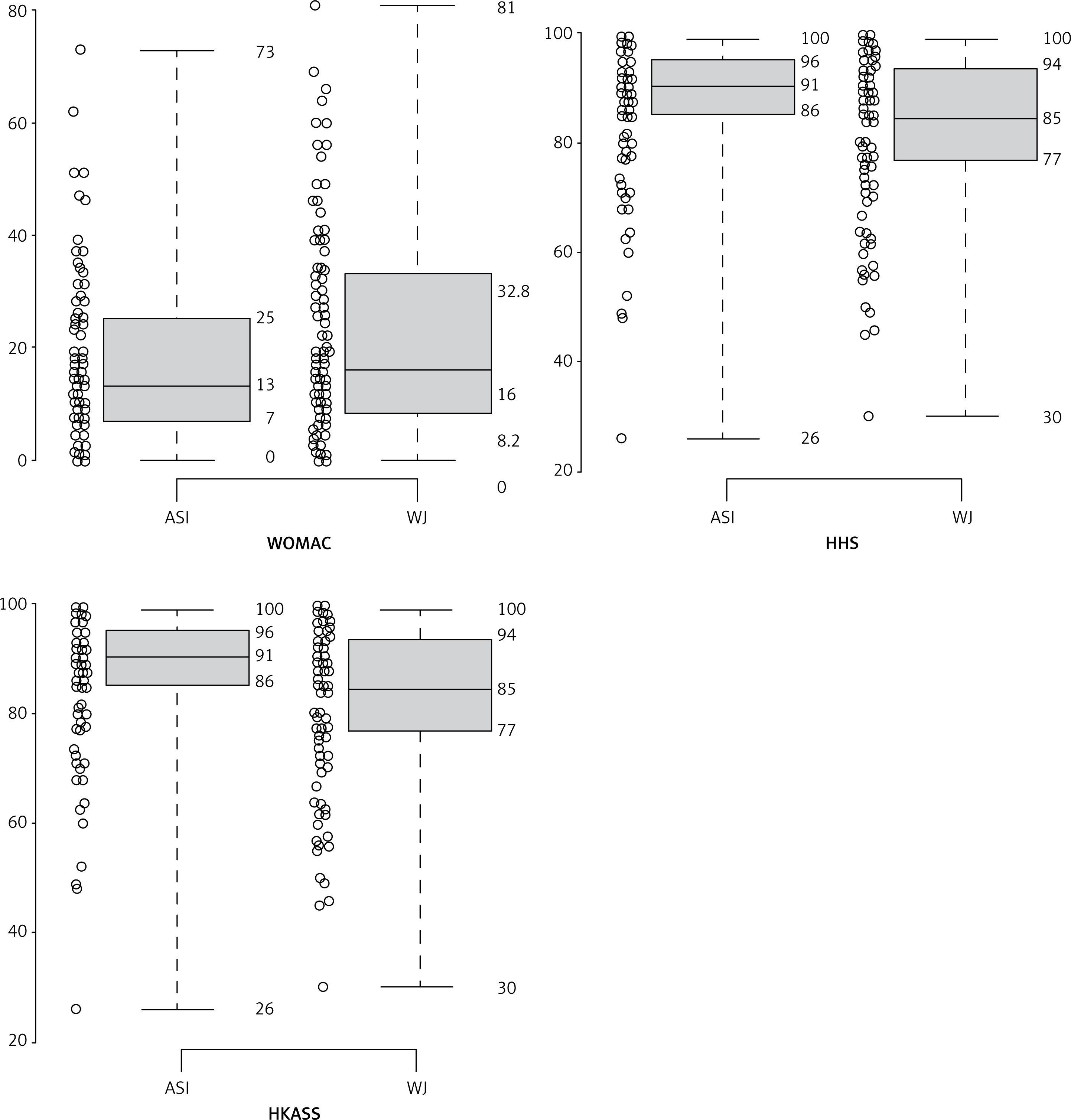
Table IV
Results of orthopedic scales evaluating the quality of life
Discussion
There is no consensus on the optimal surgical approach. Studies comparing the anterior MIS approach to other surgical approaches are limited. The problem is particularly apparent in terms of HO. According to the studies comparing the most common approaches, the WJ approach seems to be strongly predisposing patients to ossification [15, 19]. According to Newman et al. [20], the HO rate after surgery using the anterior MIS approach is 24.3%. With the WJ approach, it was rated at a similar level of 24% [21]. Repantis et al. [22] also reported no statistically significant differences in the assessment of HO between the cohorts of patients after THA using the anterior MIS and WJ approaches. Tippets et al. [11] did not observe any reduction in the incidence of HO after using the direct anterior approach (DAA), the other name for anterior MIS, when comparing their patients’ results to the other results obtained with different approaches described in the literature. In a cohort of 331 patients with an X-ray obtained 168 (50.8%) developed ossification. The distribution of ossification grade was as follows: 0 (n = 163, 49.2%), I (n = 63, 19.0%), II (n = 54, 16.3%), III (n = 40, 12.1%), IV (n = 11, 3.3%). Also in our study, we did not observe a significant reduction in the frequency of ossification after using the DAA (MIS) approach. The highest proportion of ossification for the anterior approach was in class I (25.8%).
The most commonly used scales in the analysis of THA surgery outcomes are WOMAC, HHS, and VAS. In a study comparing DAA and direct lateral (DL) approaches, statistically significant superiority of the former method was found in 1-year follow-up based on the WOMAC score. After 2-year FU, the difference between the groups was no longer statistically significant [23]. Other authors have also demonstrated the advantages of the anterior MIS approach in a short-term FU assessed using the WOMAC and HHS scales [24]. Pogliacomi et al. [5] compared the results of surgery using the MIS lateral approach and MIS anterior approach. The authors observed similar, satisfactory results of surgery and similar complication rates in both groups. Based on the VAS scale completed both pre-operatively and 1 year after THA, the authors reported a lower severity of pain shortly after surgery in the group operated on using the anterior MIS approach. Also on the HHS scale, they reported good results of THA surgery using the anterior MIS approach. Our study confirmed that the anterior MIS approach gave satisfactory results on the VAS scales, although the difference between WJ and ASI was not statistically significant. Another prospective study, in which patients were randomized to the DAA and posterior approach, showed the superiority of the former method in terms of pain relief on the first day after surgery assessed using the VAS scale. There were no statistically significant differences between the two groups at the subsequent FU visits [25].
Mirza et al. [26] presented the results of a study comparing the results of 1690 primary THAs, performed using the MIS anterior approach or the DL approach. The results showed that patients in the arm operated on by the MIS anterior approach had a shorter recovery period and better HHS scores in the short post-operative period. Similar results have been reported by other authors, comparing THA using the DAA (direct anterior approach) and the minimally invasive posterior approach [27]. They reported higher HHS scores at 8 weeks post-operatively compared to the group of patients operated on using the posterior approach, and a lower risk of wound healing complications. Rodriguez et al. [28] compared the DAA and posterior approach and showed the superiority of the DAA approach in the immediate post-operative period, related to recovery and mobility. In our study, we did not investigate the results of surgery in the short term after the operation; however, our results obtained in the medium follow-up period showed that good outcomes in THA using the anterior MIS approach, based on the clinical scores, may be maintained not only in the immediate post-operative period, as shown in the previously reported studies, but also in the medium term.
The most significant limitation of this study is its retrospective nature, and thus no randomization of approach applied for each patient. Furthermore, a large group of patients has not been evaluated at an FU visit (60.1%). It should be emphasized that WJ was the standard approach used at our department for many years, whereas the MIS approach was introduced in 2009. It is therefore possible that the slightly worse results in terms of the frequency of ossification were related to the learning curve. The impact of the learning curve on THA has been previously suggested in the literature [29, 30].
The advantages of this study include a large population and the detailed method of data collection at the FU visit. According to the authors’ knowledge, this is also one of the few available studies comparing the incidence of HO for the anterior MIS and WJ approaches. Thus we believe that the results may be helpful to other clinicians in making preoperative plans and decisions.
In conclusion, the frequency of heterotopic ossification was slightly higher in the anterior MIS approach compared to the WJ approach, but the difference was not statistically significant (p > 0.05). Considering only patients with ossification, higher grades of HO were noted in the WJ approach. However, the differences were not statistically significant (p > 0.05). The MIS approach was associated with better clinical and functional outcomes according to results of all clinical scales applied, except VAS.