Introduction
Multidetector computed tomography (MDCT) is the reference standard for the diagnosis of peripheral arterial disease (PAD) [1,2]. It is reported that PAD is the second most common disease, after myocardial infarction and stroke, and results in an estimated [3]. Early diagnosis and appropriate medical interventions can mitigate limb-specific symptoms, improve quality of life, and decrease systemic cardiovascular risk [4]. Computed tomography angiography (CTA), as a non-invasive and safe examination, has been widely used in clinical practice to diagnose PAD and acute lower-extremity vascular injury with high accuracy [5-8].
Several studies had revealed the overuse of CTA to exclude PAD, which increases in effective dose per patient [9], so there is a need for reduction of radiation dose. Therefore, the recent studies of PAD CTA have conducted important updates on optimising protocols that restrict the amount of iodinated contrast media, thus decreasing the risk of contrast medium-induced nephropathy, particularly in people suffering from certain diseases such as diabetes and high blood pressure [10]. Thus, lowering the radiation dose by using 128 MDCT scanning and low contrast medium volume CTA protocols is potentially advantageous both to reduce radiation-derived risks and to prevent contrast medium-induced adverse events.
The combination of 70 kVp and high-pitch acquisition technique holds the potential to further reduce the radiation dose with a reduction of the amount of iodine contrast injected during the image scan. The aim of our study was therefore to investigate the feasibility, image quality, and radiation dose of lower extremity CTA using 70 kVp combined with high pitch acquisition and less iodinated contrast medium injected during PAD scanning.
Material and methods
Subjects
This study was held by An-Najah National University in Nablus city, Palestine. Each individual was referred for lower extremity CTA for clinical suspicion of PAD exam. To be eligible for the study patients had to have normal renal function. Patients with a personal history of allergy to iodinated contrast material, or impaired renal function (creatinine > 1.2 mg/dl) were excluded from the study. The study subjects were divided into two groups. Patients in group A (18 male and 18 female, mean age 63 years, standard deviation 15, range 20-88 years) underwent a novel lower extremity CTA protocol consisting of optimised care dose selection and low contrast medium volume (80-85 ml) acquisition, whereas group B (18 male and 18 female, mean age 61 years, standard deviation 16, range 26-88 years) had conventional PAD CTA protocol with optimised care dose selection and iodine contrast volume (120-140 ml).
Lower extremities computed tomography angiography protocol
All lower extremities CTA examinations were performed using a 124MD CT system (Somatom Definition, Siemens Healthcare, Forchheim, Germany) for group A – the acquisition parameters were: pitch = 1.3, low contrast medium volume = 80-85; flow rate = 4; bolus tracking technique with Hounsfield attenuate threshold = 80-85 HU, and delay scan time after the contrast triggering in bolus-tracking technique 6 seconds without breathing instruction before data acquisition. For group B the acquisition parameters were: pitch = 0.8; contrast = 120-140 ml; flow rate =4; HU predefined attenuation threshold with delay scan time after the contrast triggering in bolus-tracking technique 8 seconds with breathing instructions before data acquisition, bolus tracking with the region of interest placed in the main descending aorta at a level L2-L3 (care dose were selected for both group protocols), pure, undiluted iodinated contrast medium was used for both groups (Imoron 300), other parameters kept constant for both groups (slice thickness 3 mm, kVp = 70, and care dose selected for both groups).
Quantitative analysis of pulmonary computed tomography angiography images
All images were evaluated by two observers with one and three years of experience in CTA evaluation, blinded to the clinical history and lower extremity CTA protocol. Each study was subjectively classified as diagnostic or non-diagnostic by each reader.
The signal intensity for the peripheral arteries (SI vessels), given in HU, was defined as the attenuation measured by placing circular regions of interest (ROIs) in the centre of these vessels. The ROI size was adapted to the diameter of the vessel, reaching up to 40 mm2 in the central arteries. The main arteries were analysed by select common iliac, femoral, and popliteal artery left and right. In order to minimise bias, each artery was measured at three different locations. The mean of these values was used for further calculations.
The attenuation in the peripheral lower extremities arteries was ignored because unable to use the ROI method was not possible for assessment of the signal intensity due to their small calibre.
To define the image noise, the standard deviations of HU measured in ROIs of at least 40 mm2 drawn in three different regions outside the patient body (middle, left, and right sides) were averaged.
The signal-to-noise ratio (SNR) was defined as SI vessel/noise. The contrast-to-noise ratio (CNR) was defined as ([SI vessel – SI background]/noise). These two parameters were calculated separately for the central average for lower extremities arteries.
For statistical analysis SPSS software version 16.0 (SPSS Inc., Chicago, IL, USA) was used, and the independent sample t-test was employed to compare continuous variables. A two-sided p-value < 0.05 was considered to indicate a statistically significant difference.
Result
Among 16 consecutive individuals with suspected PAD CTA, without complications there were no significant differences observed in age, weight, and gender between groups A and B. Patient data are presented in Table 1. All studies were considered to have enough image quality to detect PAD (Figure 1). A total of 16 cases of PAD (22.2%) were found in the evaluated of subjects (10 in group A and six in group B). All PAD cases were detected by the two readers. There was no significant difference in the size or location of the PAD between the two groups.
Table 1
Structure of population study data, patient characteristics, signal intensity for the central pulmonary arteries, and image quality in the study groups
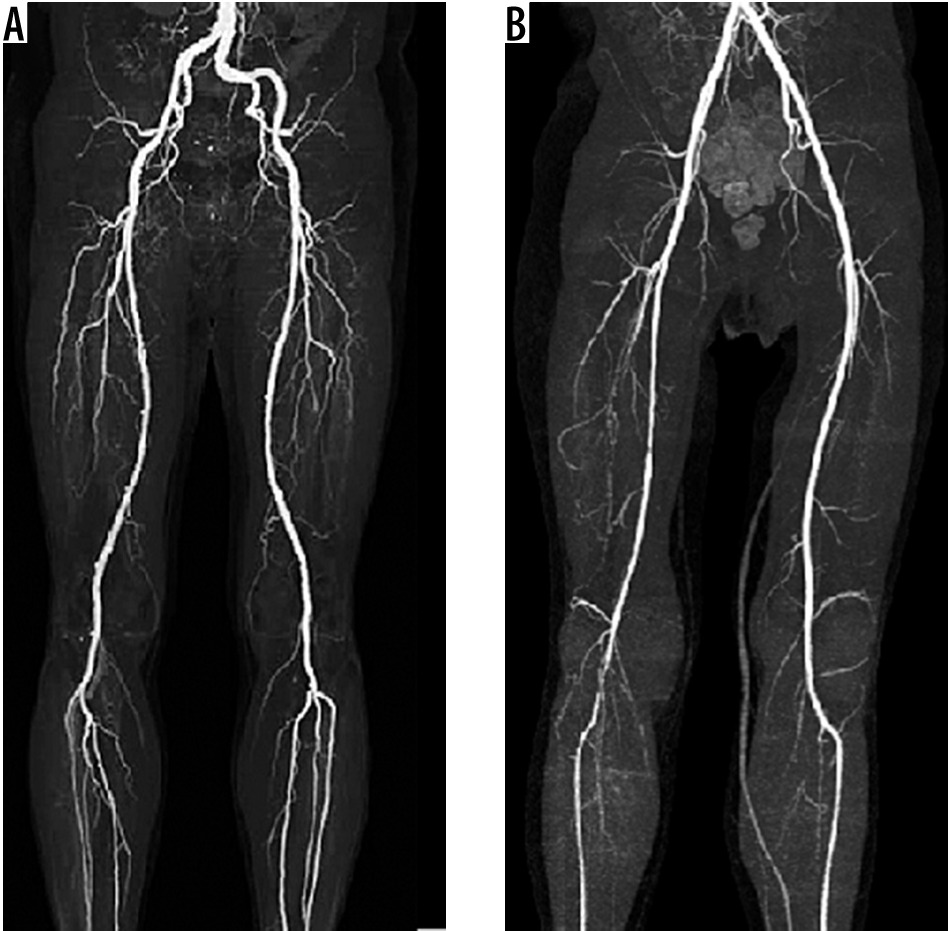
Figure 1
Exemplary 3 mm transverse peripheral arterial disease (PDA) computed tomography angiography images at 70 kVp from the present patient collective. A) Image scan with protocol A (contrast volume 80-85 cc and pitch = 1.3). B) Image scan with protocol B (contrast volume 120-140 cc and pitch = 0.8)
The average image noise was 19 HU for group A and 16 HU for group B. The difference was not statistically significant (p = 0.183). Overall, the SNR and CNR were slightly higher in group B (25.5 and 24.1, respectively) compared with group A (20 and 17.4, respectively), but those differences were not statistically significant (p = 0.61 and p = 0.38, respectively).
Discussion
In the present study, the two groups were matched by gender, age, and weight, thus exclude possible variations between the groups in the vessel enhancement secondary to a different body habitus. Conversely, volume, concentration, injection rate, and duration of iodinated contrast medium administration are factors directly associated with lower extremities artery enhancement. As shown, the reduction in acquisition times achieved with the newest CT equipment avoids the need for long-duration contrast medium administration protocols because the injection duration critically affects both the magnitude and timing of contrast enhancement [11-20], and this study used a 128 MDCT Siemens machine during lower extremities CTA scanning and managed to reduce the injection period to less than 50% during CT scanning, and this in turn reduced the size of the contrast medium to less than 40% of the value used in the classical lower extremities CTA scanning protocol.
The most relevant finding of this study is that in individuals weighing on average 85 kg, a lower extremities CTA protocol with relatively small volume of iodinated contrast medium (80 ml) results in lower extremities CT angiograms with lower injection period than when using a conventional lower extremities CTA protocol (Figure 1). The novel protocol proposed here yielded a diagnostic confidence of lower extremities that was not significantly different from the standard protocol but using 40% less intravenous contrast medium. This optimisation of a standard lower extremities CTA protocol may have been achievable due to the latest technology, such as thin collimation and shortened study time provided by the new MDCT equipment, the use of automatic initiation of the examination by the bolus tracking technique, and the infusion of a saline flush immediately following the contrast medium, which increase peak aortic enhancement by pushing contrast material into the cardiovascular system, which otherwise would be left in the injection tubing. Also the saline flush minimises streak artefacts from dense contrast, which increases SNR of the lower extremities [12,13].
It is known both that formal and CT lower extremity angiographies involve the injection of intravenous radiographic contrast under pressure, and this injection may develop cardiopulmonary arrest after contrast injection [21,22], so it is thought. The reduced amount of contrast to 40% undoubtedly will reduce the likelihood of cardiac arrest, and in turn will improve the use of CTA in diagnostic lower extremities in a large scale. Also it is noticeable that when the amount of contrast injection is reduced, it reduces beam hardening and streak artefacts (see Figure 1) causing obscuring adjust vessels during image scans, especially in the area of the superior vena cava.
The main limitations in this study are that it was a retrospective study analysis. In order to spare participants from double dose exposure, the study used data existing on the database in the hospital that were used in the survey of previously unknown lower extremities scanning and then compared them with the new protocols that use new standards through the screening to reduce the size of the contrast medium combined with a high injection rate, and this may strain the final results. Hence, in order to avoid any bias during comparison between the two scanning protocols, the author recommends that the data was collected from the same subjects on both protocols, and that iodinated contrast agents are needed for helical CT PAD angiography, and their use may not be possible in patients with impaired renal function or a severe allergy to the contrast material.
The present study demonstrates the feasibility of lower extremity CTA using 70 kVp combined with high pitch acquisition with a selective care dose option during image scanning, so there is no significant difference in radiation dose between the two protocols but a decrease of about 40% in the volume of contrast material compared to the standard protocol used in An-Najah hospital medical imaging department without compromising image quality. Lowering the tube voltage is an effective method to reduce radiation dose because of the exponential relationship between voltage and radiation dose [13]. Lowering tube voltage from 120 kVp to 70 kVp has been reported to result in a 30% reduction in radiation dose for lower extremity CTA [22]. In addition, increasing pitch is another method to reduce radiation dose by shortening the image acquisition time [14]. Amacker et al. reported that the mean radiation dose decreased by 20% and 42% when the pitch was increased from 1 to 3.2 for routine chest and abdominal CT scans, respectively [15], but it in our case there was no decrease in the amount of the dose due to the care dose option being selected during the image scan; this option increases the mAs during image scanning to reduce image noise, which led to increased image quality. On other hand, a decrease in the kVp during CTA scan will increased the attenuation of each unit of low iodine concentration because the low voltage helps improve blood vessels and elasticity while minimising the absorption of radiation at the same time, as long as there is no significant scattering of the beam or degradation of the image due to large tissue or bone along the X-ray path [6]. The reduction of the amount of contrast media also leads to the reduction of the cost and risk of side effects resulting from giving iodine in large quantities.