
Introduction
Due to pollution, urbanization, diet changes, and environmental causes, allergic dermatoses are rising. Exposure to pollutants and food additives disrupts skin barrier function and activates immunological processes, complicating the condition. Conventional techniques of assessing therapy effectiveness cannot account for pathogenetic pathways and clinical symptoms, limiting their diagnostic utility. The lack of objective skin barrier and systemic inflammation monitoring criteria makes therapy strategy adjustments difficult. Using immunological and molecular monitoring to diagnose and treat skin allergy disorders is promising. Biomarkers of skin allergy treatment efficacy can be used to evaluate new techniques of diagnosis, prognosis, and control of inflammatory processes. In atopic dermatitis and other allergic dermatoses, investigations examine Th2 inflammation, cytokine profile alterations, skin barrier dysfunction, and immunological modulation. Studies focus on immunoglobulin E (IgE), interleukin (IL) 4 (IL-4), IL-5, IL-13, and epidermal barrier disruption molecular markers: filaggrin, claudin-1, and loricrin. The results of these investigations can be used to evaluate current methodological approaches, uncover gaps in modern scientific thinking, and recommend opportunities for future research in tailored skin allergy therapy.
An analysis of the article by Gutowska-Ślesik et al. [1] revealed that the study focused on the prevalence of skin allergic diseases, but did not include the analysis of biomarkers (IgE, IL-4, IL-5, IL-13) and molecular monitoring methods (qPCR, NGS), which limited the assessment of pathogenesis and efficacy of therapy. Łoś-Rycharska et al. [2] found differences in the gut microbiota and skin microbiota of infants with atopic dermatitis, but the use of 16S rRNA sequencing without functional analysis did not allow determining the mechanisms of their action. The limited sample size, one-time nature of the analysis, and lack of consideration of possible confounders (antibiotics, nutrition) reduced the reliability of the conclusions. Kaziród-Wolski et al. [3] assessed the incidence of allergic reactions during coronary interventions, but did not consider pathophysiological mechanisms, did not factor in the immunological and molecular monitoring, which limited the personalisation of therapeutic approaches. Karłowicz-Bodalska et al. [4] evaluated the effectiveness of diphenhydramine and lidocaine therapy, but did not analyse long-term results, molecular mechanisms of drug interaction, or their comparison with alternative treatments.
Magierska et al. [5] examined the exacerbation of atopic dermatitis in SARS-CoV-2, but did not analyse the mechanisms of the virus’s effect on the skin barrier, compare it with other triggering factors, or consider other factors (stress, temperature fluctuations), which limited the possibility of establishing a cause-and-effect relationship. Beck et al. [6] investigated the effects of Th2-mediated inflammation on skin barrier function, focusing on the role of IL-4, IL-5, and IL-13 in altering the expression of intercellular contact proteins. However, the study did not factor in the contribution of other key cytokines, such as IL-31 and TSLP, to allergen sensitisation. Furthermore, the researchers did not address the possibility of correcting skin barrier dysfunction by modifying the skin microbiome, which could expand therapeutic approaches to the treatment of atopic dermatitis. Jafarzadeh et al. [7] analysed the function of microRNA-155 in the regulation of the immune response, paying particular attention to its role in viral infections. At the same time, the issue of microRNA-155 involvement in the development of allergic skin reactions is still understudied. Specifically, the possibility of its modification as a potential therapeutic tool for the treatment of atopic dermatitis has not been considered.
Bacharier and Jackson [8] investigated the efficacy of biological therapy in patients with bronchial asthma, focusing on the mechanisms of Th2-mediated inflammation. However, the study did not analyse the crossover mechanisms between asthma and atopic dermatitis, which could help substantiate the use of biologics in patients with comorbid conditions. The lack of long-term observations of the efficacy of therapy in children also limited the practical significance of the findings. Eggel et al. [9] reviewed the prospects for the use of monoclonal antibodies in allergic diseases, including anti-IgE therapy. However, the researchers did not analyse the potential of combined therapeutic strategies, specifically the combination of IgE blockers with IL-4Rα or TSLP inhibitors, which could contribute to more effective control of inflammatory reactions in atopic dermatitis. Furthermore, the issue of the long-term effect of such drugs on the restoration of skin barrier function stays unresolved. McCraw et al. [10] investigated the relationship between IgE-mediated immune responses and the risk of developing cancer, emphasising the significance of IgE in the mechanisms of immune surveillance. At the same time, the study did not address the effects of anti-IgE therapy on cancer risks, which could be vital for assessing the safety of long-term treatment of patients with atopic dermatitis.
This work integrates immunological and molecular monitoring into a unified approach, unlike earlier studies that focused on individual skin allergy characteristics such as cytokine imbalance, microbiome alterations, or therapy effects. This method links systemic immune dysregulation to epidermal dysfunction and treatment outcomes by analysing Th2 inflammation, barrier protein expression, and microRNA regulation at many levels. This study shows that biomarkers including IgE, IL-4, IL-13, filaggrin, and miRNA profiles can improve diagnosis and prognosis, unlike earlier studies without molecular monitoring. Previous research rarely explored miRNAs’ therapeutic potential, but our analysis shows their promise as disease severity biomarkers and medication optimization targets. Thus, the work goes beyond descriptive relationships to propose a comprehensive model of how immunological and molecular surveillance might personalise allergic skin disease treatment.
Aim
The purpose of the present study was to determine the effectiveness of immunological and molecular monitoring to determine the methods of treatment of skin allergic diseases. The objectives of the study are to identify key biomarkers that reflect the state of the inflammatory process and skin barrier function, to establish correlations between changes in these indicators and clinical dynamics of patients, and to analyse the possibility of using molecular monitoring for personalised assessment of therapy efficacy. By addressing these research questions, this study proposes a more targeted approach to the diagnosis and treatment of allergic skin diseases, ultimately contributing to more effective and personalised therapeutic strategies.
Methods
This study was designed as a theoretical study aimed at analysing existing scientific data on immunological and molecular biomarkers involved in the pathogenesis of allergic skin diseases. Its purpose was to study the relationship between biomarkers, clinical manifestations, and therapeutic efficacy in order to identify mechanisms that can be used to monitor treatment outcomes. The study reviewed current concepts of Th2 inflammation, skin barrier dysfunction, and molecular mechanisms of immune regulation, with a particular focus on how these processes interact to influence disease progression and response to therapy.
Content analysis was used as the primary research method. This approach was used to systematise information on the role of central immunological mediators, such as IgE, IL-4, IL-5, IL-13, in the development of Th2 inflammation and to determine their contribution to B-cell activation and enhanced IgE production. Particular attention was paid to molecular markers of skin barrier dysfunction, including filaggrin, claudin-1, loricrin, as their reduced expression is a key factor in increased transepidermal water loss and sensitisation to allergens. Using this method, the study was able to trace the fundamental mechanisms underlying the progression of skin allergies and identify molecular targets for therapy.
The second methodological approach was comparative analysis. Its aim was to assess the relationships between the levels of specific biomarkers of inflammation and the severity of clinical manifestations of allergic skin diseases. Indicators such as IgE, IL-4, IL-13, soluble CD25, CCL17, CCL22, CCL26 were compared in different clinical scenarios to establish their diagnostic and prognostic value. In addition, comparative analysis was used to assess the impact of targeted therapies, including dupilumab, omalizumab, nemolizumab, on immune balance and molecular monitoring parameters. This allowed the study to determine the extent to which changes in biomarker profiles correspond to improved clinical outcomes and restoration of immune homeostasis.
A literature review was the third key method. This approach was used to collect, critically evaluate, and synthesise existing data on immunological and molecular monitoring in the context of skin allergies. The literature review allowed data from different sources to be integrated into a single system, providing a comprehensive understanding of how biomarkers reflect both the activity of the inflammatory process and the effectiveness of therapeutic interventions. This integration contributed to the improvement of methodological approaches to evaluating treatment effectiveness, emphasising the importance of multi-level monitoring strategies in the treatment of allergic skin diseases.
The combined use of these methods provided a comprehensive overview of molecular markers and their role in disease progression and treatment monitoring. The analysis provided insight into the relationships between cytokine imbalance, barrier protein expression abnormalities, and microRNA activity (particularly miRNA-155, miRNA-146a), highlighting their impact on the persistence of inflammation and the chronicity of allergic conditions. The results also demonstrated how targeted therapy affects these parameters, reducing systemic inflammation, restoring barrier protein expression, and normalising immune regulation. This methodological framework provided a systematic and detailed assessment of the available data and provided a sound basis for the use of immunological and molecular monitoring as a tool for improving therapeutic strategies for allergic skin diseases.
Results
Immunological mechanisms of skin allergic reactions
The immunological mechanisms of skin allergic reactions are based on the activation of Th2 lymphocytes, which play a central role in the development of inflammation characteristic of atopic dermatitis and other allergic dermatoses [11]. Allergens stimulate dendritic cells, which activate naive CD4+ cells and direct their differentiation into Th2 cells. In response to this process, Th2 cells produce the key proinflammatory cytokines IL-4, IL-5 and IL-13, which play a major role in the development of a pathological immune response. IL-4 and IL-13 stimulate B-lymphocytes to produce IgE, which leads to the activation of mast cells and basophils, causing the release of histamine and other inflammatory mediators.
IL-5 plays a critical role in the survival, proliferation, and activation of eosinophils, which supports the chronic inflammatory process in the skin [11]. Elevated levels of IL-5 promote the recruitment of eosinophils into tissues, where they release toxic granules that damage keratinocytes and disrupt the barrier function of the epidermis. Additionally, IL-4 and IL-13 alter the expression of genes involved in maintaining intercellular contacts, such as filaggrin, claudin-1, and loricrin, which contributes to increased epidermal permeability to allergens and pathogens. Activation of Th2 lymphocytes is accompanied by increased expression of activation markers, among which CD25, the α-chain of the IL-2 receptor, plays an essential role, ensuring the proliferation of Th2 cells and enhancing their immune response. An elevated level of CD25 expression on the surface of Th2 cells correlates with the severity of clinical manifestations and the degree of inflammatory response [12]. Apart from CD25, activation of Th2 lymphocytes is accompanied by increased expression of OX40 and ICOS, which enhances their interaction with B lymphocytes and promotes sustained IgE production.
Skin allergy illnesses depend on the balance between Th2 and Treg cells, which maintain immunological homeostasis and reduce inflammatory reactions [12]. Allergic dermatoses impair Treg cell activity and FoxP3, their key transcription factor for immunoregulation. Insufficient Treg cell activity impairs Th2 response regulation, perpetuating chronic inflammation and abnormal IgE production. Immunomodulatory treatment reduces Th2 inflammation and normalises regulatory mechanisms by restoring Th2-Treg cell balance. In skin allergic disorders, immune imbalance causes local inflammation and systemic alterations that worsen clinical symptoms. Th2 cell activation and increased IL-4, IL-5, and IL-13 cytokine production cause a chronic inflammatory process that compromises skin barrier function and the immune system. Decreased expression of intercellular contact proteins such as filaggrin, claudin-1, and loricrin increases epidermal permeability, which increases allergen sensitisation and penetration. Eosinophils, mastocytes, and basophils assist the inflammatory process in this cascading immunological response.
The skin microbiome regulates immune response and epidermal homeostasis [13]. Symbiotic bacteria modulate keratinocyte differentiation, AMP synthesis, and acid-base balance to produce skin barrier qualities. The connection between microbiota and immune cells, including γδ T cells, MAIT cells, and regulatory T cells, regulates inflammation and inhibits over-activation [14]. By activating Toll-like receptors (TLRs), producing too many proinflammatory cytokines, and changing the lipid barrier, this imbalance can cause inflammatory and allergic dermatoses such as atopic dermatitis. Figure 1 depicts the skin microbiomeimmune system connection and epidermal barrier function.
Figure 1
Role of the skin microbiome in the regulation of the immune response and barrier function of the epidermis. Source: compiled by the author based on Lee and Kim [14]
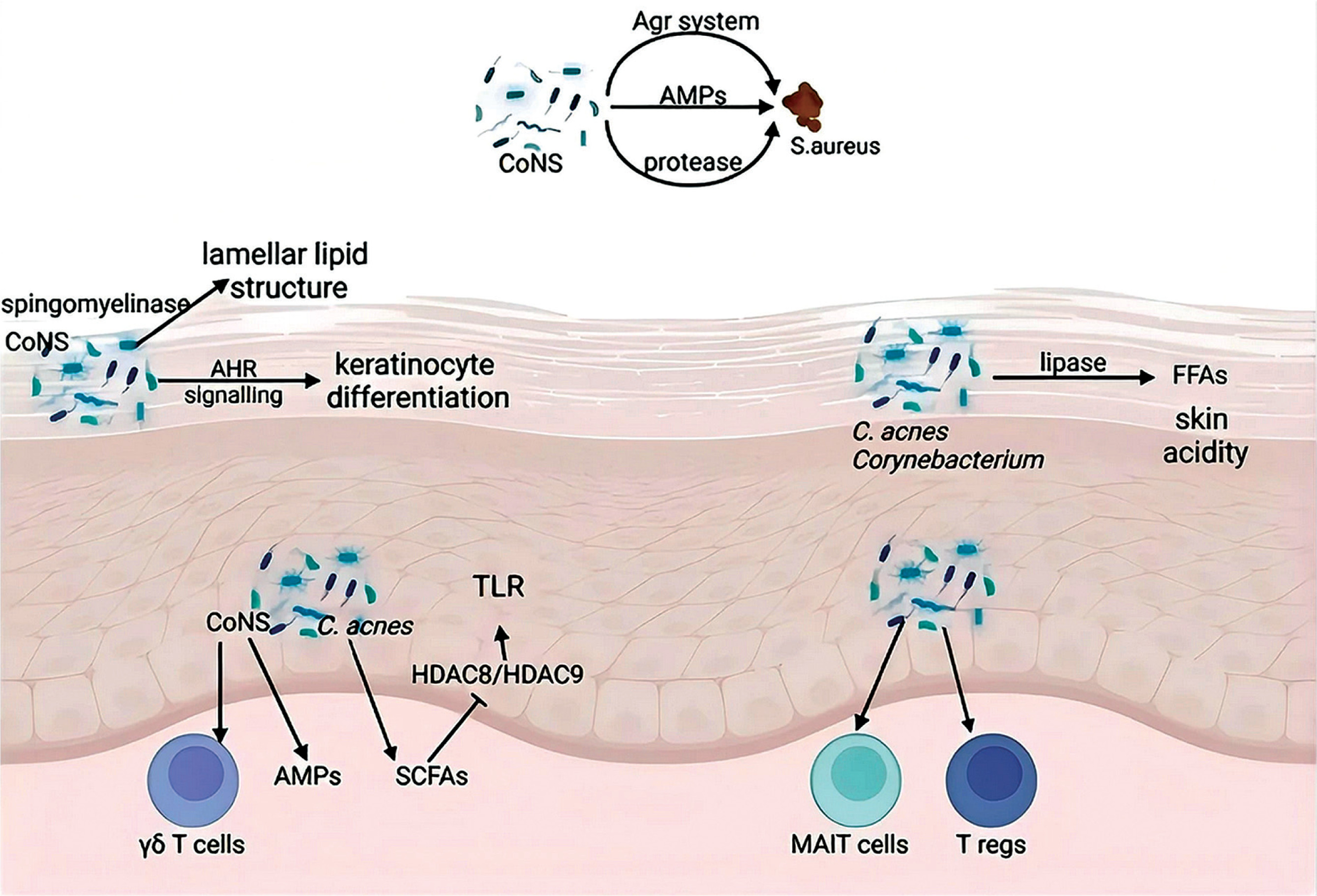
Figure 1 demonstrates the relationship of the skin microbiome to the immune system and the maintenance of the epidermal barrier function. Coagulase-negative staphylococci (CoNS) and Cutibacterium acnes play a vital role in regulating local immunity, specifically by stimulating antimicrobial peptides that prevent the colonisation of pathogenic bacteria such as Staphylococcus aureus. The effect of CoNS on the aryl hydrocarbon receptor (AHR) signalling pathway promotes keratinocyte differentiation and the development of the lamellar lipid structure of the epidermis. At the same time, C. acnes and Corynebacterium are involved in the metabolism of short-chain fatty acids (SCFAs) and free fatty acids (FFAs), which determines the acidity of the skin. The interaction of these bacteria with TLRs and the involvement of γδ T cells, MAIT cells, and regulatory T cells (Tregs) ensure the maintenance of immune balance [14]. Disruption of these processes can contribute to the development of chronic inflammation, which is one of the mechanisms of atopic dermatitis pathogenesis.
Local immune disorders in atopic dermatitis are closely related to systemic changes, including increased levels of IgE and cytokines in the blood [15]. Excessive production of IgE stimulates mast cell degranulation, which leads to the release of histamine and other proinflammatory mediators that cause intense itching, erythema, and infiltration of the skin by immune cells. Increased activation of IL-5-dependent mechanisms promotes the involvement of eosinophils in the skin tissue, where they secrete cytotoxic proteins that damage keratinocytes and increase inflammation. These processes form a vicious circle of immune activation, which ensures the chronicity of the pathological process. One of the key factors that determines the intensity of the inflammatory response is the ratio of Th2 to Treg cells. A decrease in the activity of Treg cells and their ability to control an excessive immune response contributes to the maintenance of the inflammatory process [12]. The loss of the regulatory effect of Treg cells leads to increased production of Th2-associated cytokines, which leads to further stimulation of B lymphocytes and IgE production. In patients with severe atopic dermatitis, not only local but also systemic dysregulation of this balance is observed, which is reflected in changes in the levels of biomarkers in the peripheral blood.
Impaired skin barrier function: molecular mechanisms
Molecular biomarkers play a key role in the pathogenesis of skin allergies, as they provide an opportunity to assess the structural and immunological changes that occur during the development of inflammation [16, 17]. These include proteins that maintain the integrity of the skin barrier, as well as regulatory molecules that control the activity of the inflammatory response. Impaired expression of these biomarkers is associated with the progression of the allergic process and the development of chronic symptoms. Biomarkers are inherent in both affected (lesional) and unaffected (non-lesional) skin areas, and they also reflect changes in the systemic circulation of patients with atopic dermatitis. These data emphasise the relationship between local immunological disorders and their systemic manifestations. Particular attention was focused on key molecules that played a significant role in the pathogenesis of the disease, making them promising targets for therapeutic and diagnostic monitoring [18].
Among the characteristic biomarkers specific to affected and unaffected skin areas in atopic dermatitis are CCL22/MDC, IL-13, IL-18, and IL-22, which are detected in unaffected areas (non-lesional AD). Their presence reflects the basic activation of the immune system [19]. These molecules are indicative of a systemic inflammatory process even in the absence of clinical manifestations, which suggests subclinical activity of atopic dermatitis and a potential risk of exacerbation. The close interaction between local and systemic immune processes in atopic dermatitis confirms the need for a comprehensive approach to biomarker analysis, including the assessment of both skin and peripheral blood parameters. Such an approach contributes to the development of more accurate diagnostic algorithms and therapeutic strategies to control the inflammatory process and reduce the severity of symptoms in patients. In the context of skin allergy therapy, molecular biomarkers play a significant role in determining the effectiveness of treatment and predicting the course of the disease. The study of the expression of filaggrin, claudin-1, loricrin proteins and microRNA levels (miRNA-155, miRNA-146a) allows to assess the functional state of the skin barrier and the activity of the inflammatory process [20, 21]. Monitoring of these parameters provides a personalised approach to treatment, which considers the specifics of the pathogenesis in each patient.
Table 1 summarises the principal molecular biomarkers used to assess the therapeutic response in patients with skin allergies. The data presented reflect their role in the development of the pathological process, clinical significance, and dynamic changes under the influence of therapy. The summarised information contributes to a better understanding of the mechanisms of allergic dermatoses and the possibilities of their correction by targeting key pathophysiological processes.
Table 1
Key molecular biomarkers for assessing therapeutic response in skin allergies
Table 1 summarised the role of skin barrier proteins (filaggrin, claudin-1, loricrin) in the pathogenesis of skin allergies. The lack of their expression is associated with an impaired barrier function of the epidermis, which contributes to uncontrolled penetration of allergens and enhances the inflammatory response. The restoration of these proteins after therapy indicates an improvement in the structural integrity of the skin, which confirms the effectiveness of the treatment.
The regulatory role of microRNAs (miRNA-155, miRNA-146a) in the inflammatory process was also presented in Table 1. An elevated level of miRNA-155 correlates with the activity of allergic inflammation, while miRNA-146a provides control over these processes, acting as a negative regulator of the inflammatory response [22, 23]. Tracking changes in the levels of these biomarkers allows to assess the efficacy of therapy and potential treatment resistance. Levels of IgE and Th2-associated cytokines (IL-4, IL-13) are still key indicators of systemic inflammation [24–26]. Their reduction after therapy indicates effective immunomodulation and a decrease in the activity of Th2-dependent inflammation. These parameters, in combination with other molecular parameters, are used to monitor the efficacy of treatment and correct therapeutic tactics.
Inflammatory biomarkers and their clinical significance
Inflammatory biomarkers play a key role in the pathogenesis of skin allergic diseases, as they allow to assess the intensity of the inflammatory response, immune cell activity, and the effectiveness of therapy [23]. Their dynamics correlate with the severity of clinical manifestations, making them essential indicators in the development of personalised treatment approaches. Table 2 shows the key biomarkers of the inflammatory process, their functional significance, and the specifics of changes in patients with skin allergies.
Table 2
Inflammatory biomarkers and their clinical significance
Allergic inflammation is marked by IgE, which contributes to rapid hypersensitivity [27]. Higher levels indicate allergic activation and worsen clinical symptoms. Anti-IgE treatment reduces inflammation and allergic dermatitis symptoms. In addition to IgE, IL-4 and IL-13 activate Th2 inflammation, which increases IgE production and affects epidermal barrier function. IL-4Rα inhibition reduces these cytokines, confirming their crucial involvement in allergic responses. IL-5 is the main factor that helps eosinophils survive and activate, causing chronic inflammation [27]. High peripheral blood IL-5 levels indicate disease severity, especially in severe atopic dermatitis. IL-5 antagonists lower blood and tissue eosinophils, reducing inflammation. IL-13, which regulates epidermal barrier permeability, is crucial to allergen sensitisation. The decrease in its level after targeted therapy suggests improved skin barrier function. Besides cytokines, chemokines such as CCL17, CCL22, and CCL26 contribute to inflammation [28]. They recruit Th2 cells and eosinophils to the inflammation site, perpetuating persistent inflammation. Increased peripheral blood chemokine levels correspond with illness severity and anticipate allergy process activity. After targeted therapy, CCL17, CCL22, and CCL26 levels drop, indicating inflammatory response reduction. A complete biomarker study can measure the inflammatory process and therapy efficacy.
Effects of therapy on molecular and immunological parameters
The development of skin allergic diseases is accompanied by complex immunological and molecular disorders, which necessitates the use of comprehensive monitoring methods to assess the efficacy of therapy. Immunological analysis provides information on the level of systemic inflammation, Th2 lymphocyte activity, concentration of IgE, and pro-inflammatory cytokines (IL-4, IL-5, IL-13), which determine the intensity of the allergic response. However, these indicators do not reflect changes in the skin structure, which limits their prognostic value. Molecular monitoring allows to assess the state of the skin barrier and intracellular mechanisms that affect the development of the pathological process [27]. Analysis of the expression of genes encoding proteins of barrier function (filaggrin, claudin-1, loricrin), as well as the levels of regulatory microRNAs (miRNA-155, miRNA-146a) provides additional information on the mechanisms of disease development. The integration of these methods with modern genetic technologies, such as next-generation sequencing (NGS) and genome editing (CRISPR-Cas9), opens new opportunities for personalised therapy.
Table 3 summarises the key immunological and molecular monitoring methods employed to assess the condition of patients with skin allergies. It described their clinical significance and prospects for use in diagnosis and treatment. Particular attention is paid to combined biomarker panels, non-invasive monitoring technologies, and promising genetic methods that could expand the possibilities of personalised medicine.
Table 3
Prospects for combined immunological and molecular monitoring in skin allergies
The integration of immunological and molecular monitoring has improved approaches to the treatment of skin allergies, providing a multilevel assessment of pathophysiological processes [29, 30]. Combining the analysis of immunological parameters, such as the level of IgE and cytokines (IL-4, IL-13), with molecular characteristics, including the expression of skin barrier genes (filaggrin, claudin-1) and microRNA profile (miRNA-155, miRNA-146a), helped to gain a detailed understanding of the mechanisms of disease development. This contributed to a personalised approach to therapy and determination of treatment efficacy according to individual patient characteristics. IgE levels were still one of the key indicators of systemic inflammation, reflecting the severity of the allergic response. Therewith, the cytokine profile helped to assess the activity of Th2-dependent inflammation, which was significant for the choice of targeted therapy. For instance, a decrease in IL-4 and IL-13 levels after treatment indicated the efficacy of the drugs used and the achievement of control over inflammatory processes. Molecular monitoring, based on the analysis of the expression of skin barrier genes such as filaggrin and claudin-1, demonstrated high efficacy in predicting the recovery of the skin structure. The determination of these indicators complemented the immunological analysis, forming a holistic picture of the disease course and treatment effectiveness. The restoration of the expression of these genes was considered as one of the predictors of sustained remission and stabilisation of the skin condition after therapy.
NGS methods identified genetic variants that impacted skin allergy risk and severity [31]. Individual sensitivity to targeted immunotherapy was determined by genetic variant analysis. This enabled personalisation of treatment to boost efficacy. CRISPR-Cas9 genome editing enabled skin barrier and immune response mutation correction [32]. These technologies can establish new therapeutic techniques to regulate symptoms and correct illness aetiology, according to preliminary investigations. Regular monitoring of the patient’s status using biomarkers in saliva, perspiration, or epidermal samples [33] reduced discomfort and the need for intrusive treatments. Such approaches provided dynamic data on illness progression and treatment efficacy, increasing clinician surveillance. Multi-level diagnostic panels for skin allergies were developed using immunological and molecular monitoring. Such technologies have improved therapy techniques, predicted relapse risk, and accelerated treatment adjustments.
After skin allergy disorders developed, pro-inflammatory and regulatory immune response systems were imbalanced, causing chronic inflammation and epidermal alterations. Th2 lymphocyte activation, IgE, IL-4, and IL-13 levels rose, causing immune system hyperactivity and skin barrier dysfunction. The disruption to epidermal structures decreased filaggrin and claudin-1, which enhanced transepidermal water loss and allergen sensitisation. Normalizing these parameters is one of the main therapy goals to restore skin barrier function and reduce systemic inflammation. Skin allergies were treated by targeting important pathophysiological pathways. A reduction in Th2 inflammation was accomplished by suppressing IL-4, IL-13, IL-31 signalling pathways and limiting FcεRI-dependent mast cell activation. Anti-IgE medicines lowered basophil and mastocyte degranulation, reducing inflammatory mediators and pruritus severity. Skin barrier molecular indicators were also affected, restoring epidermis structure. Table 4 summarises the main treatment techniques to rectify these processes, including their efficacy and consequences on disease pathogenetics/pathogenesis.
Table 4
Therapeutic approaches to the correction of inflammatory and barrier disorders in skin allergies
[i] Source: compiled by the author based on Livshits and Kalinkovich [34].
The results of the analysis of therapeutic strategies revealed the efficacy of a combined approach that included simultaneous immunomodulation and restoration of the skin barrier function. The use of dupilumab reduced the levels of IL-4 and IL-13, which contributed to the normalisation of the ratio of Th2 and Treg cells and the reduction of immune response hyperactivity. In addition, inhibition of IL-31 was significant for controlling pruritus and reducing the intensity of the inflammatory process. Anti-IgE therapy reduced the sensitivity of mastocytes and basophils to stimulation, which prevented the excessive release of inflammatory mediators, while the use of JAK inhibitors blocked the transmission of inflammatory signals through cytokine receptors. Therapeutic approaches aimed at restoring the skin barrier function included normalising the expression of intercellular contact proteins (claudin-1, filaggrin), which helped to reduce epidermal permeability and transepidermal water loss [34]. The use of molecularly targeted therapies, such as modification of microRNA levels (miRNA-155, miRNA-146a), helped to regulate the activity of inflammatory signals and compensatory mechanisms of the immune response. The study found that the effect on microRNAs contributed to the stabilisation of the inflammatory process and the maintenance of immune homeostasis, making them a promising target for the treatment of chronic skin allergies.
The most successful treatment for atopic dermatitis and other skin allergies was targeted immunomodulation and epidermal normalisation, according to a comprehensive review. Controlling inflammation, lowering IgE, blocking IL-4 and IL-13, and repairing intercellular connections improved skin condition and reduced exacerbations. To tailor treatment to the diseased process, the proposed methods assessed inflammatory mediators, skin barrier biomarkers, and immune regulatory mechanisms. The study demonstrated that Th2 cell activation promotes excessive IgE production and eosinophil involvement in cutaneous allergy responses. The cytokines IL-4, IL-5, and IL-13 influence systemic and local immune responses, compromising epidermal barrier function. Lack of Treg cell activity and an imbalance between proinflammatory and regulatory processes perpetuate inflammation.
The skin microbiome regulates inflammation and maintains the epidermis structure. TLR activation and pro-inflammatory mediator synthesis increase with commensal microorganism alterations in dysbiosis. Microbial homeostasis disruption accelerates skin pathology, increasing permeability and allergen sensitisation. In skin allergy sufferers, biomarkers showed decreased expression of intercellular contact proteins (filaggrin, claudin-1, loricrin) and higher proinflammatory cytokines and IgE. Targeted treatment reduces Th2 inflammation and normalises skin barrier function. Dupilumab and omalizumab decreased IL-4, IL-13, and IgE levels, confirming their effect on skin allergy pathophysiology.
Discussion
The results confirmed the importance of immunological and molecular monitoring for skin allergy treatment success. IgE, IL-4, and IL-13 levels rose with Th2 cell activity and clinical severity, according to the study. According to Dubin et al. [35], IL-4, IL-13, and IL-31 contribute to atopic dermatitis. The researchers observed that IL-31 directly modulated pruritus and enhanced inflammatory response, supporting the systemic nature of Th2 inflammation. Treatment to decrease these cytokines stabilised the epidermal barrier and restored claudin-1 and filaggrin expression, proving its efficacy. The epidermis became more permeable to allergens when intercellular contact proteins (claudin-1, filaggrin) decreased due to epidermal barrier dysfunction. Beck et al. [6] observed that Th2 cytokines maintained chronic inflammation and directly impacted intercellular contact protein expression. It was also shown that epidermal barrier disturbance encouraged Staphylococcus aureus colonization and infectious consequences. Dupilumab therapy improved barrier function, inflammation, and claudin-1 expression, confirming this mechanism. IL-4 and IL-13 activated innate immunity and Th2-mediated pathways. Donetti et al. [36] found that IL-4 and IL-13 increased the innate inflammatory response by modulating TLR2, TLR4. They observed that these cytokines had no effect on tight junctions but maintained chronic inflammation via TLR-dependent mechanisms. The present findings validated these findings, as patients with significant Th2 inflammation had increased TLR signalling pathway activity, suggesting a holistic therapy that corrects both adaptive and innate immune responses/which suggests that a holistic therapy can correct both adaptive and innate immune responses.
Katsarou et al. [37] examined the mechanisms of tight junction dysfunction in atopic dermatitis. The researchers reported that a decrease in the level of claudin-1 and claudin-23 contributes to increased epidermal permeability and increases the risk of allergen sensitisation. The analysis of the obtained results confirmed these findings, as the level of claudin-1 returned to normal after treatment, indicating the restoration of the skin’s barrier function. The relevance of these findings confirms the key role of intercellular contact disorders in the development of allergic skin diseases and emphasises the significance of their restoration as one of the principal therapeutic tasks. Dong et al. [38] also confirmed this relationship, proposing the hypothesis of an ‘inflammatory cycle’ wherein a violation of the skin barrier function served as a catalyst for the immune response. The researchers discovered that damage to filaggrin and claudin-1 not only reflects the intensity of the inflammatory process but also contributes to its maintenance, which is consistent with the present findings. This confirms the significance of therapeutic strategies aimed at restoring the structure of the epidermis, specifically when using dupilumab.
Namrata and Bai [39] also confirmed the role of impaired intercellular contacts in the pathogenesis of skin allergies. The researchers found that dysfunction of tight junctions contributes to an increase in TEWL and sensitisation to allergens. They reported that a decrease in the level of claudin-1 correlates with the severity of clinical manifestations of atopic dermatitis, which is consistent with the present findings. Restoration of claudin-1 levels after therapy was accompanied by a decrease in epidermal permeability, which confirms the effectiveness of therapeutic approaches aimed at reducing Th2 inflammation and stabilising the skin barrier. The analysis of the mechanisms of correction of skin barrier disorders confirmed the prospects of using natural immunosuppressors. Guo et al. [40] demonstrated that Momordin Ic helps to normalise claudin-1 levels and reduce inflammation through MyD88/NLRP3-mediated mechanisms. The researchers found that Momordin Ic improves filaggrin expression, reduces IL-33 and IL-4 levels, which positively affects the skin barrier function. The findings confirmed the significance of targeted effects on the molecular mechanisms of epidermal dysfunction and highlighted the prospects for the use of natural compounds in the treatment of skin allergies.
Atopic dermatitis inflammatory regulation/Inflammatory regulation of atopic dermatitis is closely linked to microRNA activity. According to Săsăran et al. [41], miRNA-155 and miRNA-146a regulate NF-κB-mediated inflammatory pathways. Researchers showed that miRNA-155 stimulates pro-inflammatory processes and miRNA-146a reduces excessive immune responses. The present study demonstrated higher miRNA-155 levels in atopic dermatitis patients, confirming its role in Th2 inflammation. This emphasises the importance of managing miRNA-155 levels in severe cases and opens the door to microRNA-based therapies. Kim et al. [42] discovered that miRNA-154-5p activated NF-κB-dependent signalling pathways by mediating allergic inflammation via the MCP1 axis. Research indicates that miRNA-154-5p increases Th2 inflammation by boosting MCP1 levels, which activates NF-κB and promotes proinflammatory cytokines. This study supports previous findings that NF-κB-dependent signalling pathways are crucial for sustaining Th2 inflammation in skin allergies. IL-4 and IL-13 expression rose with miRNA-154-5p, demonstrating its role in maintaining atopic dermatitis’ inflammatory environment. This supports targeted miRNA-154-5p suppression as a disease-severity treatment. Hammad et al. [43] confirmed miRNA-155 as an allergy inflammatory biomarker. Higher miRNA-155 levels were linked to more severe allergic rhinitis and higher IL-4 levels. The researchers found that miRNA-155 regulated Th2-associated inflammation and might monitor treatment response. Since miRNA-155 also plays an equivalent role in atopic dermatitis, these findings are congruent. Increased miRNA-155 levels are linked with clinical severity and higher SCORAD scores, validating its role as a disease activity predictor. This highlights the necessity to study miRNA-155 as a marker for treating severe skin allergies individually. Tontini and Bulfone-Paus [44] studied IgE-dependent mast cell activation pathways, examining IL-4Rα and TSLP inhibitors as novel treatments. The study found that IL-4Rα inhibition lowered Th2 inflammation and IgE production, making it an attractive therapeutic target. Targeted suppression of IgE-dependent inflammation in atopic dermatitis was verified by these findings. Reducing IgE levels and blocking IL-4Rα led to reduced inflammatory activity, improved skin barrier function, and reduced illness symptoms. Combining anti-IgE medication with IL-4Rα blockers may be effective in treating severe skin allergic responses.
The analysis of the role of IL-13 in the development of the inflammatory process confirmed its significance in Th2-associated inflammation, which was accompanied by increased IgE expression and impaired skin barrier function. The study found that a decrease in IL-13 levels after the use of targeted therapy correlated with the normalisation of the expression of intercellular contact proteins (filaggrin, claudin-1, loricrin) and a decrease in epidermal permeability to allergens. Tubau and Puig [45] also confirmed the key role of IL-13 in the development of Th2 inflammation in atopic dermatitis, but the researchers did not analyse the interaction of IL-13 with other mediators such as IL-4, IL-31, and TSLP. The results confirmed that IL-13 not only mediated the inflammatory response but also played a notable role in the disruption of epidermal barrier functions, which substantiates its significance as a therapeutic target.
The study found that IL-13 was involved in the development of itching through the activation of neurosensory mechanisms, which was accompanied by increased expression of sensory receptors. The study confirmed that inhibition of IL-13 reduced itching and normalised the activation of skin nerve endings. Napolitano et al. [46] also confirmed that IL-13 affected the skin barrier function and played a role in the regulation of pruritus through neurosensory mechanisms. However, the cited study did not address the interaction of IL-13 with TLRs, which are involved in the triggering of innate immunity. The results obtained are consistent with previous studies, adding to the understanding of the mechanisms of IL-13-mediated effects on sensory receptors and maintenance of the inflammatory process.
Through macrophage and mastocyte activation, TLR-dependent mechanisms maintained chronic inflammation in allergic dermatitis, according to this study. The elevated TLR-mediated signalling response increased proinflammatory cytokines, worsening Th2 inflammation. Yamaguchi et al. [47] also found TLR-dependent innate immune activation in allergic contact dermatitis. The present study did not compare allergic contact and atopic dermatitis, limiting extrapolation. The findings showed that TLR-mediated mechanisms were crucial to atopic dermatitis’ chronic inflammation and maintenance. The significance of miRNA-155 and miRNA-146a in controlling NF-κB-dependent signalling pathways supports the role of microRNAs in regulating skin allergy inflammation. High miRNA-155 levels corresponded with severe clinical symptoms, while miRNA-146a reduced excessive immune response. Khosrojerdi et al. [48] demonstrated that miRNA-155 and miRNA-146a affect inflammation, but they did not explore the prospect of targeting these molecules to restore the skin barrier function. The findings support earlier research and suggest that miRNA-155 may be an indicator of illness severity and a prospective therapeutic target.
The present investigation validated the role of Th2-mediated processes in atopic dermatitis, including elevated IL-13, IL-4, and IgE activity and skin barrier dysfunction. The study demonstrated that targeted therapy reduced epidermal allergen permeability by normalising filaggrin, claudin-1, and loricrin levels. It was confirmed that TLR-dependent mechanisms activate macrophages and mastocytes to maintain inflammation. The study revealed the importance of miRNA-155 and miRNA-146a in NF-κB-mediated signalling pathways, highlighting their potential as disease severity biomarkers and therapeutic targets. Taken together, these findings extend previous research by demonstrating that the integration of immunological and molecular biomarkers provides a more comprehensive assessment of the pathogenesis of skin allergy and response to treatment than approaches that investigate these mechanisms separately. This is a unique contribution of this study to the development of personalised dermatological therapy.
Conclusions
This study demonstrated that a combined immunological and molecular approach to monitoring provides a comprehensive and reliable assessment of the pathogenesis of skin allergies and the effectiveness of treatment. The analysis confirmed that elevated levels of IgE, IL-4, and IL-13, as well as an imbalance of Th2 and Treg cells, are major factors in chronic inflammation and correlate with disease severity. These immune abnormalities were accompanied by reduced expression of barrier proteins such as filaggrin and claudin-1, leading to increased epidermal permeability and sensitisation to allergens. Elevated levels of miRNA-155 further reflected the persistence of inflammatory activity and the severity of clinical manifestations.
Evaluation of targeted therapies showed that dupilumab and omalizumab effectively reduced IgE, IL-4, and IL-13 levels, normalised barrier protein expression, and improved both epidermal integrity and clinical outcomes. These results confirm that therapies that inhibit the IL-4/IL-13 pathways not only control inflammation but also restore the structural basis of skin homeostasis, confirming their role as key agents in the long-term treatment of the disease.
The integration of next-generation sequencing and microRNA analysis has shown promise for identifying individual immune profiles and predicting treatment resistance, highlighting the potential for personalised therapeutic strategies. The development of multiplex diagnostic panels combining immunological, molecular, and epigenetic markers will improve diagnostic accuracy and aid in the selection of individualised interventions in clinical practice.
However, the study was limited by its theoretical design and reliance on data taken from the literature, which may not fully reflect patient variability or long-term therapeutic outcomes. Therefore, experimental and long-term clinical studies are needed to confirm these findings and enhance their translational value. Future directions include investigating genome editing techniques, such as CRISPR-Cas9, to eliminate mutations affecting skin barrier function and improving non-invasive monitoring of biomarkers from saliva, sweat, or epidermal samples. These approaches have the potential to significantly improve diagnostic accuracy, patient comfort, and long-term treatment outcomes.







