
Introduction
Over the past decade, hybrid and gel manicures have gained immense popularity [1]. The attractiveness lies in their resilience and visual appeal as they offer a long-lasting glossy finish [2]. Hybrid and gel manicures share some similarities. Hybrid manicure combines traditional nail polish with gel-like properties while gel manicure uses a fully gel-based polish [1]. Both need to be cured under LED or UV light [1]. Gel manicure requires curing between each layer [3], resulting in a thicker, more resilient coating. Thus, hybrid polishes are generally thinner and easier to remove. The manicures can either be performed at a beauty parlour or at home using kits for domestic use [1]. The rising prevalence of these manicure techniques has raised growing concern regarding their potential health implications and remains a topic of scientific and public debate.
Aim
The study aims to provide a comprehensive understanding of the safety, health risks, and implications of hybrid and gel manicures, offering valuable insights for consumers and healthcare providers.
Methods
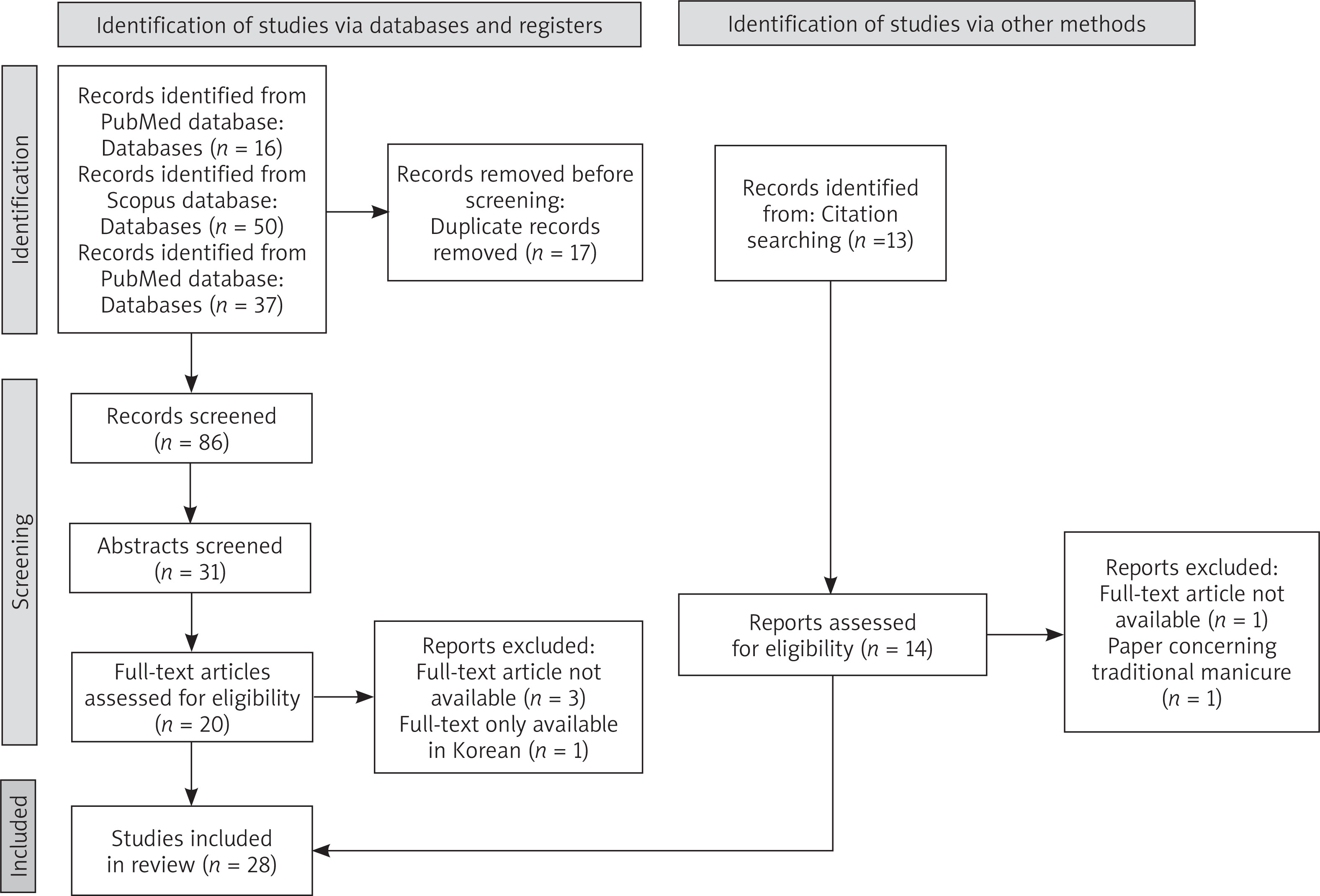
A literature search was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The search was conducted in the PubMed, Scopus and Google Scholar databases using the following search strategy: (“hybrid manicure” OR “gel polish*” OR “UV cure* nails”) NOT (“acrylic nails” OR “artificial nails”). The search was limited to articles published in Polish and English from January 2011 to December 2024. A flow diagram of the systematic review is shown in Figure 1, adhering to the PRISMA model.
Studies that examined the following topics were included in the study: the physical and structural changes occurring in nails because of the prolonged use of hybrid and gel manicures, allergic and non-allergic diseases linked to the use of hybrid and gel manicures, cancer risk associated with repeated UV light exposure and the implications of hybrid and gel manicures on hand hygiene, particularly in the context of the healthcare-associated infections.
All articles were screened based on the title (n = 86) and then abstracts (n = 31). Finally, the compliance between full-text articles and the topic of the review was assessed. Additionally, studies identified from citation searching were included in the study (n = 12) after the same screening process.
Results and discussion
Changes in nails as a result of hybrid and gel manicure use
In the context of hybrid and gel manicures, changes in the nail can be caused by the application, nail polish itself and the process of removal. Batory et al. [4] used scanning electron microscopy to establish that mechanical removal of manicure by a drill machine or nail file is the most destructive procedure for nails. A phenomenon connected with those procedures is the worn-down nail syndrome, characterized by thinning of the distal nail plate.
An online survey with over two thousand respondents found that 84.5% of gel manicure users report side-effects, 21.2% during and 75.2% after removing gel nail polish. 55.9% of respondents who used gel nail polish kits and 18.1% of respondents whose manicure was performed by a professional, noticed changes in the nail plate after removing the manicure. This means that while the application technique may have a significant impact on the frequency of these side-effects, those can also be present following a professional service. More than half of respondents experienced subjective symptoms such as itching, burning sensation or pain. The most frequently reported changes were decreased toughness (30.3%), splitting (24.7%) and white spots on the nail plates (8.5%) [5]. Those results are consistent with another questionnaire which established that the most common complaints of manicure users concern nail brittleness and splitting [4].
Physiologically, the thickness of nails increases with age and ranges from 0.5 to 0.7 mm [6]. However, the application of manicure can lead to nail thinning. Borowczyk and Głowacki [6] investigated the impact of UV varnishes on the content of cysteine and methionine which are the most important sulfur amino acids that build keratins in the nail plate. When the number of disulfide bridges in the structure of keratins decreases, the nails become more brittle and breakable, and thus more susceptible to damage. They found that after 6 months of hybrid manicure use, the average amount of cysteine was 22.1% lower while the content of methionine was 36.5% lower. This corresponds directly with nail thinning which changed from 0.50 ±0.12 mm before to 0.46 ±0.12 mm after the use of the hybrid manicure. This was observed along with another common manifestation of keratin degradation such as nail vitiligo. It seems that pH of the nail plate is also affected by hybrid and gel manicure. It increases and therefore may predispose to various infections [4, 7].
Apart from the aforementioned changes, a series of case reports presented 5 patients with severe pseudoleukonychia as a result of superficial nail plate desquamation and severe onychoschizia lamellina [8]. One case report described a 63-year-old Korean woman who had gel manicure applied once a week for 5 months. The patient removed the manicure by soaking her nails in acetone for 15–30 min. Two months after the first manicure she developed a pincer nail deformity of both thumbnails accompanied by yellowish chromonychia [9].
Allergic reactions to the ingredients of hybrid and gel varnishes
1–3% of the population is allergic to nail products’ ingredients [1]. Acrylate monomers, known for their sensitizing properties, are one of the components of hybrid and gel nail polishes. If used correctly the acrylate monomers undergo polymerization under the influence of UV light, which transforms them into polymers that have no sensitizing properties. However, low-power UV lamps may prevent acrylate monomers from complete polymerization leading to the development of acrylate allergies which are even more likely if the outer layer of the nail plate is damaged and cuticles are removed [10]. The most common skin lesions connected with allergic contact dermatitis caused by acrylates are oedema, reddening and fissures of the fingertips and nail dystrophy [1].
A series of case studies by Opalińska et al. [10] presented 8 patients with hand eczema along with nail changes that included: inflammation within the nail bed and nail matrix (n = 8), onycholysis (n = 8), subungual hyperkeratosis (n = 8), splinter haemorrhages (n = 2) and eczematous finger pulp fissuring (n = 2). All patients were diagnosed with allergic contact dermatitis induced by hybrid manicure. The exposure period to acrylates ranged from 1 month to 3 years and patients with longer exposure developed more severe changes. Type IV allergic reaction was suspected. After hybrid manicure removal and applied treatment, all patients recovered. In all cases manicure was performed using non-professional UV lamps. It is particularly dangerous to use UV lamps with a power below 36 watts. The risk of sensitization and recurring dermatitis can be reduced by using suitable light sources, ensuring complete curing of acrylic monomers, and preventing skin contact with uncured varnish.
A typical patient with allergic contact dermatitis caused by acrylates contained in nail varnishes is a young, non-atopic woman working as a beautician, suffering from dermatitis of the hands and face. Gatica-Ortega et al. [3] found that for beauticians the mean time before the development of allergic contact dermatitis symptoms is 10.55 months from the first exposure to hybrid varnishes. Occupational allergic contact dermatitis can be prevented by minimizing exposure to allergens by using personal protective equipment. Appropriate gloves should be changed regularly and removed properly to prevent skin contamination. Regular application of emollients may also be helpful [1].
Allergens may be transported via contaminated tools, hands or through evaporation of acrylates, which may explain both the occurrence of respiratory symptoms and skin lesions in other locations [1]. An example of such case is a 49-year-old woman who presented with cheilitis and lip oedema after 3–4 months of getting UV-curable manicure. While the cheilitis was worsening, the lip oedema remained constant, with no relationship with the manicure sessions. The patient admitted touching her lips frequently. A patch test was performed and the patient was diagnosed with allergic contact dermatitis. Removal of the varnish resulted in rapid resolution of the cheilitis and slow recovery of the lip oedema [11].
Non-allergic diseases associated with hybrid and gel manicure
Paronychia is a risk especially associated with manicure application which is accompanied by reduction or removal of the cuticle [12]. The most common microbes that have been isolated in beauty salons from nail care tools are Candida spp., Penicillium spp., Micrococcus spp., and Staphylococcus spp. [13].
A less common complaint is pterygium inversum unguis (PIU), characterized by the abnormal adherence of the hyponychium to the ventral surface of the nail plate. There are case reports of PIU as an adverse outcome of gel manicure, however it is unclear whether PIU is related to chemicals present in the nail polish or to the application and/or removal process. Some hypothesize that LED or LED-activated photoinitiators may be more likely to induce PIU as compared to UVA. A retrospective and prospective case series reported that in 15 out of the 17 patients with PIU connected to gel manicure, the condition was reversible upon removal of the varnish [2].
Potential cancer risk associated with UV-light exposure
There is a debate on the safety of using UV lamps in the context of potential cancerogenic effects. Although rare, there are reports of squamous cell carcinoma (SCC) of the nail unit [14] and dorsal hands [15, 16] which consider UV lamps as a potential triggering factor. Ordońez et al. [14] reported the case of a 26-year-old female patient who presented with changes in the colour of her nail and detachment of the nail plate. A biopsy of the nail matrix enabled the diagnosis of SCC in situ. The patient had been continuously exposed to UV lamps twice a month for 2 years. The authors argue that while a declared relationship between the use of UV lamps and the development of SCC cannot be asserted, it is suggestive due to the patient’s young age and no other risk factors, with the presence of tumour in an area directly exposed to UV lamps. There is however a study which claims that healthy fingernails can protect the subungual skin against potentially harmful UV light. Namely, Stern et al. [17] performed a study on cadaver fingernails which provided insight into the extent to which UV-A and UV-B radiation can penetrate the human fingernail plates. It turns out that UV-B is completely blocked, whilst the mean penetration of UV-A through the fingernails is 1.65%.
The controversies surrounding the use of UV lamps were further fuelled by an article published by Zhivagui et al. [18] which concluded that radiation emitted by UV lamps used for curing hybrid and gel manicure can damage DNA and permanently engrave mutations on the genomes of primary mouse embryonic fibroblasts, human foreskin fibroblasts, and human epidermal keratinocytes. However, the study was based on in vitro cell line models which lack the protective cornified layer of the epidermis. Furthermore, in vitro cell lines accumulate non-physiological background mutations which would be different in normal human skin. The authors state that their report does not provide direct evidence for an increased cancer risk in human beings. Another study performed on keratinocyte cell lines investigated the viability of human keratinocytes irradiated by a UV lamp led by Słabicka-Jakubczyk et al. [19], came up with a conclusion that the typical manicure exposure time does not significantly affect keratinocyte viability, which could increase the risk of developing skin cancers.
A study by Aguilera et al. [20] compared the emission of UVA- and LED-lamps to sunlight exposures to assess the carcinogenic potential. The conclusion was that the common use of lamps is equivalent to sunlight exposure of 3–5 min in the central hours of the day. Therefore, it represents a very low carcinogenic potential. In a different study, Diffey [21] came to a similar conclusion by creating a mathematical model that enabled the estimation of the number of women who would need to be exposed to UVA nail lamps for one woman to develop SCC on the dorsum of hands. His estimation was that tens or hundreds of thousands of women would need to use a UVA nail lamp regularly for one to go on to develop SCC.
Many authors recommend using protective measures to further minimize the potential cancer risk. Słabicka-Jakubczyk et al. [19] found that sunscreen cream SPF50 significantly increases the viability of keratinocytes during UV lamp radiation, so sunscreen application 30 min before UV lamp use is advised. Other authors also recommend the use of fingerless manicure gloves [15, 20, 21].
Hand hygiene efficacy in hybrid and gel manicure
According to the practice recommendation by Glowicz et al. [22], healthcare workers should maintain short, natural fingernails which should not extend past the fingertip. Prohibitions against nail polish are at the discretion of the infection prevention program, except among healthcare workers who interact with the sterile field who are prohibited from any kind of nail polish. The recommendations rate the quality of evidence as high which faced criticism from authors whose research suggests that some types of nail polish do not interfere with the effectiveness of hand hygiene [23]. The summary of literature search concerning hybrid and gel nail varnishes in the context of potential impact on the rate of healthcare-associated infections is presented in Table 1.
Table 1
Summary of studies investigating the impact of hybrid manicure on hand hygiene included in the systematic review
| Authors and year | Study design | Population | Sample size | Outcomes |
|---|---|---|---|---|
| Wałaszek et al. (2018) [24] | Pilot study | Healthcare workers (nurses and midwives) | 99 analyzed, 15 hybrid manicure | The presence of potentially pathogenic microorganisms was correlated with nail length, and the presence of UV-cured nail polish. |
| Wałaszek et al. (2021) [25] | Controlled study | Healthcare workers (nurses) | 188 analyzed, 80 hybrid manicure, 27 hybrid varnish applied to a plate reinforced/extended with gel | The risk of growing a pathogenic microorganism after hand disinfection due to nails coated with a hybrid varnish was similar to that of natural nails. Modelling and/or extending the nail plate with a LED/UV light curing gel, and then painting it with a hybrid varnish increases the risk of ineffective hand disinfection. |
| Hewlett et al. (2018) [26] | Controlled study | Healthcare workers | 74 | The study did not show the increased number of microorganisms on nails with gel polish; however, gel nails may be more difficult to clean using alcohol hand gel. |
| Arreba et al. (2024) [27] | Prospective experimental study | Healthcare workers | 46 | Compared with unpolished nails, gel polished nails were not associated with a higher bacterial burden within 3 weeks after application, and even had a significantly lower count on day 21 before alcohol-based hand rub. |
| Anderson et al. (2021) [28] | Randomised controlled trial | Healthcare workers and students | 40 | Application of gel nail polish did not seem to affect the ability of surgical scrub to reduce bacterial viability 1 and 14 days after a manicure. |
The pilot study by Wałaszek et al. [24] found that the presence of potentially pathogenic microorganisms was correlated with the presence of UV-cured nail polish which could indicate ineffective hand hygiene. The same author conducted another study in 2021 to investigate the effectiveness of hand disinfection depending on the type of nail plate coating. The conclusion was that the risk of growing a pathogenic microorganism in the healthcare workers with hybrid varnish was similar to that of natural nails, whereas modelling the nail plate with a gel and then painting it with a hybrid varnish increased the risk of ineffective hand disinfection [25]. A study by Hewlett et al. [26] evaluated the bacterial burden of gel nails compared to standard nail polish and natural nails. They found a reduction in the bacterial burden of natural nails and standard polish, but not gel polish (p = 0.001, p = 0.0028, and p = 0.98, respectively) after hand hygiene. However, the results concerning gel polish are statistically insignificant and therefore the study did not show an increased number of microorganisms on nails with gel polish, nonetheless, it highlighted the possibility that gel nails may be more difficult to clean using alcohol hand gel. Another study which investigated the bacterial burden of gel polished nails by Arreba et al. [27] showed that gel polished nails were not associated with a higher bacterial burden within 3 weeks after application compared to unpolished nails and even had a significantly lower count on day 21 before alcohol-based hand rub. Finally, Anderson et al. [28] performed a randomised controlled trial which established that gel nail polish did not seem to affect the ability of surgical scrub to reduce bacterial viability 1 and 14 days after a manicure. However, nail length correlates with reduced effectiveness of hand disinfection [22, 24, 25].
Other health risks
A common varnish ingredient diphenyl(2,4,6-trimethylbenzoyl)phosphine oxide (TPO) has been recently banned in the European Union based on toxicological data. In 2023 it was classified as a CMR category 1B substance (carcinogenic, mutagenic, or toxic to reproduction) as well as a moderate skin sensitizer after discovering severe reproductive toxicity in rats, including testicular atrophy and infertility at high doses [29].
Conclusions
The growing trend of hybrid and gel manicures raises important health and safety concerns. Evidence suggests that prolonged use of these techniques can lead to physical and structural changes in nails with most frequently reported complaints being brittleness and splitting [4]. There are also multiple reports of allergic contact dermatitis caused by acrylate monomers present in UV-cured nail varnishes [1, 10, 11] particularly among frequent users and nail technicians. Allergens may be transported, therefore skin lesions in locations other than nails and hands may be present [1]. Non-allergic diseases associated with hybrid and gel manicure include paronychia [12] and pterygium inversum unguis [2]. Although rare, there are reports of squamous cell carcinoma of the nail unit [14] and dorsal hands [15, 16] which consider UV lamps as a potential triggering factor. While there is a study on cell lines which shows that UV lamps can damage DNA and permanently engrave mutations on the genome [18], most authors agree that UV-cured manicure represents a very low carcinogenic potential [19–21]. Nonetheless, there are recommendations for using protective measures such as sunscreen SPF50 [19] and fingerless manicure gloves [15, 20, 21] to further minimize the potential cancer risk. One study found that the risk of growing a pathogenic microorganism in the healthcare workers with hybrid varnish was similar to that of natural nails, whereas modelling the nail plate with a gel and then painting it with a hybrid varnish increased the risk of ineffective hand disinfection [25]. However, other studies did not show an increased number of microorganisms on nails with gel polish [26, 28]. There is a suspicion that gel nails may be more difficult to clean using alcohol hand gel [26], however a randomised controlled trial established that gel nail polish did not seem to affect the ability of surgical scrub to reduce bacterial viability [27].
Despite the growing body of research, significant gaps remain in understanding the long-term health effects and safety implications of hybrid and gel manicures. There is a need for more rigorous, high-quality studies especially to evaluate the risk of developing skin cancer associated with the use of UV lamps as well as risks of healthcare-associated infections. Further research should also focus on establishing clearer guidelines for safe application and removal practices as well as UV light exposure limits as those are essential to mitigate potential health risks.







