








Introduction
Numerous advantages of laparoscopy contributed to the increased use of this technique for upper and lower gastrointestinal tumors. In case of colorectal cancer it is highly recommended to use the laparoscopic approach rather than open surgery. For benign and malignant tumors of pancreas, the laparoscopic technique was adopted relatively late. There is evidence for advantages of the laparoscopic approach in left pancreatectomies compared to open technique [1–5]. Even though many years have passed since the first laparoscopic pancreaticoduodenectomy (LPD) was done, those operations are relatively rarely performed, usually by experienced surgeons in high-volume centers. Nevertheless the number of those procedures and surgeons willing to perform them is steadily increasing. It is well known that this approach is related to shortening of hospital stay, lower blood loss and acceptable perioperative morbidity [6–9]. The key factor is however oncological quality of the procedure, which should not be compromised. Resection of the portal vein or superior mesenteric vein infiltrated by the pancreatic cancer is currently a standard approach during open pancreatic surgery for cancer. Preoperative suspicion of infiltration of major veins is usually a reason for selection of open operation. When found intraoperatively it often leads to conversion. If laparoscopic pancreatic surgery is to be considered an equivalent alternative to open surgery, routine resection of vessels belonging to the portal system must also become the standard option. Nowadays, research data for laparoscopic pancreatectomies with portal or superior mesenteric vein resections and reconstructions are scarce [10–19]. We can learn from available publications that the laparoscopic approach in proper hands could be feasible and safe [20].
Aim
The aim of this work is to present our own results of laparoscopic pancreatic operation including total pancreatectomies, pancreaticoduodenectomy and distal pancreatectomies (RAMPS) performed for cancer with major venous resection and reconstructions of the portal system.
Material and methods
This is a prospective observational study. We included consecutive patients treated for adenocarcinoma of pancreas who underwent laparoscopic total pancreatectomy, laparoscopic pancreaticoduodenectomy or laparoscopic distal pancreatectomy with major venous resection and reconstruction in 2020 and 2021. The study setting was secondary referral public hospital. Patient characteristics and clinical data were included in the study. 30-day perioperative morbidity rates were recorded, classified with Clavien-Dindo grades accordingly [21].
Preoperative work-up
Standard preoperative work-up included serum Ca 19-9, bilirubin, transaminases, albumin and protein levels, and other laboratory tests needed for general anesthesia. Thorax, abdomen and pelvic computed tomography (CT) scans with contrast and/or MRI scan of abdomen with contrast were performed. In case of a high suspicion of dissemination, the PET-CT scan was performed.
Operative technique
The patient is placed on the operating table in the supine position. The operating surgeon stands between the patient’s legs, two assistants stand on either side of the patient, however the position of the operator changes frequently depending on the situation in the operating field. Pneumoperitoneum is obtained using a Veress needle. The first trocar for the laparoscope is placed in the midline above or below the umbilicus, depending on the patient’s physique. The next two trocars (10 mm on the left and right side) are placed on the mid-clavicular lines. Another two trocars (5 mm) are placed above the right and left sides in the anterior axillary lines. One 5 mm trocar under the xiphoid process is used for the retractor to elevate the liver. Specimen is delivered through the Pfannenstiel incision. After careful evaluation and exclusion of peritoneal neoplastic dissemination, evaluation is made for infiltration of the PV/SMV or CHA/SMA.
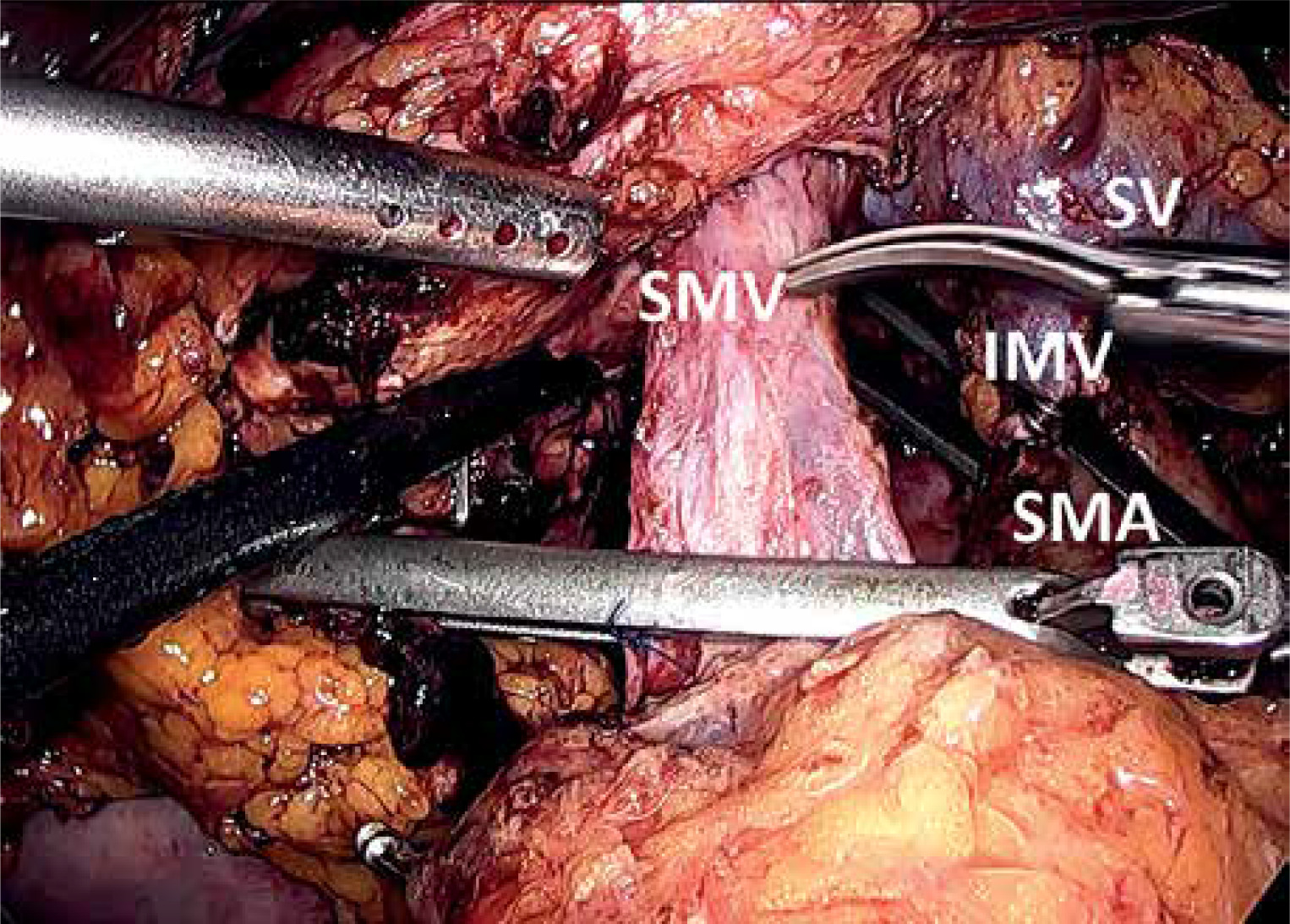
If the intraoperatively evaluated resection criteria are met (no dissemination and ability to perform resection with at least macroscopically clear margins), pancreaticoduodenectomy or left pancreatectomy resection is performed. For tumors localized in the head of the pancreas, resection was performed according to the Heidelberg technique that includes wide dissection of mesopancreas (triangle operation) [22], while left pancreatectomies were performed using the RAMPS technique as describe elsewhere [23]. The en bloc resection of the infiltrated vessel is performed in the last stage of resection (Photo 1).
Venous resection and reconstruction
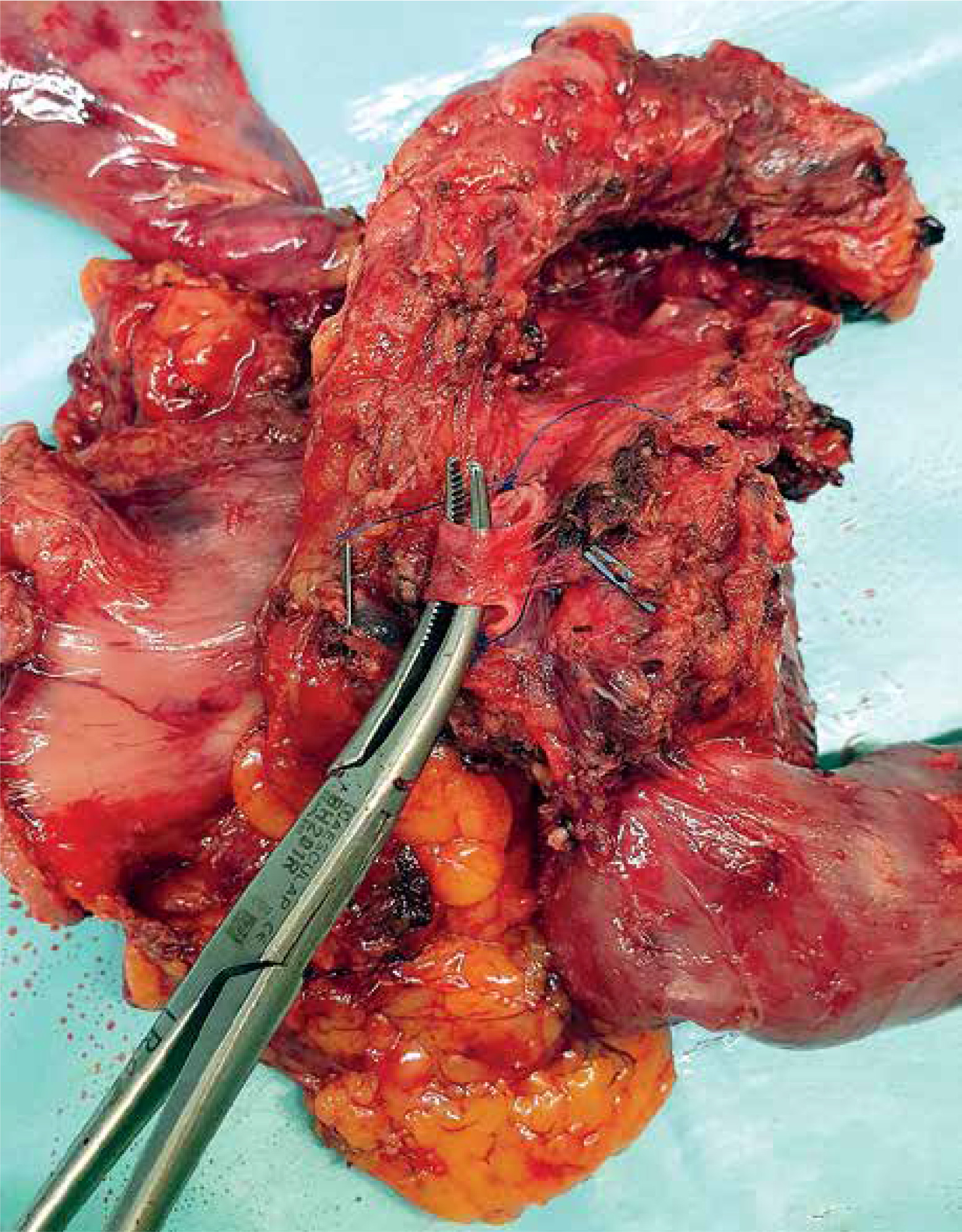
After exposure of the neoplastic infiltration of the vein, a long section of the vessel is dissected above and below the infiltration to achieve proper mobilization, and small vessels are clipped and cut (Photo 2). In case of segmental resection mobilization or if the right colon and small bowel mesentery is performed (Cattell-Braasch maneuver) to decrease tension at the anastomosis. Endoscopic vascular clamps are placed on the superior mesenteric artery to decrease inflow of blood to the small intestine and to prevent congestion. Than vein is clamped below and above the infiltration. Segmental or tangential venous resection is performed with laparoscopic scissors. In cases of segmental vein resection, the reconstruction is performed end-to-end with two 5/0 semi-continuous polypropylene sutures. The wall defect after tangential resection is closed transversely to the long axis of the vessel with two 5/0 semi-continuous polypropylene sutures (Photos 3–7). Prosthetic material (vascular grafts) or autologous vein graft has not been used for the reconstruction of veins so far. After the vascular reconstruction is performed, the vascular clamps are removed and the vessel patency is assessed using a Doppler ultrasound scan. Extra sutures are occasionally used to control bleeding. Neither local (intravascular) nor systemic heparinization was used for venous reconstruction. After obtaining a tight and patent vascular anastomosis, the reconstructive stage of post-pancreaticoduodenectomy begins. One or two drains are left in the peritoneal cavity in the proximity of pancreatic anastomosis or pancreas transection line. An enteral feeding tube is inserted below the gastrojejunostomy.
Photo 2
Beginning of transection of the portal vein above tumor. Portal vein dissected, clamped with a bulldog clamp and partially opened
PV – portal vein, PH – pancreatic head, CHA – common hepatic artery.
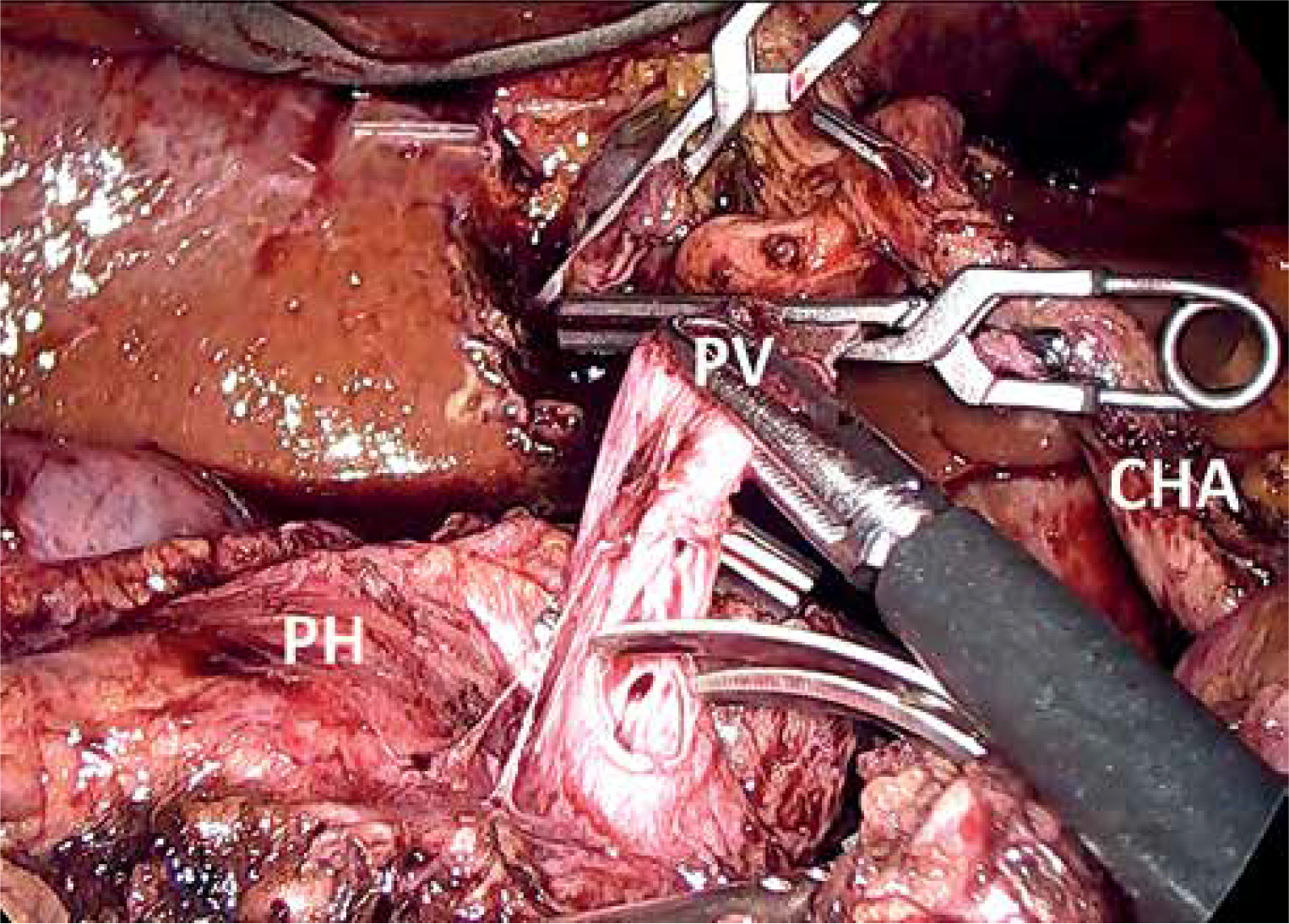
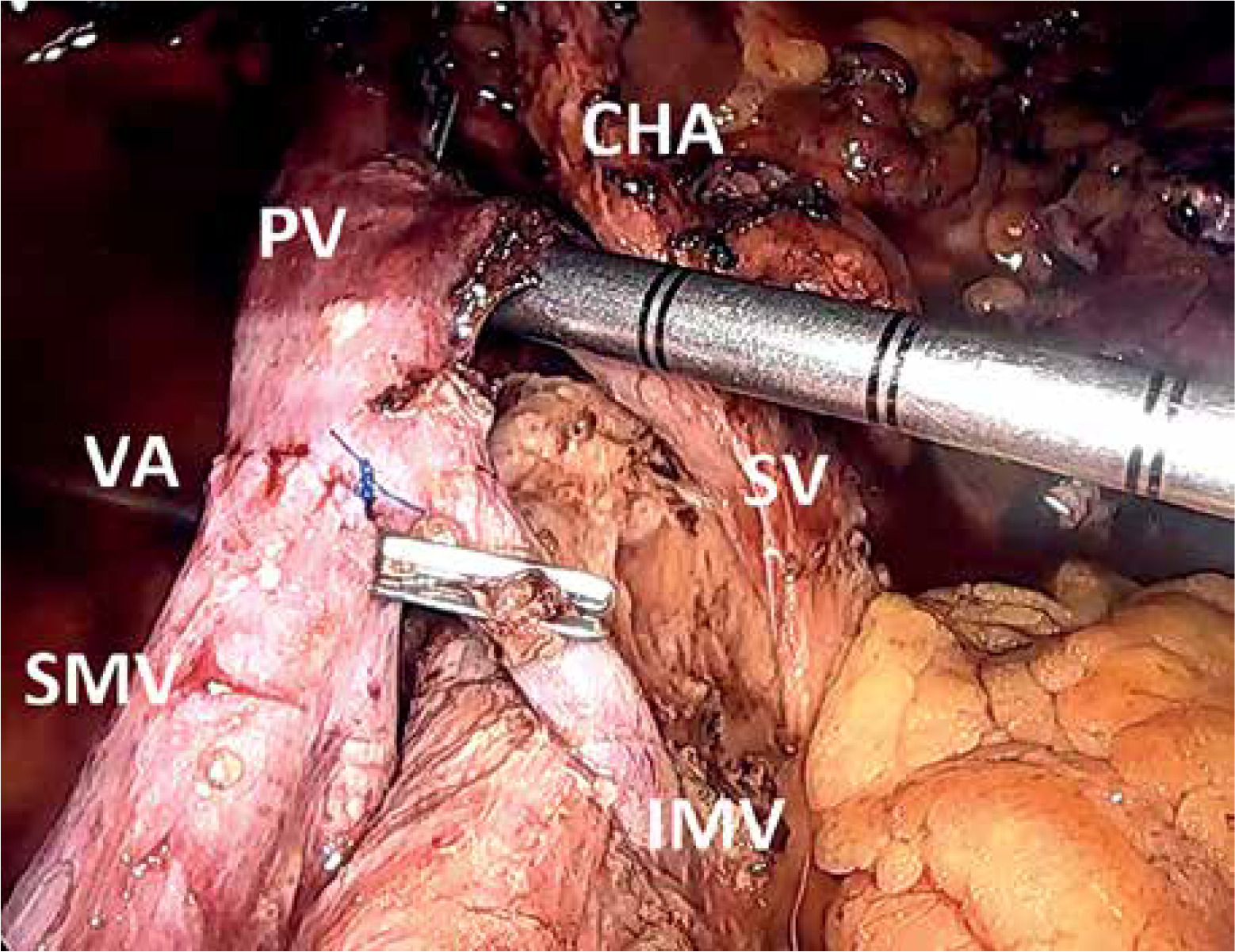
Photo 3
Reconstruction after laparoscopic segmental resection of portal system confluence
PV – portal vein, SMV – superior mesenteric vein, CHA – common hepatic artery, IVC – inferior caval vein.

Photo 4
Vascular reconstruction after laparoscopic resection of portal system confluence during pancreaticoduodenectomy
VA – vascular anastomosis, PV – portal vein, SMV – superior mesenteric vein, SMA – superior mesenteric artery, CHA – common hepatic artery, HT – “Heidelberg’s triangle”.
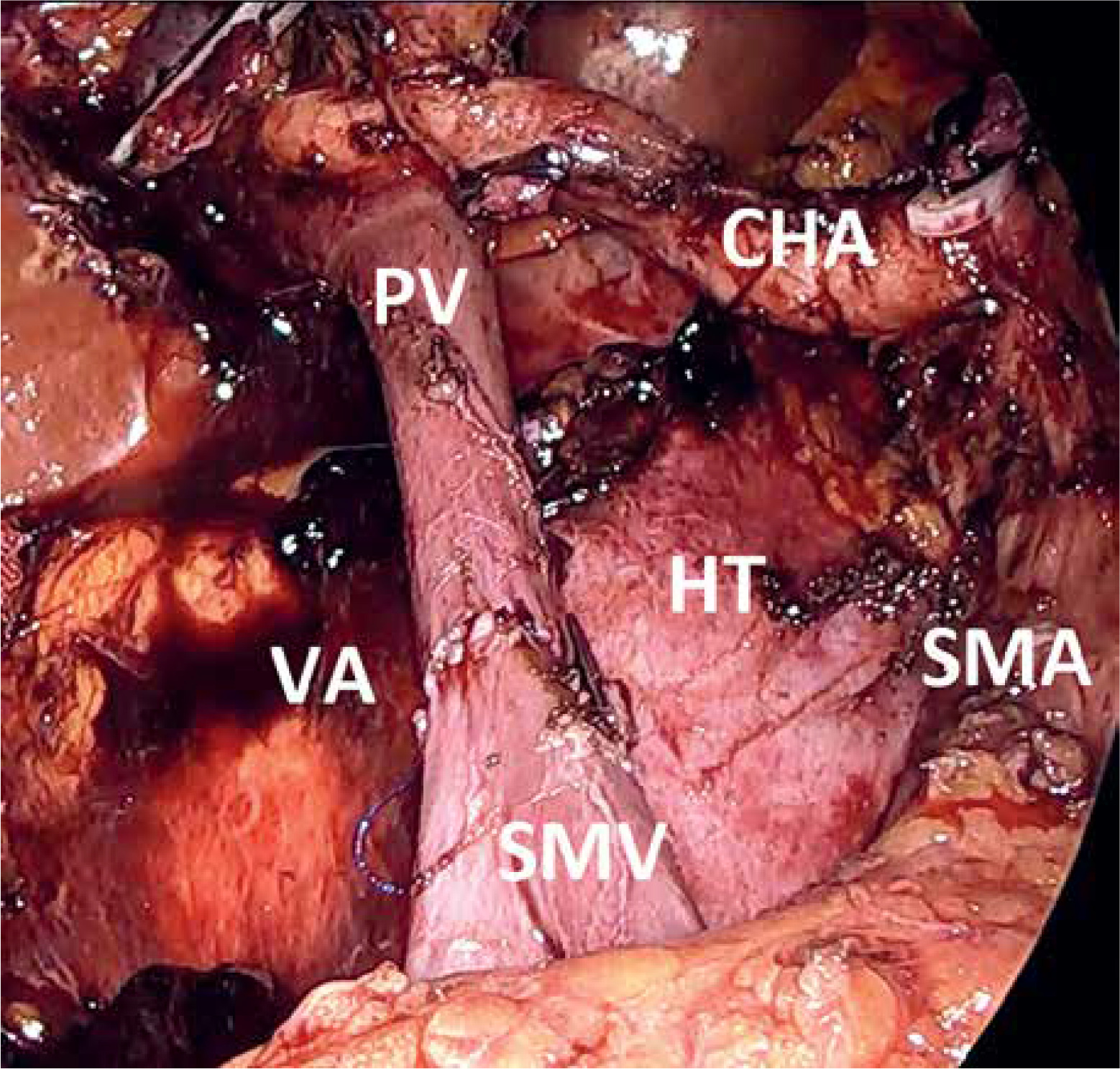
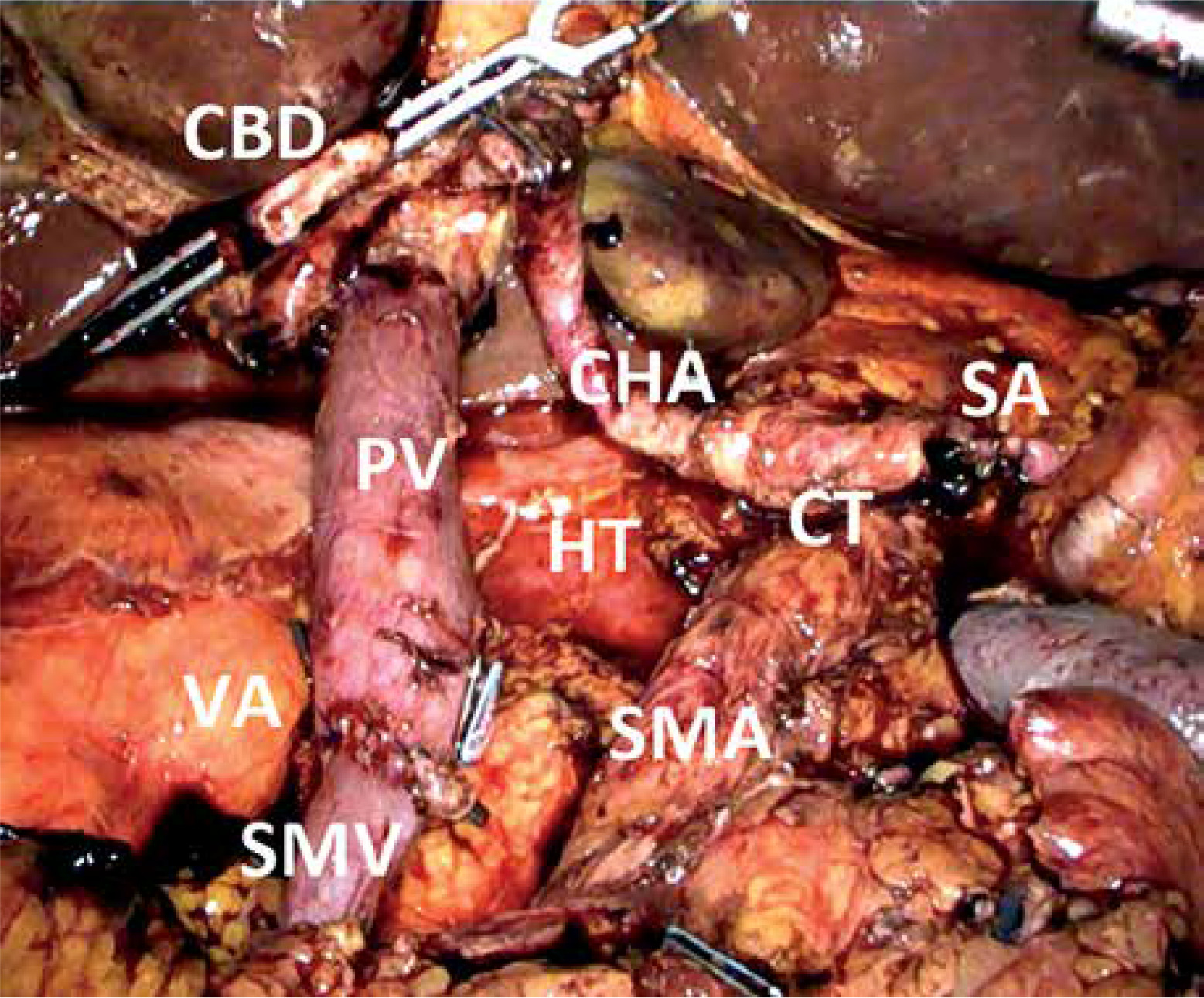
Photo 5
Vascular reconstruction after laparoscopic resection of portal system confluence during total pancreatectomy
VA – vascular anastomosis, PV – portal vein, SMV – superior mesenteric vein, SMA – superior mesenteric artery, CHA – common hepatic artery, CT – celiac trunk, SA – splenic artery, HT – “Heidelberg’s triangle”, CBD – common bile duct.
Perioperative care
Patients are treated in accordance with the Enhanced Recovery After Surgery protocol [24]. On the day of surgery, each patient receives a prophylactic dose of LMWH. Peritoneal drains are removed in the absence of symptoms of a pancreatic or biliary fistula. In the postoperative period, imaging diagnostics is performed to assess blood flow in the portal circulation.
Statistical analysis
Data were analyzed with Statistica 13.3 PL (TIBCO Software, Palo Alto, USA). Continuous data are presented as medians with range (minimal-maximal).
Ethics
All study procedures followed the ethical standards of the responsible committee on human experimentation (Institutional or regional) and the Helsinki Declaration of 1975, as revised in 1983. This is a retrospective observational study of our own clinical data that did not require official bioethics committee approval.
Results
The study included 8 patients, 6 female and 2 male patients, in median age of 68 years (56–84). Patient characteristics and perioperative outcomes are presented in Table I. Most of the patients were females (75%), median BMI was 24.4 (20.8–27.3) kg/m2. Preoperative diabetes mellitus type 2 was present in 37.55% of patients. 6 tumors were located in the pancreatic head, 1 in the pancreatic neck and 1 in the pancreatic body. Surgical procedures included 5 total pancreatectomies, 2 RAMPS and 1 Whipple pancreaticoduodenectomy. There were no conversions. Operative times are as presented in Table I. Median time of vascular closure was 55.5 (40–70) min. Median blood loss was 500 (250–900) ml. Median length of hospital stay (LOS) was 18.5 (8–34) days. We observed no complications related directly to vascular resection. Results of the histopathological examinations are presented in Table II.
Table I
Patient’s characteristic and perioperative outcomes
Table II
Results of the histopathological examination
Two patients died in the postoperative period. One due to overall friability without surgical complication. The other due to COVID infection acquired in the hospital during the postoperative period. Six patients received adjuvant chemotherapy with the combination of fluorouracil and folinic acid. After a 6-month follow-up, 3 patients were diagnosed with liver metastases.
Discussion
Pancreatic cancer has a very poor prognosis. Almost half of the patients at the time of diagnosis have distant metastases [25]. Due to the adherence of the tumor to large vessels and frequent infiltration of them, only a small percentage of patients (10–15%) [26] are considered candidates for resection. Nowadays the standard treatment for borderline resectable tumors is pancreatectomy with resection and reconstruction of infiltrated veins. The best oncological results are obtained through radical surgical treatment and adjuvant chemotherapy [27]. The most important prognostic factor is R0 resection [28]. Therefore it is of utmost importance to follow the same principles in minimally invasive surgery if it is to be considered equivalent to open surgery.
It is generally accepted that the use of laparoscopic approach in pancreatic surgery shortens the duration of hospitalization and convalescence, and thus enables faster initiation of chemotherapy. The impact of this technique on morbidity and mortality is, to say the least, questionable. Available data show that laparoscopic pancreatectomies with venous resections, in centers with extensive experience, are at least as safe and oncologically effective as open pancreatectomies with venous resection. These data encourage wider use of laparoscopic approach to improve the quality of surgery.
After acquiring substantial experience in laparoscopic surgery for pancreatic cancer, we began to use the laparoscopic technique for borderline tumors. The first resection of the vein of the portal system in our series was performed during our 317th laparoscopic operation of the pancreas.
As in open procedure an en bloc venous resection was performed at the end of the resection stage. This requires the preparation of longer sections of PV/ SMV and SMA. This approach facilitates a decision about the extent of vascular surgery and allows to obtain diseases-free margins of the resected vein. Moreover in case of segmental resection it is easier to perform reconstruction when the specimen is fully detached from other tissues. During vascular resection all major vessels both PV/SMV and SMA are closed with vessel clamps. Closing the arterial blood supply to the small bowel is believed to prevent congestion and edema of the bowel loops, which according to some authors is beneficial for the postoperative course [29, 30]. The vessel occlusion time in the laparoscopic technique is usually longer than in the open technique. We can only hope that with more experience this difference will be smaller. In the current available knowledge, there is no established length of time for safe SMA clamping during venous resection. Nevertheless, we found no ischemic or thrombotic complications during surgery. There were also no cases of intestinal ischemia, necrosis or prolonged paralytic ileus in the postoperative period in our series. PV/SMV resection and clamping are associated with an increased risk of portal vein thrombosis compared with patients not undergoing venous resection. The risk of venous thrombosis after a PV/SMV resection is 13% and varied according to the technique [31]. There is no evidence that anticoagulation reduces the risk of thrombosis following venous resection during pancreatectomy [32].
As described in the literature vascular, stapler can be used for tangential resection of a vessel, but we never used this approach due to a fear of stenosis of the vein [16]. In our Center, no grafts or autologous vein implants were used for the venous reconstruction during the laparoscopic procedure so far.
In all patients, a postoperative histopathological report confirmed cancer infiltration of PV/SMV. In 3 cases, an R1 margin was found on the resected vessel despite appropriate margins assessed macroscopically. All those patients have also other unfavorable features in the pathological report. Unfortunately, despite PV/SMV resection during pancreatectomy, the percentage of R1 margins remains still high also in other series [33–35]. Croome et al. [11] comparing laparoscopic and open pancreaticoduodenectomies with major venous resection, showed a higher percentage of R0 resections, a greater number of harvested lymph nodes and a lower blood loss using the laparoscopic approach. We have observed that laparoscopic pancreatectomy with major venous resection (LPD, TLPD, LDP) was not related to extensive blood loss in our series, which is consistent with the observations of others. Some authors claimed that it was even lower than in the open approach [36, 37].
Despite the longer operation time there were no intraoperative and postoperative metabolic, clinical and cardiovascular complications caused by prolonged exposure to anesthesia and pneumoperitoneum. We believe any disadvantages that may be caused by laparoscopy are overcome by the advantages of minimally invasive approach, including high magnification of the operating field and positive peritoneal pressure that allow for more precise and careful dissection and exposure during laparoscopy even though it cannot be documented in objective parameters.
It should be noted that performing such advanced procedures as TLPD, LPD and LDP (RAMPS) with concomitant major venous resection requires great experience in open pancreatic resections with vein resection and laparoscopic pancreatic resections without vessel resection.