








Introduction
Recurrent radiculopathy after anterior cervical discectomy with fusion (ACDF) is not common. However, if revision surgery is indicated then the choice of the best approach is important. Persistent or recurrent cervical radiculopathy is usually caused by osteophytosis or residual disc herniation [1] with secondary foraminal or lateral recess stenosis. The main problems of revision surgery after ACDF via the same surgical approach are scar tissue and arthrodesis. Alternatively, a posterior foraminotomy may be employed for nerve root decompression [2]. Another option is the lateral approach to the cervical spine described for the first time in 1968 by Verbiest [3]. This approach was developed by George over the following decades [4–6] and has been used in different cervical spine conditions [7–9], mainly for degenerative spinal stenosis with dominant unilateral radiculopathy. However, oblique corpectomy is currently not used as often as the anterior and posterior approaches for the treatment of central spinal stenosis. This technique is technically demanding and has a higher risk of complications, including Horner syndrome and injury of the vertebral artery (VA). Nevertheless, this approach can still be an appropriate choice in some clinical situations.
Aim
The aim of this report was to present the potential of the lateral approach as a less invasive surgical technique after failed ACDF. We present 2 patients with recurrent unilateral radiculopathy who underwent revision surgery using this technique.
Case reports
Case 1
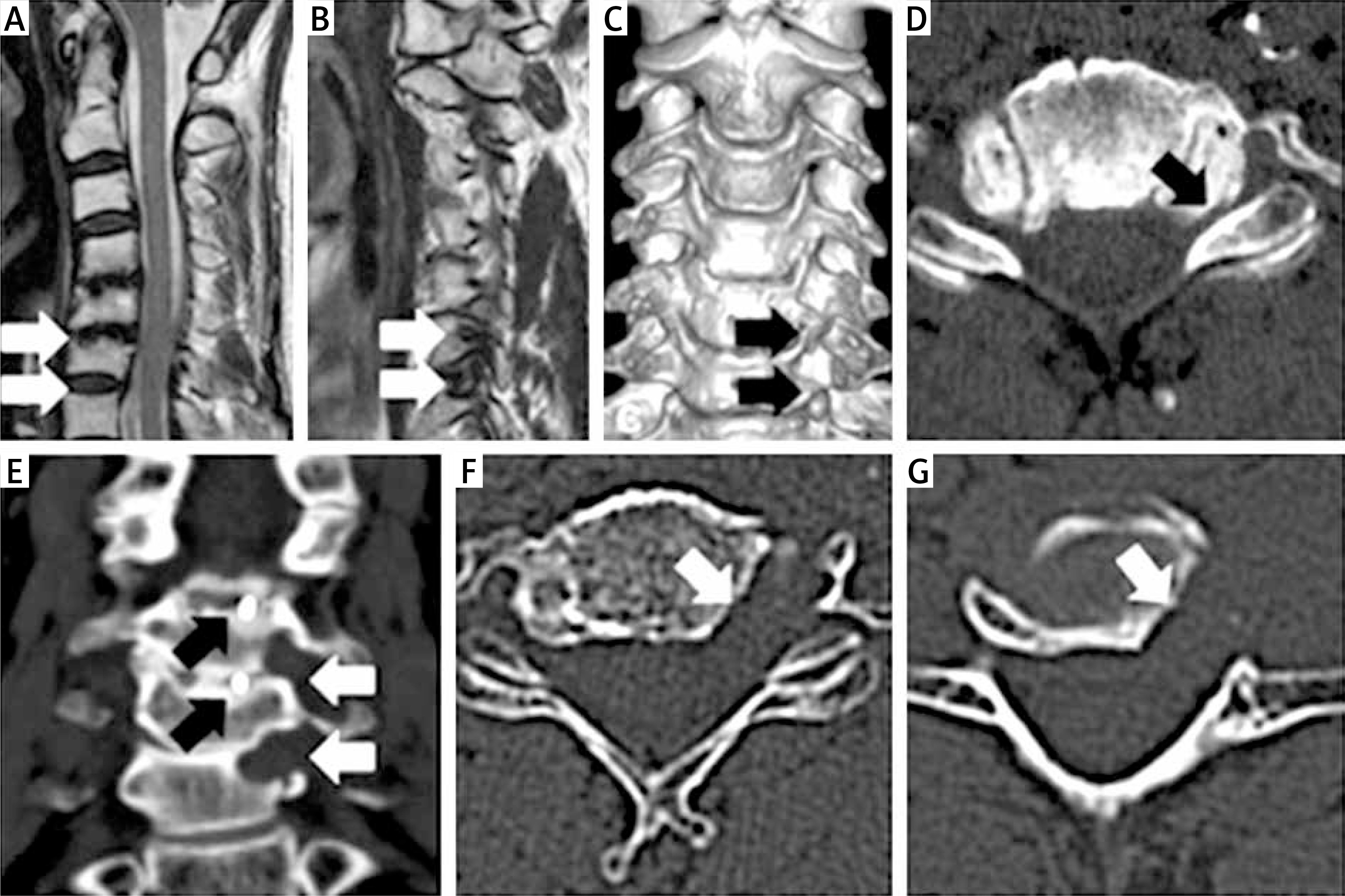
A 54-year-old woman presented with a 6-month history of unilateral radicular pain and paresis of the left upper limb. Three years earlier she underwent successful ACDF at the C4/C5/C6 levels for right-sided brachialgia. Computed tomography (CT) and magnetic resonance imaging (MRI) showed left-sided foraminal stenosis at the C5/C6 and C6/C7 levels without significant central canal stenosis (Photos 1 A–D). She was qualified for revision surgery because of increasing neurological deficit and the lack of improvement after rehabilitation. The left lateral approach between the sternocleidomastoid muscle and internal jugular vein was employed. After VA identification, anterior foraminotomy at the C5/C6/C7 levels was performed [10]. The previously implanted cage at the C5/C6 disc level was not violated. With microscope magnification, two-level anterior foraminotomy with removal of posterolateral osteophytes and soft degenerative spurs was performed (Photos 1 E–G). Selective decompression of the neural roots was accomplished. No implants were used for additional fusion. The postoperative course was uneventful. The radicular pain went away immediately after surgery and the left upper limb paresis withdrew successively. No cervical instability or symptom relapse was observed during 3-year follow-up.
Photo 1
A – Sagittal T2-weighted MR image of the cervical spine demonstrated no significant central stenosis at the C5/C6 and C6/C7 levels (white arrows). B – Sagittal T2-weighted MR image showed left-sided foraminal stenosis at the C5/C6 and C6/C7 levels (white arrows). C, D – CT scans showing spondylotic changes of uncovertebral joints with unilateral foraminal stenosis (black arrows). E–G – Postoperative CT scan showing the range of bony resection (white arrows); note that the interbody cages at the C4/C5 and C5/C6 levels remain untouched (black arrows)
Case 2
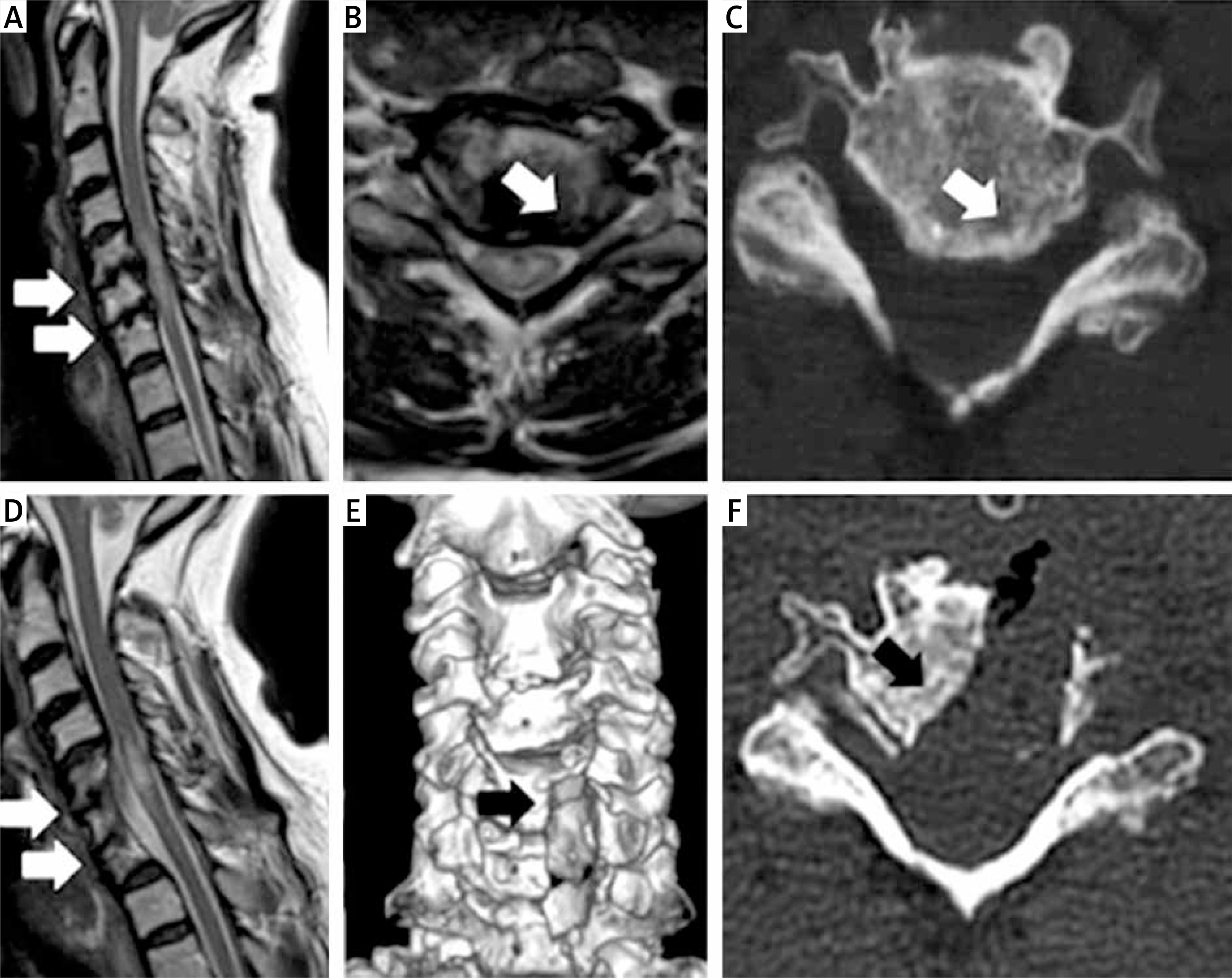
A 65-year-old woman, who was operated on for C5/C6/C7 cervical degenerative disc disease with myelopathy one year earlier, was readmitted with recurrent cervical radiculopathy on the left side. After the first surgery (ACDF C5/C6/C7), the lower paraparesis decreased and the left-sided radicular pain disappeared. However, gait deterioration, numbness of the left upper limb and periodic interscapular pain returned 8 months after the primary procedure. On the second admission, the patient presented with minor paraparesis of the lower limbs (grade 4 according to the Lovett scale) and with the Babinski sign present bilaterally. MR imaging demonstrated the progression of foraminal and central stenosis at the C5/C6/C7 levels. The radiological signs of myelopathy were unchanged compared to the first preoperative MR images (Photos 2 A, B). The patient was qualified for revision surgery. Tailored oblique corpectomy from the C5 to C7 spinal level with decompression of the spinal cord and nerve roots on the left side was performed. The interbody devices from the previous surgery were left in place and no additional fusion hardware was used. After surgery, radiculalgia was resolved and walking ability improved. At 1-year follow-up, the clinical outcome was still satisfactory and effective decompression of the nervous structures without spinal instability was documented in CT and MRI (Photos 2 D–F).
Photo 2
A – Sagittal T2-weighted MR image. Central stenosis at the C5/C6 and C6/C7 levels causing significant spinal cord compression with myelopathy (white arrows). B – Axial T2-weighted MR image. Central and left-sided foraminal stenosis (white arrow). C – Axial CT scan. Significant bone spurs causing central and foraminal stenosis on the left side (white arrow). D – Follow-up sagittal T2-weighted MR image shows clear widening of the spinal canal at the C5/C6/C7 levels (white arrows). E, F – Postoperative CT scans demonstrate the range of bony resection (black arrows)
Discussion
Recurrent cervical radiculopathy after ACDF which requires revision surgery occurs in approximately 4% of cases [1]. Adjacent segment disease is the most common reason, but progression of degenerative disease at the same level is also possible. Dowd et al. [11] described three patients who required another operation because of persistent or recurrent signs. One underwent revision surgery via the same anterior approach and two patients underwent posterior foraminotomy.
Anterior (ipsi- or contralateral), posterior and lateral approaches may all be considered for the same level recurrent unilateral radiculopathy after ACDF. However, each technique has specific advantages and disadvantages. The ipsilateral anterior approach is associated with a higher risk of soft tissue (e.g., esophagus) and blood vessel injury because of postoperative scars. The previously achieved interbody fusion must be violated in both the ipsi- and contralateral anterior approaches. Furthermore, it is difficult to ensure in the anterior approach that decompression at the distal end of the intervertebral foramen is sufficient.
Modern spine surgery strives to use minimally invasive methods [12] to decrease the risk of complications associated with a surgical approach. Therefore, posterior foraminotomy can also be employed for unilateral nerve root decompression. This posterior approach does not interfere with previous interbody fusion, but it is more appropriate for fresh disc protrusions [2]. On the other hand, the same level radiculopathy after ACDF is usually caused by osteophytes on the posterolateral edges of vertebral bodies. Therefore, simple posterior decompression may be not sufficient because it does not directly address the cause, which is the anterior compression of the nerve roots. Removal of osteophytes using the posterior approach is possible, but it is difficult and hazardous for the nerve roots and also for the VA, which is not visible with this approach.
The third option is the lateral approach, popularized in recent decades mainly by George [4–6]. In cervical spondylotic radiculopathy, the improvement rates for radiculalgia and neck pain were 85% and 94%, respectively. Motor deficits and sensory deficits decreased in 90% and 83% of patients, respectively. Only 1 patient experienced postoperative Horner syndrome and another patient presented a permanent C5 paresis [5]. Compression of the nerve roots is caused by either posterolateral disc protrusion or by degenerative changes in uncovertebral joints causing foraminal stenosis. For these reasons, George argues that the lateral approach is the most direct way for nerve root decompression.
In our experience, this surgical technique is very useful in recurrent unilateral radiculopathy after ACDF, because interference with previously achieved arthrodesis is not necessary. An advantage is the low risk of postoperative spine instability even if oblique corpectomy was performed at several levels. Osteophytes are usually resected with a high speed drill without nerve root retraction. The vertebral artery remains under direct visual control and can be mechanically protected against the drill with a spine raspatory. In comparison with the anterior approach, there is no need for esophagus retraction. We used the lateral approach in both of our patients as it directly addressed the cause of the nerve root compression, i.e., posterolateral osteophytosis. The radicular pain and upper limb paresis subsided after anterior foraminotomy in the first patient. In the second patient, because of coexisting central stenosis, a broader decompression was successfully performed with oblique corpectomy. Therefore, in similar conditions, an additional advantage of the lateral approach is the possibility of extending the decompression from foraminotomy to corpectomy [10, 13] if it is necessary and without instrumental stabilization. Decompression of the neural structures is feasible without removing the previously implanted cages. The lack of intraoperative complications, satisfactory outcome and spine stability preservation documented in follow-up encourage the use of the lateral approach more often for recurrent unilateral radiculopathy.
On the other hand, it should be noted that the lateral approach is technically demanding and requires more experience than the anterior and posterior approaches. This mainly results from the necessity of preparation in close proximity to the VA. The main steps of vertebral artery exposure include gently cutting the intertransversarii muscles at the pathological level and removing the anterior part of the transverse foramen. To avoid bleeding from the perivertebral venous plexus and to minimize the risk of vertebral artery injury, it is suggested to leave the periosteal sheath around these structures. Keeping the vertebral artery under direct visual control and, in some cases, protecting it with the spatula, especially when working with a high speed drill, may be necessary.
It is reasonable to perform CT angiography before surgery because of the possible tortuous course of the VA, its anatomical variability and modeling by osteophytes. There is also a 2.5% risk of permanent damage to the sympathetic trunk. Temporary Horner syndrome mainly causes a cosmetic defect [4]. Bilateral radiculopathy is also a limitation of this method [14].
Conclusions
Anterior cervical foraminotomy and oblique corpectomy via the lateral approach enables direct and effective decompression of neural structures without violation of previously achieved interbody fusion. Therefore, the lateral approach can also be considered in patients with recurrent, unilateral radiculopathy after ACDF.