
Oral verrucous carcinoma (OVC) is an uncommon, low-grade variant of squamous cell-carcinoma (SCC), distinguished by its slow growth, local invasiveness, and better prognosis compared to the conventional type of SCC [1]. Unclear aetiology and clinical presentation which varies and overlaps with both benign and malignant conditions make it a rare and interesting entity. We present the case of underlying OVC presenting as treatment-resistant chronic, proliferative oral candidiasis.
A 63-year-old male patient was referred to our hospital for evaluation of a verrucous white mass in the oral cavity. He reported a 4-year history of recurrent oral candidiasis, followed by appearance of a lesion on the maxillary gingiva that had been present for approximately 1 year and had progressively enlarged in recent months. A prior diagnostic workup conducted by the patient’s general practitioner included multiple swabs and microbiological analyses which confirmed oral candidiasis. Despite receiving both systemic and topical antifungal therapy (systemic fluconazole and topical nystatin), there was no significant improvement or regression of the lesion. As main reasons for delaying a hospital visit and undergoing a detailed check-up earlier the patient cited living in a rural area accompanied by a fear of respiratory infections in the post-Covid pandemic period. Consequently, biopsy of the lesion had not been done earlier. The patient’s previous medical history and laboratory results were unremarkable, and he denied any history of tobacco or alcohol consumption.
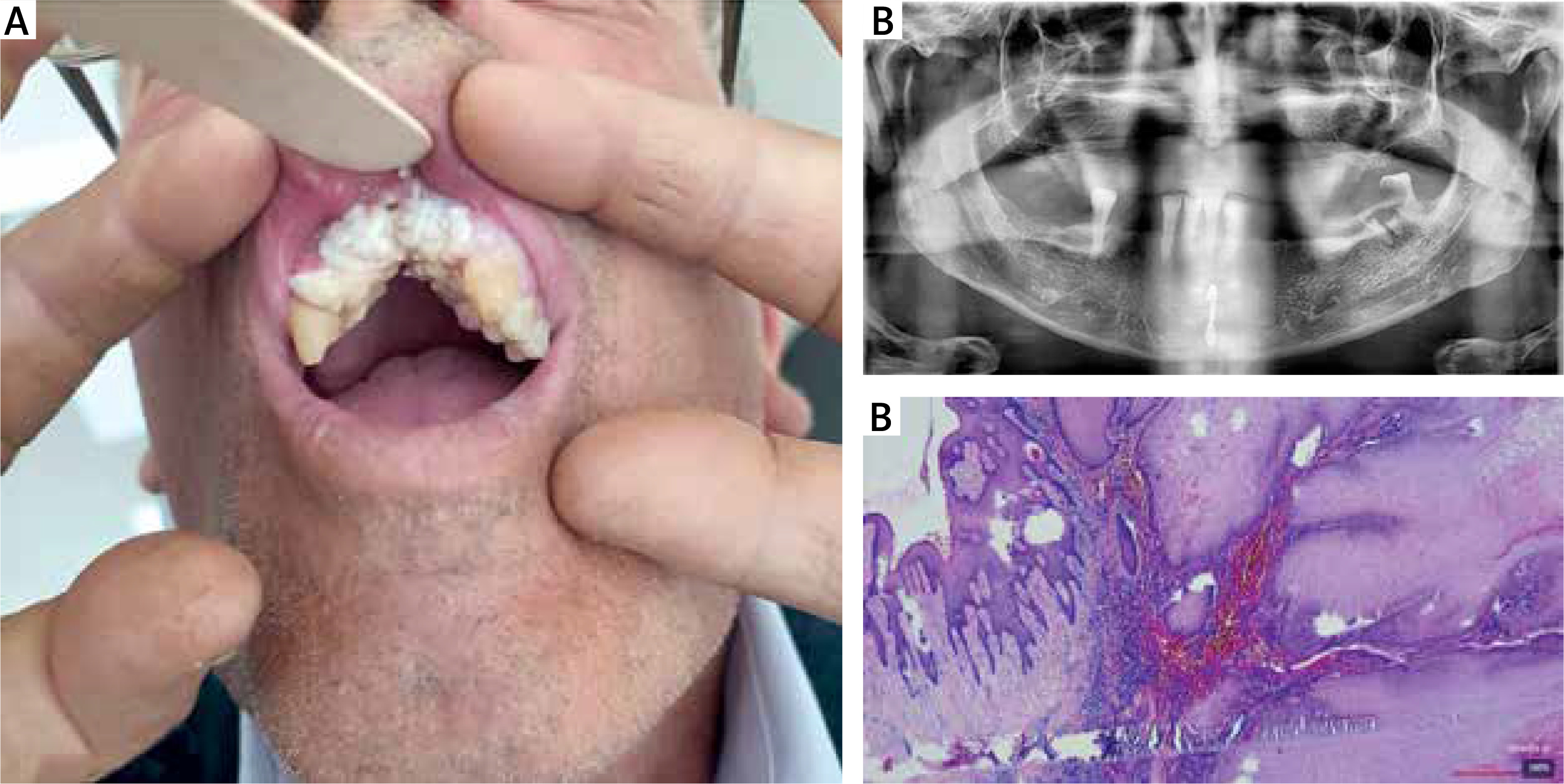
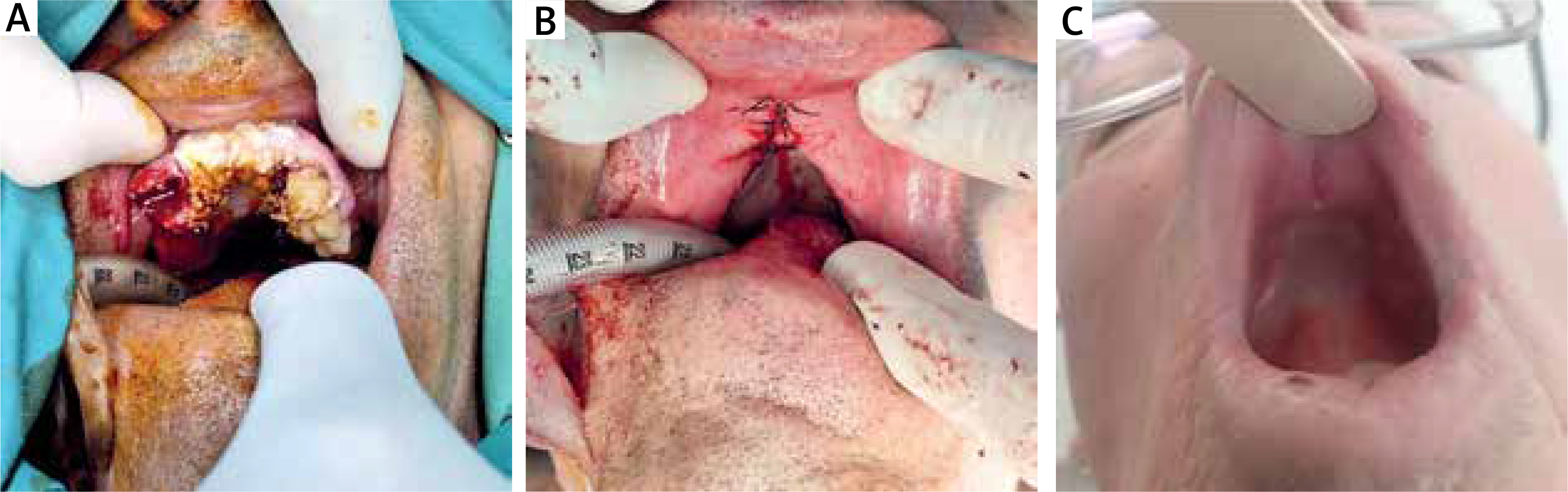
Clinical examination revealed painless, verrucous, exophytic white tumefaction on maxillary alveolar ridge from teeth #14-#24, propagating adjacent to the palate (Figure 1 A). Clinically, submandibular lymph nodes were impalpable, and physical exam revealed no extra-oral abnormalities. Orthopantomogram revealed ridge resorption in the anterior maxillary region (Figure 1 B). Incisional biopsy from three locations of the lesion under local infiltrative anaesthesia was performed. Histopathological examination of the analysed material revealed the presence of cancer tissue composed of squamous epithelium with pronounced acanthosis, papillomatosis, parakeratosis, and hyperkeratosis, exhibiting a low degree of nuclear atypia, low mitotic index, with final diagnosis of verrucous carcinoma – low grade (HG1; NG1) (Figure 1 C). Diagnostic imaging followed, ultrasonography did not reveal regional neck lymphadenopathy, and computed tomography (CT) scan of the head was performed, which showed no infiltration of the maxillary bone. After the diagnosis of oral verrucous carcinoma was established, preoperative workup was completed, the patient underwent surgery under general anaesthesia. The surgical procedure included excision of cancer en bloc with part of the alveolar ridge of maxilla, part of the hard palate, along with the extraction of teeth #11-#14 and #21-#24 (Figures 2 A, B). Histopathological examination confirmed the same diagnosis, and margins were cancer-free. The patient underwent regular clinical follow-ups monthly during the first 6 months, followed by every 2 months until the end of the second postoperative year, with no evidence of disease recurrence, and is continued to be monitored (Figure 2 C).
Figure 1
Exophytic white tumefaction on the maxillary alveolar ridge (A), orthopantomogram revealing ridge resorption (B), Microscopic confirmation of OVC (H&E, 100×) (C)
Oral verrucous carcinoma is an uncommon, low-grade variant of squamous cell-carcinoma, which accounts for 2–12% of all primary oral malignancies [1]. It is most common in male patients, after 6th decade of life, with buccal mucosa, alveolar ridge and gingiva being the most frequently affected [1]. It is characterized by low-mitotic activity, slow-growth, locally aggressive-infiltrative nature with low tendency to produce regional or distant metastases [2]. Depending on its intraoral location, that means an average span of several years until it reaches a size or infiltrates surrounding structures to an extent to produce symptoms as oral discomfort, chewing difficulties, pain. Such symptoms and absence of lesion regression are the main reason why patients seek help or request a specialist consultation [3].
Etiology of OVC remains unclear, with various risk factors being reported, including tobacco, alcohol consumption, chronic inflammation, oral ulcers, poor oral hygiene and immunosuppression [1, 3]. However, over 20% of patients have negative anamnesis for risk factors [2, 3], which leaves space to question possibility of other known causal factors of OVC.
Our patient’s history was notable for recurrent candidal infections rather than conventional risk factors, suggesting that chronic Candida-associated inflammation may have been a critical co-factor. Certain chronic bacterial, viral and parasitic worm infections and their association with malignancies (such as hepatitis C virus and hepatocellular carcinoma, Helicobacter pylori and gastric cancer, schistosomiasis and bladder cancer) have been well studied [4].. However, there is significantly less evidence linking fungal infection to cancer. Candida spp. has been associated and studied in the context of a possible link with oral and esophageal SCC, but its carcinogenic potential and underlying mechanisms are not fully understood, particularly since it is a natural commensal of the oral cavity [5]. It contributes to carcinogenic microenvironment by producing chemical carcinogenic metabolites as Nitrosamine (N-nitroso-benzylmethylamine) which can induce oncogenic mutations in DNA, by metabolizing ethanol into the carcinogen acetaldehyde; and by creating a chronic inflammatory milieu that promotes malignant transformation [6]. Clinically, of special interest are chronical leukoplakia lesions infected with Candida, termed “chronic hyperplastic candidiasis” (CHC), which have higher risk of dysplasia and malignant transformation than uninfected leukoplakia lesions [5, 6].
Benign oral proliferative, verrucous lesions such as chronic hyperplastic candidiasis (CHC), oral verrucous keratosis (OVK), oral verrucous hyperplasia (OVH), squamous cell papilloma are difficult to differentiate clinically and all exhibit overlapping histological characteristics with OVC [7]. Therefore, good communication between the pathologist and the surgeon is adamant/necessary to exclude or confirm malignant nature of the lesion as in OVC, often supported by several incisional biopsies needed to provide a good sample for analysis [1, 6, 7]. Furthermore, of special significance are lesions of OVC which contain focal areas of conventional SCC, classified as hybrid verrucous carcinoma (HVC) [8, 9], characterized by a higher recurrence rate and metastatic potential. That is very important treatment-wise, with metastatic potential of OVC being attributed to incorrect histopathological diagnosis or presence of occult component of conventional SCC in OVC [9]. Furthermore, anaplastic transformation after radiotherapy (RT) is reported in some patients and is also attributed to presence of conventional SCC in hybrid verrucous carcinoma [8]. Therefore, the decision for adjuvant RT should be case-approach based.
The location and rapid growth of the lesion, with no response to initial therapy, made our patient seek further medical assistance. Therefore, it is crucial that all lesions which do not regress nor respond to initial therapy, regardless of their benign appearance, should promptly undergo a biopsy to exclude potential malign transformation and prevent diagnostic delay [5].







