
INTRODUCTION
Palisaded and neutrophilic granulomatous dermatitis (PNGD), first described by Chu et al., is a rare reactive dermatosis associated with chronic inflammatory diseases, particularly systemic connective tissue diseases and rheumatoid arthritis [1–3]. The exact etiopathogenesis of PNGD remains unclear. Clinically, the disease is characterized by symmetrical, erythematous or skin-colored umbilicated or crusted papules located on the extensor surfaces of the extremities [2, 3]. Histopathological findings include dermal collagen degeneration, palisaded histiocytes, and neutrophilic infiltration [3, 4].
OBJECTIVE
The aim of this study was to present a case of PNGD associated with rheumatoid arthritis and to discuss its clinical and histopathological features.
CASE REPORT
A 65-year-old female patient presented to the dermatology clinic with raised, crusted, painful indurated lesions on both hands and knees that had been present for approximately 5 months. She reported no improvement with topical methylprednisolone therapy. Her medical history included rheumatoid arthritis (RA) diagnosed 20 years earlier. The patient had been treated with methylprednisolone (4 mg daily) for 2.5 years, hydroxychloroquine for 10 years, and leflunomide and sulfasalazine for the previous 18 months. Family history was unremarkable.
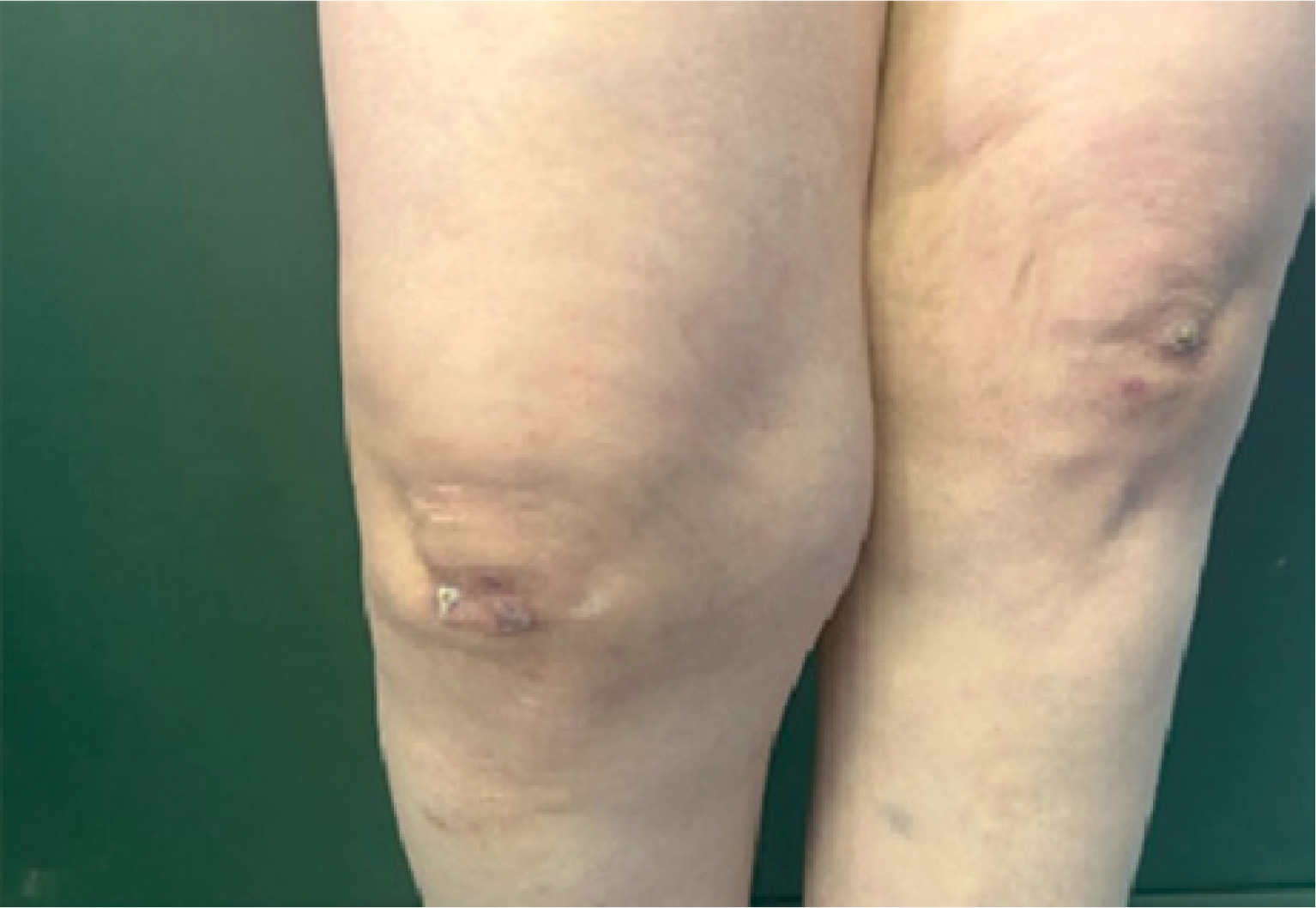
Dermatological examination revealed hemorrhagic, crusted, hyperkeratotic papules and nodules on an erythematous base located on the proximal and distal interphalangeal joints of both hands and knees (figs. 1, 2). Laboratory tests performed in cooperation with the rheumatology department showed elevated levels of anti-cyclic citrullinated peptide antibodies (anti-CCP) and rheumatoid factor (RF). Autoimmune markers were negative, including antinuclear antibodies (ANA), anti-dsDNA, anti-histone antibodies, anti-Sm, anti-Scl-70, anti-Jo-1, anti-SSB, anti-SSA, and c- and p-antineutrophil cytoplasmic antibodies (c-ANCA, p-ANCA). Complete blood count and routine biochemical tests were within normal limits. Serological tests for hepatitis B and C were negative.
Figure 1
Hemorrhagic, crusted papules and nodules on the proximal and distal interphalangeal joints of the right hand

A punch biopsy was performed with the preliminary diagnoses of rheumatoid nodule, rheumatoid vasculitis, sarcoidosis, granuloma annulare, interstitial granulomatous dermatitis, and palisaded neutrophilic granulomatous dermatitis.
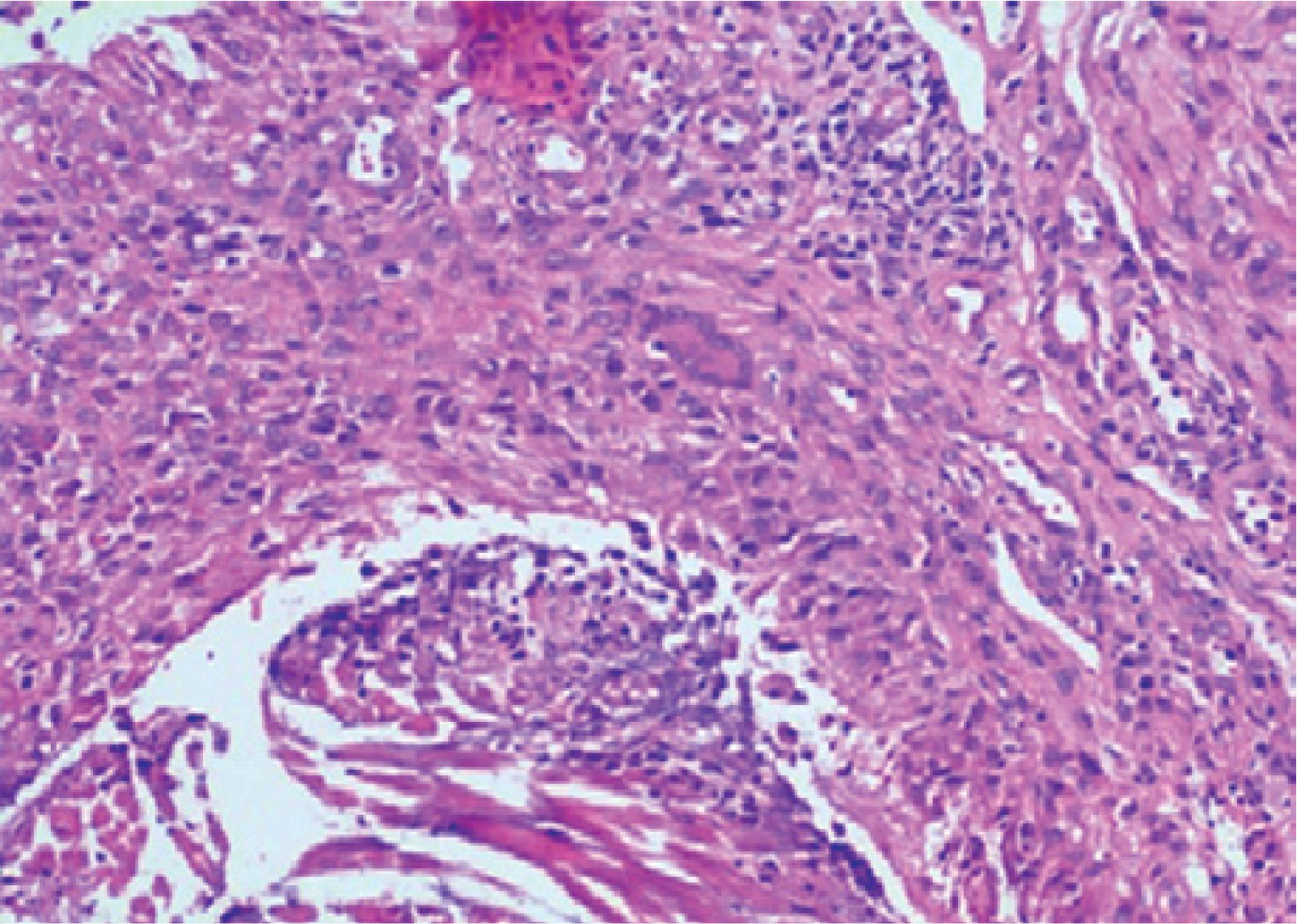
Histopathological examination revealed an irregular granulomatous reaction composed of palisading histiocytes surrounding areas of necrobiotic collagen. Neutrophilic infiltration and nuclear debris were present within the granulomas (fig. 3). At higher magnification, multinucleated giant cells, epithelioid histiocytes, and marked collagen degeneration were observed (fig. 4).
Figure 3
Irregular granulomatous reaction with palisading histiocytes and necrobiotic material within the granulomas (H&E, ×40)
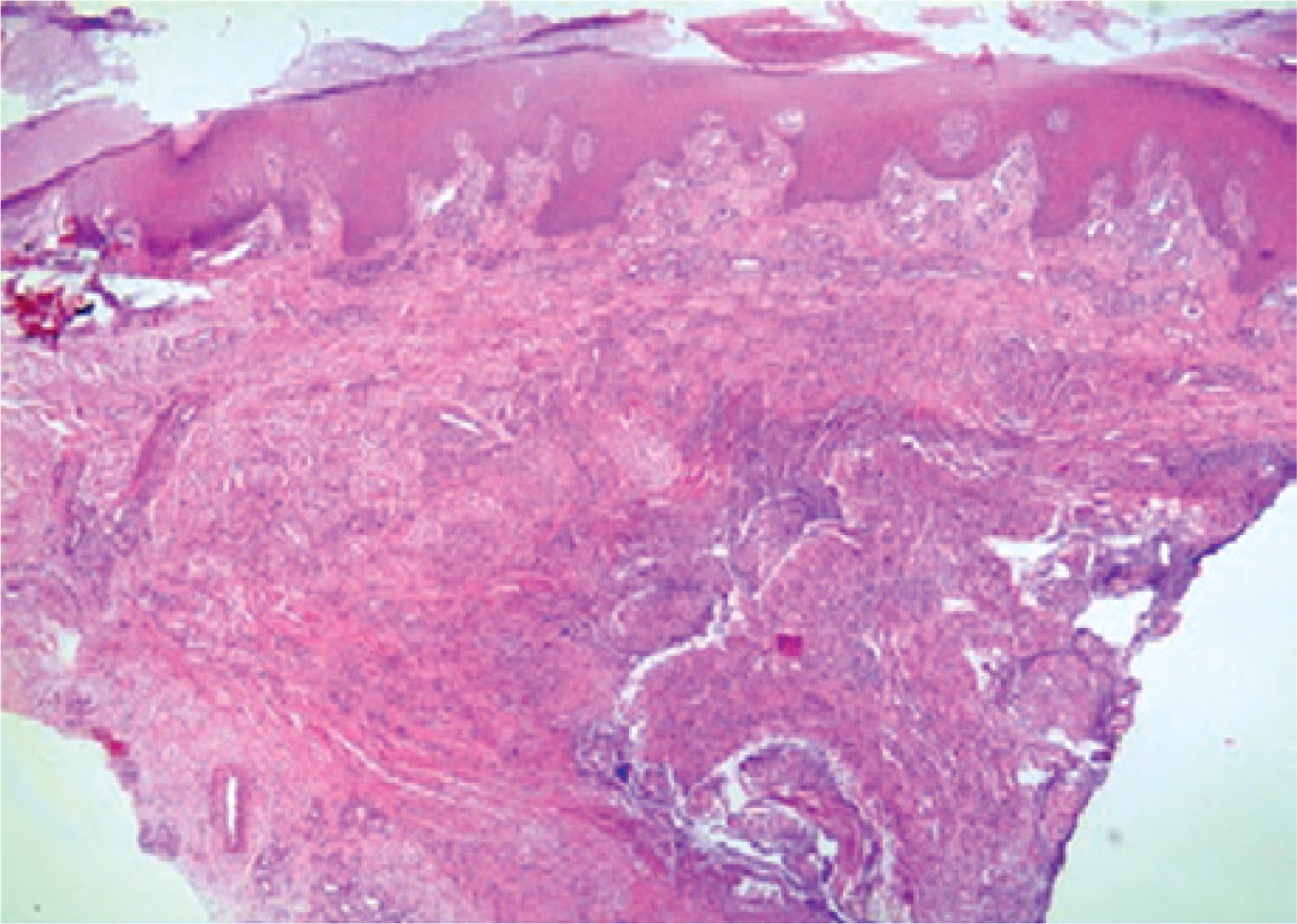
Figure 4
Multinucleated giant cells, epithelioid histiocytes, and marked collagen degeneration (H&E, ×200)
Based on clinical and histopathological findings, a diagnosis of PNGD was established. Sulfasalazine and leflunomide were discontinued by the rheumatologist, while methylprednisolone and hydroxychloroquine therapy was continued. The patient was additionally treated with topical corticosteroid ointment containing betamethasone dipropionate. Marked regression of the lesions was observed at the 2-month follow-up (fig. 5).

DISCUSSION
Different terms have been used in literature to describe PNGD. In 2015, Rosenbach and English introduced the term reactive granulomatous dermatitis to encompass PNGD, interstitial granulomatous dermatitis (IGD), and interstitial granulomatous drug reaction [3]. Although the exact pathogenesis of PNGD remains unclear, it is thought that complement activation triggered by the accumulation of immune complexes and a granulomatous response resulting from neutrophilic inflammation play a role [2, 3]. PNGD occurs more frequently in women and typically presents as erythematous or skin-colored, umbilicated or crusted papules and nodules located on the extensor surfaces of the upper extremities, particularly the elbows [2, 3].
The diseases most commonly associated with PNGD include RA and systemic lupus erythematosus. In addition, certain drugs and malignancies have been reported as potential triggers of the disease [3, 5]. Yang et al. reported that PNGD/IGD-associated lesions often occur in patients with autoimmune diseases, particularly RA [5]. In drug-related PNGD/IGD cases, in addition to tumor necrosis factor inhibitors used in RA, drugs such as allopurinol, biologic therapies, diuretics, and antiepileptics have also been reported [3, 5]. Our patient had no history of such drug exposure.
The diagnosis of PNGD is based on clinical and histopathological evaluation. In early-stage lesions, histopathology typically shows intense neutrophilic inflammation, leukocytoclastic vasculitis, and nuclear debris. In later stages, collagen degeneration, palisading granulomas, and fibrosis may be observed [3, 4]. The differential diagnosis of PNGD includes neutrophilic dermatoses, small-vessel vasculitis, granuloma annulare, interstitial granulomatous dermatitis, sarcoidosis and rheumatoid nodules [2, 3].
When PNGD is diagnosed, patients should be evaluated for an underlying systemic disease. In some cases, spontaneous resolution may occur. Reported treatment options include topical, intralesional, and systemic corticosteroids as well as dapsone. In addition, colchicine, hydroxychloroquine, methotrexate, cyclosporine, and nonsteroidal anti-inflammatory drugs may be successful in some patients [2, 3].
CONCLUSIONS
PNGD is a rare reactive granulomatous dermatosis associated with systemic diseases. After clinicopathological confirmation, patients should be carefully evaluated for underlying conditions. Therefore, PNGD requires not only dermatological assessment but also multidisciplinary clinical management.










