
A 59-year-old female patient with known hypertension and hyperlipidemia presented to our dermatology clinic with complaints of itchy brown lesions on her back that began approximately 1 year ago (Figure 1). The patient, a housewife, did not take any regular medication and was a nonsmoker. She used various topical steroids for the lesions but did not experience any improvement. A punch biopsy obtained from the brown lesion area revealed amyloid accumulation in the papillary dermis with crystal violet and Congo red staining, leading to a diagnosis of macular amyloidosis (Figures 2 B, C).
Figure 1
Pink papules in areas of hyperpigmented patches on the back. A, B – Mediastinal and hilar lymphadenopathies. C, D – Lung parenchymal fibrosis with lymphadenopathies
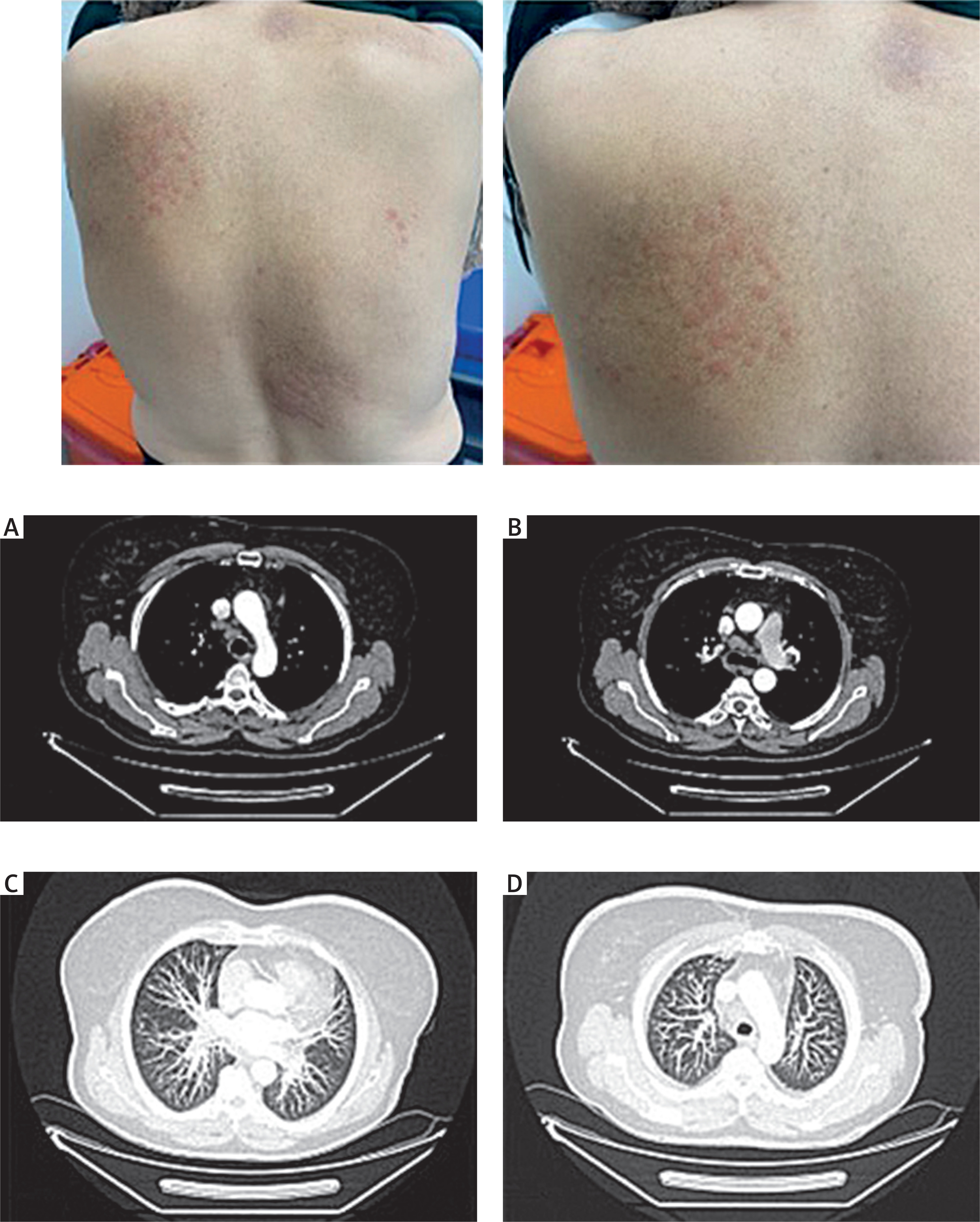
Figure 2
A – Dermal non-necrotizing granuloma structures (H and E, ×200). B – Homogeneous eosinophilic granular structures in the papillary dermis (H and E, ×200). C – Amyloid staining with crystal violet (×400)
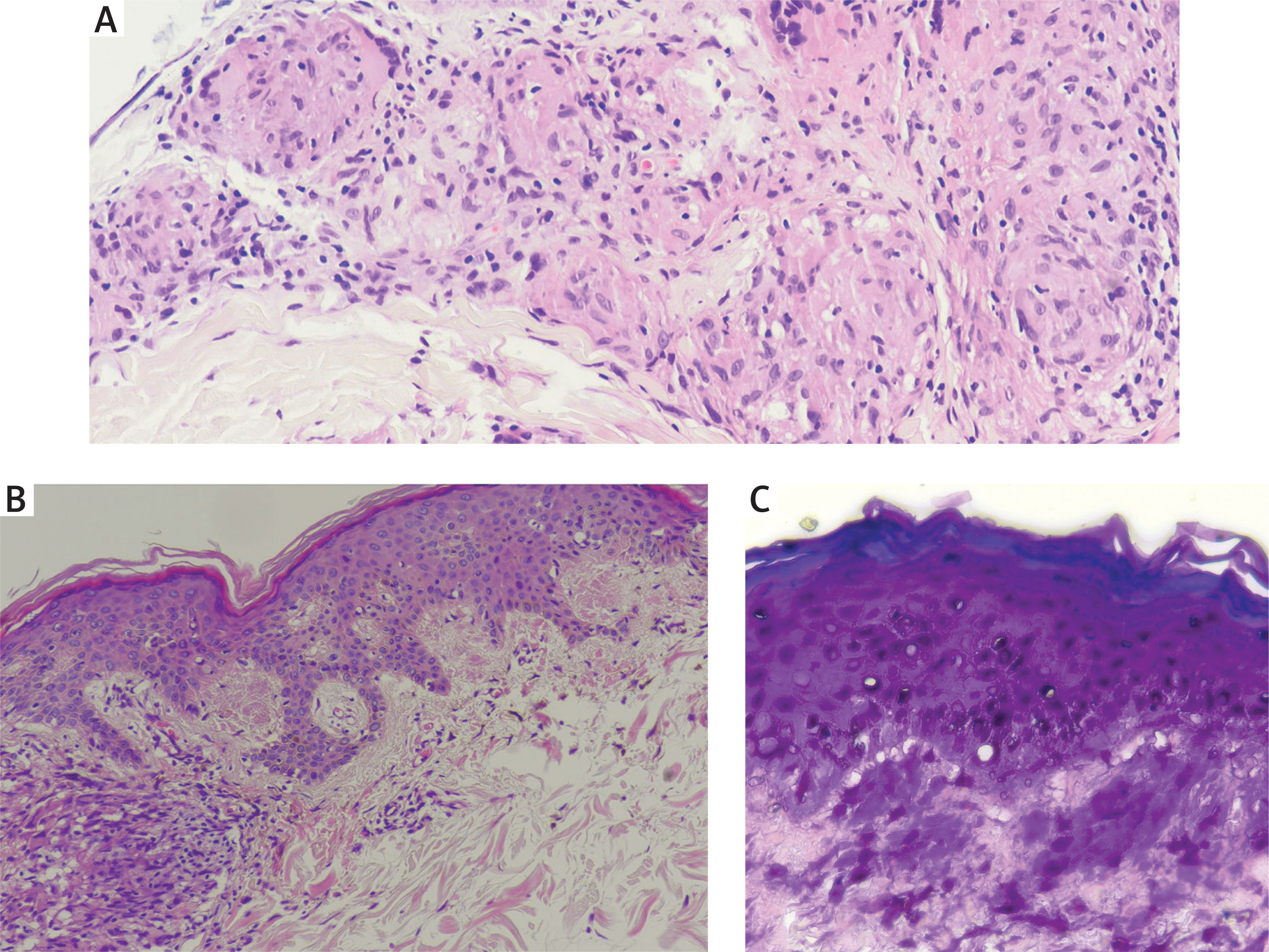
About 1.5 months later, during a follow-up appointment, the patient had new pink papules in some brown-coloured lesion areas. A second biopsy of the pink lesion revealed non-necrotizing granuloma structures in the superficial, middle, and deep dermis (Figure 2 A). Acid-fast bacillus staining for tuberculosis and periodic acid-Schiff staining for fungi were negative. The patient’s complete blood count, routine biochemistry, thyroid function tests, routine urine examination, sedimentation rate, and C-reactive protein levels were normal. Hepatitis marker, anti-HIV, VDRL, and QuantiFERON test results were negative. However, the angiotensin-converting enzyme level was elevated at 105.0 U/l (13.3–63.9). Chest computed tomography revealed mediastinal and hilar lymph nodes, with the most prominent measuring 26 × 17 mm in the subcarinal space (Figures 1 A, B). Some lymph nodes were pathologically enlarged and showed lung parenchymal fibrosis (Figures 1 C, D). Based on the clinical, histopathological, and radiological findings, the patient was diagnosed with sarcoidosis. The patient had no known diagnosis of sarcoidosis prior to developing papular sarcoidosis. Furthermore, systemic involvement had not been previously evaluated; therefore, this information is unknown. No eye, cardiac, or other organ involvement was detected during systemic investigation. Although systemic steroid treatment was recommended, the patient declined treatment and opted for topical therapy. Unfortunately, the patient did not return to follow-up.
Sarcoidosis is a significant condition because it can mimic various skin diseases and impact numerous systems and organs [1]. The etiopathogenesis of sarcoidosis is still unclear. It is thought to be related to an autoimmune response secondary to immunoregulation and various infectious and chemical agents [1]. However, information regarding the association between sarcoidosis and macular amyloidosis is insufficient.
One hypothesis proposed in the literature regarding the development of two different diseases in the same skin area is the isotopic or Wolf’s phenomenon [2]. It describes the occurrence of distinct dermatoses at the site of a previously healed skin disease [3]. Although the exact cause of this reaction is unknown, it has been suggested that an altered local immune response may play a role [3]. The factor contributing to this situation is memory T cells created through stimulation of the regional immune system in traumatized skin with an initial skin disease [2]. Secondary skin conditions that can develop at the same site include granulomatosis, lichenoid reactions, cutaneous infiltration of haematological diseases such as leukemia and lymphoma, various skin tumours, and infections [3].
Another theory suggests that skin trauma may contribute to the formation of granulomas in sarcoidosis, and an abnormal hyperimmune response to a foreign body is believed to be a trigger in some patients with systemic involvement [4]. In our case, amyloidosis may have been perceived as a foreign body that stimulated the reactive immune system, which may have triggered granuloma formation in a region of chronic trauma caused by itching.
In patients diagnosed with sarcoidosis, the specific type of cutaneous clinical manifestation is crucial for determining the disease prognosis and predicting systemic involvement [5]. Maculopapules indicate that a favourable prognosis for sarcoidosis is often observed during the acute stage [5].
Sarcoidosis therapy is managed using a patient-centred approach, with topical and/or systemic steroids being the first step, depending on organ involvement and severity [1]. In the differential diagnosis of papular lesions on the back, diseases such as syphilis, granuloma annulare, cutaneous lupus erythematosus, papular amyloidosis, mycosis fungoides, and eczema should be considered [6]. In addition, it is important to inquire about the patient’s history of local trauma, surgery, chronic inflammatory conditions, infections, and accompanying systemic diseases [7].
As a result, there are many uncertainties regarding the order in which sarcoidosis and amyloidosis appear in patients, their relationship with systemic involvement, and their impact on prognosis. Therefore, additional studies are required to determine the relationship between these two diseases, and patients should be closely followed-up.







