
Introduction
As we know, systemic lupus erythematosus (SLE) is a chronic autoimmune disease of unknown pathogenesis which can affect virtually any organ of the body, of which the skin is the second most frequently affected and relatively easily observed organ. Papulonodular mucinosis (PNM) is an uncommon but distinctive cutaneous manifestation of lupus erythematosus (LE), characterized by a diffuse deposition of mucin in the dermis [1], which is always found in patients with SLE [2]. Till now some have even presented with PNM as the major and initial manifestations, without characteristic features or positive serologic autoantibodies of SLE [3]. Under this circumstance, an accurate diagnosis and appropriate treatment of the disease pose a challenge for the clinician, not to mention that the prognosis remains incompletely unknown.
Aim
Herein this research collected the data of 13 patients from 2004 to 2024, summarised the similarities and meanwhile compared the differences between patients with PNM as only manifestations and others who met the diagnostic criteria of SLE, in order to better understand and deal with this rare situation.
Material and methods
Clinical data including the lesion characteristics, concurrent symptoms, remedies, prognosis and all the laboratory examinations were collected from 13 cases of nodular cutaneous lupus mucinosis at the Hospital of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College from 2004 to 2024. All pathological data, including histopathological features and alcian blue stain were assessed by Dr. XL Xu and Dr. Yq Jiang, respectively. Meanwhile, based on the above results, all patients were divided into 2 groups: 9 cases who presented with nodular cutaneous lupus mucinosis as the major manifestations (non-SLE group), and 4 cases, who met the diagnostic criteria of SLE (the SLE group). Comparisons between groups were performed by the SPSS 21.0 software. P-values < 0.05 were considered statistically significant.
Results
The 13 patients included 8 (61.5%) males and 5 (38.5%) females. The mean age of onset was 39.8 years, with mean disease duration of 17.2 months. The skin lesions mainly manifested as localized (5 cases, 38.5%) or generalized (8 cases, 61.5%) papules, nodules or plaques (Figures 1 A–F), besides, telangiectasias, dyspigmentation were also observed. In addition, arthralgia, oral ulcer, and alopecia was noted particularly in 2 cases (Table 1).
Figure 1
A–C – The skin lesions manifested as localized plaques. D–F – The skin lesions manifested as generalized papules and nodules
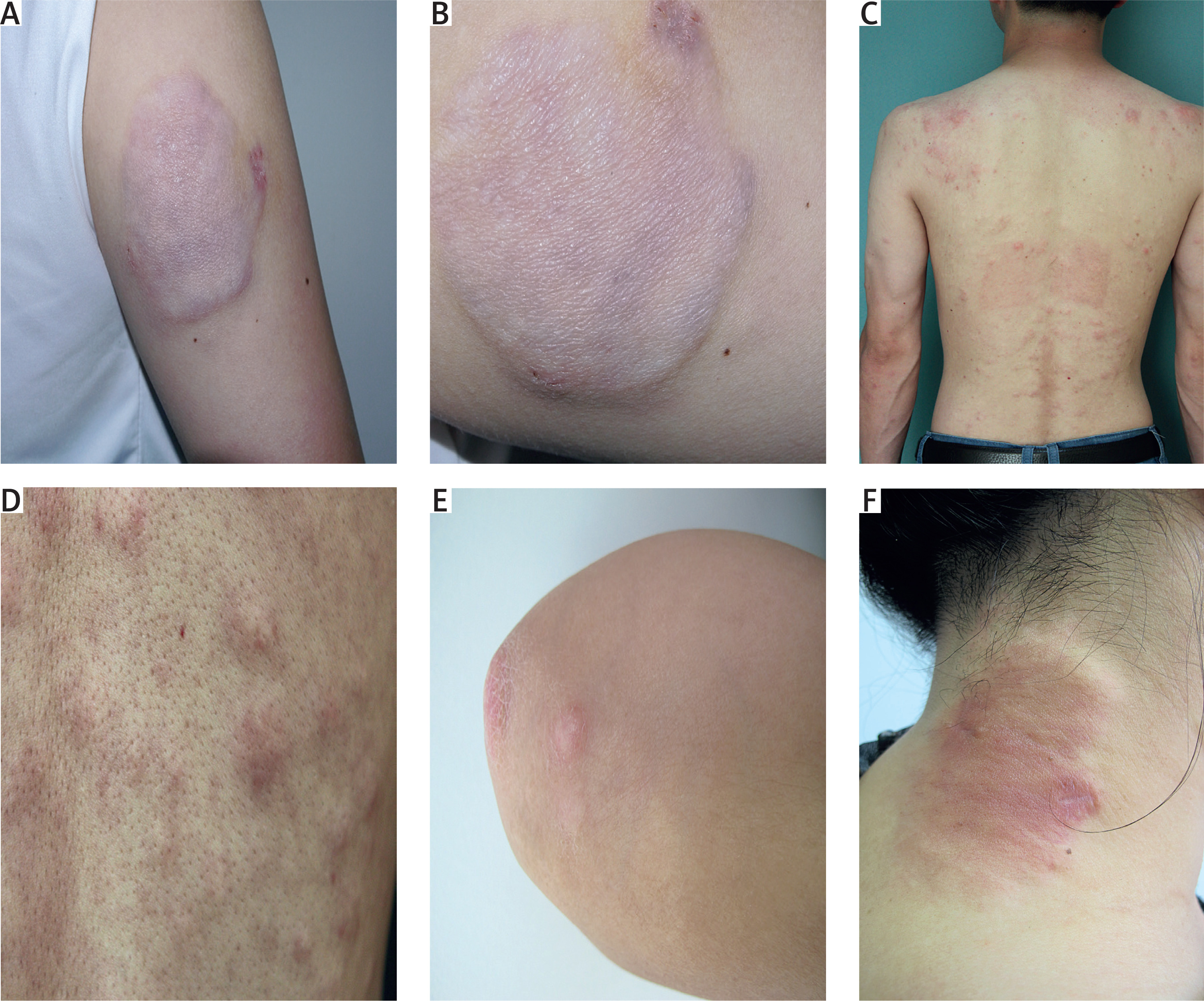
Table 1
Nodular cutaneous lupus mucinosis: clinical features and immunological examination results
| Case | Gender | Onset age (y) | Duration (m) | Distribution | Lesion characteristics | Others | Serologic examination | Treatment | Prognosis | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ANA | dsDNA | Sm | Other autoanti-bodies | C3 | C4 | |||||||||
| 1* | F | 35 | 12 | Face, generalized | Papule, nodule,telangiectasias, dyspigmentation | Arthralgia, oral ulcer, and alopecia | 1 : 640 | + | + | SSA/SSB± | ↓ | ↓ | Oral prednisolone, hydroxychloroquine and intralesional triamcinolone acetonide | Obvious improvement |
| 2 | F | 27 | 48 | Upper limb, shoulder, generalized | Patch, plaque | Lymphadene-ctasis | 1 : 160 | + | + | SSA± | – | ↓ | Oral prednisolone, hydroxychloroquine and intralesional triamcinolone acetonide | Obvious improvement |
| 3 | M | 39 | 25 | Back, generalized | Nodule, plaque, telangiectasias | – | 1 : 320 | – | + | SSA± | – | – | Oral prednisolone, hydroxychloroquine and intralesional triamcinolone acetonide | Obvious improvement |
| 4 | M | 61 | 2 | Upper limb, localized | Nodule | – | – | – | – | – | – | – | Oral prednisolone, triptolide, and tranilast | Partial resolution of the skin lesions |
| 5 | F | 40 | 8 | Back, localized | Plaque | – | – | – | – | – | – | – | Oral prednisolone, triptolide, and tranilast | Partial resolution of the skin lesions |
| 6 | M | 36 | 24 | Abdomen, generalized | Nodule, patch, scales, telangiectasias, dyspigmentation | – | – | – | – | SSA± | – | – | Oral prednisolone, hydroxychloroquine and intralesional triamcinolone acetonide | Obvious improvement |
| 7 | M | 52 | 4 | Upper limb, shoulder, generalized | Nodule | – | – | – | ± | – | – | – | Oral prednisolone, hydroxychloroquine and intralesional triamcinolone acetonide | Obvious improvement |
| 8 | M | 40 | 2 | Limbs, trunk, generalized | Nodule, plaque, telangiectasias, dyspigmentation | – | – | – | – | – | – | – | Intralesional triamcinolone acetonide | Partial resolution |
| 9 | M | 42 | 6 | Face, back, generalized | Nodule, plaque, dyspigmentation | – | – | – | – | – | – | – | – | Lost to follow-up |
| 10 | M | 8 | 12 | Chest, abdomen, localized | Nodule, plaque | – | – | – | – | – | – | – | – | Lost to follow-up |
| 11 | F | 48 | 12 | Upper limb, generalized | Nodule, plaque | – | – | – | – | – | – | – | Oral prednisolone, hydroxychloroquine and intralesional triamcinolone acetonide | Obvious improvement |
| 12 | F | 47 | 6 | Neck, generalized | Nodule, plaque, telangiectasia | – | – | – | – | – | – | – | Oral prednisolone, hydroxychloroquine and intralesional triamcinolone acetonide | Obvious improvement |
| 13 | M | 43 | 62 | Face, generalized | Nodule, patch, scales, telangiectasias | Arthralgia, oral ulcer, and alopecia | 1 : 640 | ± | 3+ | SSA3+ | ↓ | ↓ | Oral prednisolone, hydroxychloroquine and intralesional triamcinolone acetonide | Partial resolution |
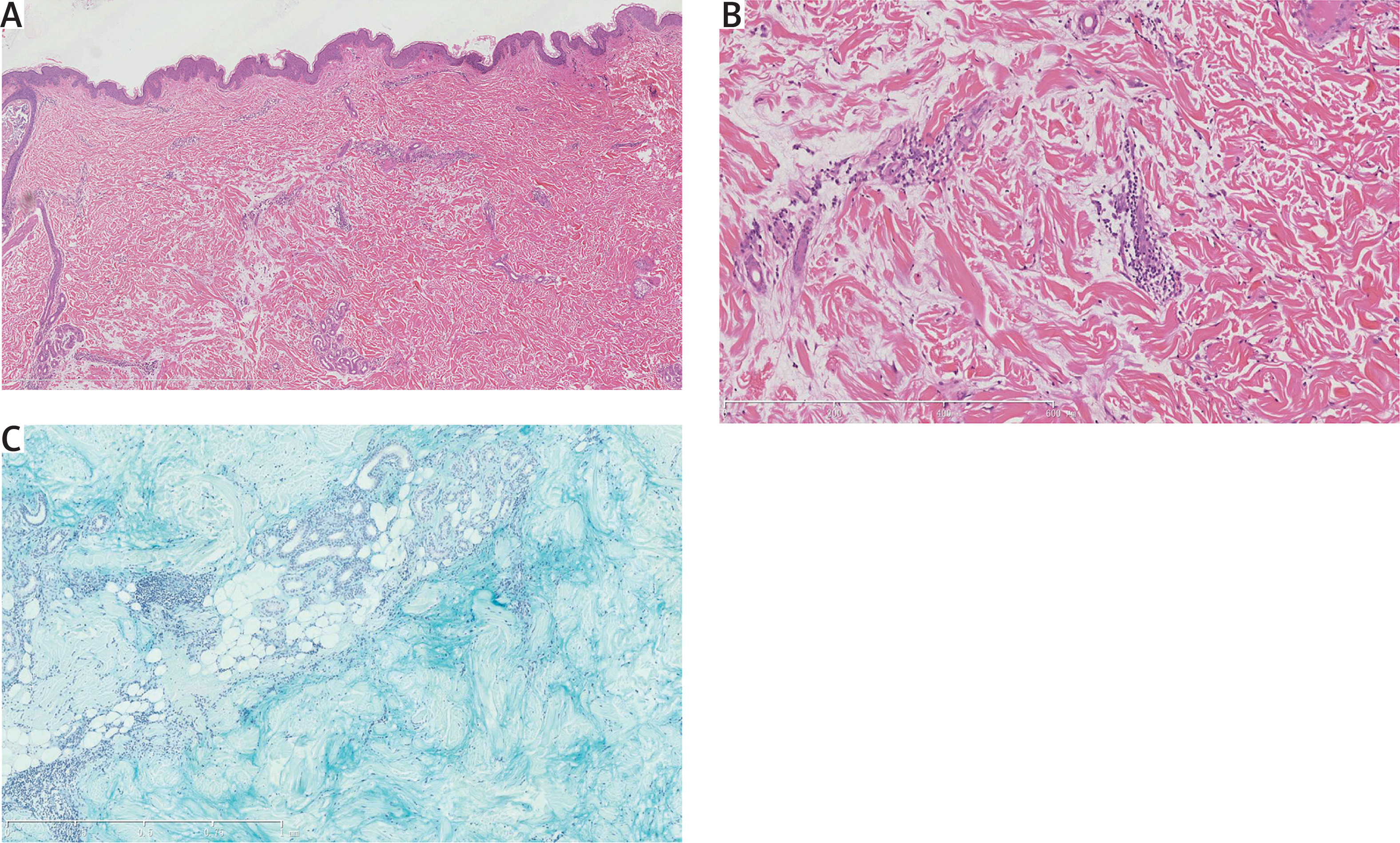
Histopathological examination showed marked dermal pallor caused by the diffuse deposition of mucin throughout the dermis (Figures 2 A, B), which were confirmed by alcian blue stain (Figure 2 C), and infiltrates composed of primarily lymphocytes perivascularly were found in all cases. Atrophic epidermis, acanthosis, and liquefaction of basal cells were presented in 2 (case 1 and 2, 22%), 1 (case 3, 11%), and 2 (case 1 and 3, 22%) cases, respectively, while other 5 (55%) cases were normal. Direct immunofluorescence examination of the lesion was positive in 2 of 6 cases (33.3%).
Figure 2
A, B – Histopathological examination showed marked dermal pallor caused by the diffuse deposition of mucin throughout the dermis, and perivascular infiltrates composed of primarily lymphocytes (HE, magnification ×10 left, ×40 right). C – Alcian blue staining confirmed the existence of abundant mucin
Serum immunological examination revealed positive antinuclear antibody (ANA) in 4 cases with 1 : 640, 1 : 160, 1 : 320, 1 : 640 titres, respectively. Other results of antibodies including anti-dsDNA, anti-Ro (SS-A), anti-Sm, anti-RNP antibodies, C3, and C4, were shown in Table 1. Besides, only 1 case was associated with leukopenia, and the results of the other laboratories, including blood and urine analysis, liver function test, thyroid function test were within normal range.
Based on the clinical, pathological features and laboratory results, diagnosis of papulonodular mucinosis for all the cases was made. Particularly, 4 cases (case 1, 2, 3 and 13) accorded with the diagnostic criteria for SLE defined by the American College of Rheumatology in 2019 as well [4]. In view of that, there were indeed some differences between the two groups regarding the aspects of clinical characteristics. The SLE group seemed to have a female preponderance (50.0% and 33.3%, respectively); it appeared to occur at an approximate age at a similar age (p = 0.492), but with a longer duration (p = 0.004) compared with the non-SLE group. Their lesions tended to be more generalized and multiform, and it also has a higher prevalence of some nonspecific symptoms, such as arthralgia, oral ulcer, and alopecia. On the contrary, patients from non-SLE group, who did not meet the diagnostic criteria of SLE, had not the above features, and their laboratory findings were almost within normal range (Table 2). Pathologically, there seemed to be no obvious differences, except for the changes of epidermis or liquefaction of basal cells, which were present in the SLE group. Therefore, it can be concluded that the above characteristics are associated with a higher risk of SLE.
Table 2
Comparative characteristics of patients with papulonodular mucinosis
The SLE group adopted the regimen of oral prednisolone of 20 mg/day, and hydroxychloroquine of 400 mg/day, together with intralesional triamcinolone acetonide and 3 cases gained an obvious improvement while 1 case achieved partial resolution after 4 weeks. Due to the generalized lesions, 4 cases of the non-SLE group also received the same remedy, leading to significantly softer and thinner lesions. Also another 2 patients received a remedy of oral prednisolone, triptolide, and tranilast, which led to partial resolution of the skin lesions at 2 months. Fortunately till now they all have not shown any other symptoms of SLE. One patient was given barely intralesional triamcinolone acetonide and still achieved partial resolution. The other two failed to adopt any effective treatment and were lost to follow-up eventually.
Discussion
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease of unknown pathogenesis. Patients can present with variable clinical features ranging from mild joint and skin involvement to life-threatening renal, hematologic, or central nervous system involvement. Cutaneous lupus erythematosus may occur as an independent disorder or in association with SLE. The subtypes of LE-specific skin disease have varying degrees of association with SLE. Papulonodular mucinosis (PNM), or cutaneous lupus mucinosis (CLM) was first reported in 1954 by Gold [5], who described an unusual papular eruption characterized by mucinous dermal deposits in two SLE patients. However the pathogenesis of PNM is also unknown. Increased production of glycosaminoglycans by dermal fibroblasts has been described, stimulated by an unknown factor in serum, possibly immunoglobulins or cytokines [6]. Other possible contributing factors may be ultraviolet light and sex-related factors such as androgenic hormones [7]. Although minute amounts of mucin deposition can generally be found in patients with SLE, it is rare to find large, clinically palpable mucinous deposits presenting as nodular lesions. Till now very few cases have been reported in the literature and even fewer as the initial presentation without other typical manifestations of SLE. In the present study, through analysing the clinicopathologic and prognostic features of all the patients, the similarities are summarised and differences between the two groups are compared, in order to provide clinicians with more relevant information on these patients. This study found that patients with PNM who have extensive and diverse skin lesions have a higher risk of developing SLE. In addition, this is the largest case series study of PNM in China.
Clinically PNM presents as asymptomatic, flesh-coloured papules or deep, fleshy nodules, giving a lumpy appearance, and without any atrophy, scar, or pigmentation after recovery. The lesions usually involved the trunk and upper extremities [8]. In our cases, a series of clinical features including the onset age, the duration and the lesion characteristics of the SLE group were summarized and we therefore consider that recognition of these special features may help us get an earlier and accurate diagnosis even when the patient is lacking other typical manifestations of SLE. Histology typically shows a slight lymphocytic perivascular infiltrate, large amounts of mucin deposition between the collagen fibres of the reticular dermis, with stellate fibroblasts and rare mast cells, with or without evidence of epidermal changes. Among them, mucin deposition is the most common histologic finding [7]. On the basis of the unique histological features, the diagnosis of PNM can be supported. In our cases, diffuse deposition of mucin throughout the dermis were obvious of the most obvious of all. The liquefaction of basal cells was present in only 3 cases, stating that epidermal changes may not be required for the diagnosis of the disease, but may be a hint for diagnosis of SLE. Beyond that recent reports have also documented vasculitis in PNM [8], which may also remind of the diagnosis of SLE. Besides, according to the prior literature [3], ANA positivity in PNM has been observed in 25 of 30 cases (83%), while 3 of 30 cases were ANA negative and 2 of 30 were not reported. Considering the high positive rate, it is indispensable to conduct a long-term monitoring. Typically the following laboratory results yield the diagnostic value for SLE: positive anti-dsDNA antibodies, increased erythrocyte sedimentation rate, and positive ANA, especially with a speckled pattern, though a homogenous pattern also has been described [2]. Among all PMN patients, 61.5% were male, contrasting with the female predominance in lupus spectrum disorders. Given the limited sample size of this study, this discrepancy may be due to random factors, and future research should expand the sample to better track this phenomenon.
On the basis of a previous review [3], 77% of patients with PNM had met 4 of the 11 criteria defined by the American College of Rheumatology for SLE prior to presentation. In another review of 41 cases of PNM associated with LE, 31 (75.6%) patients had SLE, 8 (19.5%) had discoid lupus erythematosus (DLE), and 2 (4.9%) had subacute cutaneous LE [7]. Therefore, a hypothesis that PNM was highly associated with SLE was put forward. However, in spite of that, its relationship with LE is somewhat variable: in some cases, patients with PNM had, by history, demonstrated signs and/or symptoms of SLE or DLE months before actual presentation; while in other cases, patients presented with lupus mucinotic nodules as the initial and only manifestations, without any typical symptoms (arthralgia, proteinuria, and malar rash), just as some of our cases. So that there is still a considerable proportion of patients, in whom the diagnosis of SLE may not be given. At this time, the above clinicopathologic features may give hints for final diagnosis of SLE. In addition, other documents of PNM had confirmed that, although in some cases, it was asymptomatic and without evidence of systemic disease during follow-up time [3, 9, 10], the prognosis of those patients has not been recorded till now, not to mention that some patients with PNM and SLE proved to be more vulnerable in joint and kidney involvement (present in half of the cases) [7], which further highlights the need for vigilance regarding atypical presentations of SLE. In brief, it seems to be particularly important to conduct a long-term monitoring and determine how to treat appropriately, since such patients may or may not subsequently develop characteristic multisystem features of SLE in the following months or years.
Although no consistently effective therapy has been reported, systemic or local glucocorticoids and antimalarial drugs have been used with some success to treat patients with PNM and especially accompanied with SLE [11], just as in our cases. The response to systemic corticosteroids (up to 60 mg of prednisone daily) has been observed in the reported cases, with significant improvement in the cutaneous lesions in all patients. Besides, the use of antimalarials or intralesional injection with triamcinolone alone also showed some efficacy [3], consistent with some of our cases. Interestingly, some scholars [3] once reported the case of ANA-negative PNM without SLE who responded to hydroxy-chloroquine and intralesional triamcinolone. Given the rarity of that condition and reported association with SLE, it is indeed important to follow these patients clinically for any signs or symptoms of systemic involvement, sometimes even to treat it as SLE, especially those with the above clinicopathologic features. In one word, despite the different clinical presentations, the similarly distinctively histological features give hints to accurate diagnosis and systematic treatments. The good outcomes in turn support such remedies.
This retrospective study has certain limitations. The small sample size and lack of standardized follow-up duration resulted in some findings lacking accuracy. In future studies, continuous collection of clinical data from PMN patients to expand the sample size and standardized follow-up will be implemented. Despite these limitations, the study still provides valuable insights due to its unique data.
Conclusions
In many patients, papulonodular mucinosis can precede the onset of nonspecific symptoms or autoantibodies of SLE by several years, or occur in their absence. The clinical manifestations and unique histological features highlighted in this study can aid in accurate diagnosis and better management of this rare condition. Given the strong association between these two diseases, recognizing the correlation of clinicopathological features and maintaining close follow-up are essential, particularly as the risk of progression to systemic disease remains to be fully determined.







