








Introduction
Petersen’s hernia (PH) is a type of long-term complication that occurs after gastrointestinal surgery, resulting in herniation between the transverse mesocolon and jejunal limb mesentery [1]. It may occur after total or distal gastrectomy (DG) with Roux-en Y (RNY) reconstruction, Billroth II (B-II) reconstruction, and RNY gastrojejunal bypass. It has been reported that it occurs in approximately 2.5–6% of patients after laparoscopic RNY gastrojejunal bypass surgery performed for obesity [2, 3]. After the small intestine herniates in Petersen’s space, it progresses with intestinal necrosis or intestinal perforation. If PH is not diagnosed early or is misdiagnosed, it can cause sepsis in a short period of time, and the mortality rate increases dramatically. PH is reported to account for 0.5–5% of all cases of total small bowel obstruction, and the overall mortality rate increases by more than 50% in the case of bowel necrosis [4, 5]. Due to this course, PH requires emergency surgery.
With the recent expansion of minimally invasive surgery in the surgical field, the number of reports on laparoscopic surgery in the treatment of intestinal obstruction is increasing. Laparoscopic surgery can reduce the incidence of postoperative complications compared with the open approach [6]. Compared to open adhesiolysis, the frequency of laparoscopic adhesiolysis increased from 17.6% in 2006 to 28.7% in 2013 [7]. However, some surgeons still question the application of laparoscopic surgery in treating intestinal obstruction due to the possibility of artificial intestinal damage during surgery and limited visibility. Laparoscopic surgery for the treatment of internal hernias is still reported in case reports in limited patients rather than being recognized as a standard treatment [8].
Aim
To identify predictive computed tomography (CT) profiles of patient suitability for laparoscopic reduction of PH by a comparative analysis between patients treated by laparoscopic and open reduction.
Material and methods
A retrospective observational study was designed and carried out according to the principles of the Declaration of Helsinki, 1989. This study was approved by the institutional review board (Approval number of corresponding author institution, GNUH-IRB-201908002).
Patients
We retrospectively collected the clinical data of patients who underwent PH repair surgery after minimally invasive gastrectomy for gastric cancer between 2015 and 2018. Patients who underwent surgery for PH after a past laparoscopic or robotic gastrectomy at four hospitals were enrolled.
Six expert surgeons in laparoscopic gastrectomy have been meeting for the laparoscopic reduction of PH since 2015. All surgeons are specialists in gastric cancer surgery with experience in performing more than 200 laparoscopic gastrectomies. We examined preoperative CT scans and decided to perform the laparoscopic or open reduction of PH. The recruitment of patient data was indicated after the first laparoscopic reduction by each surgeon.
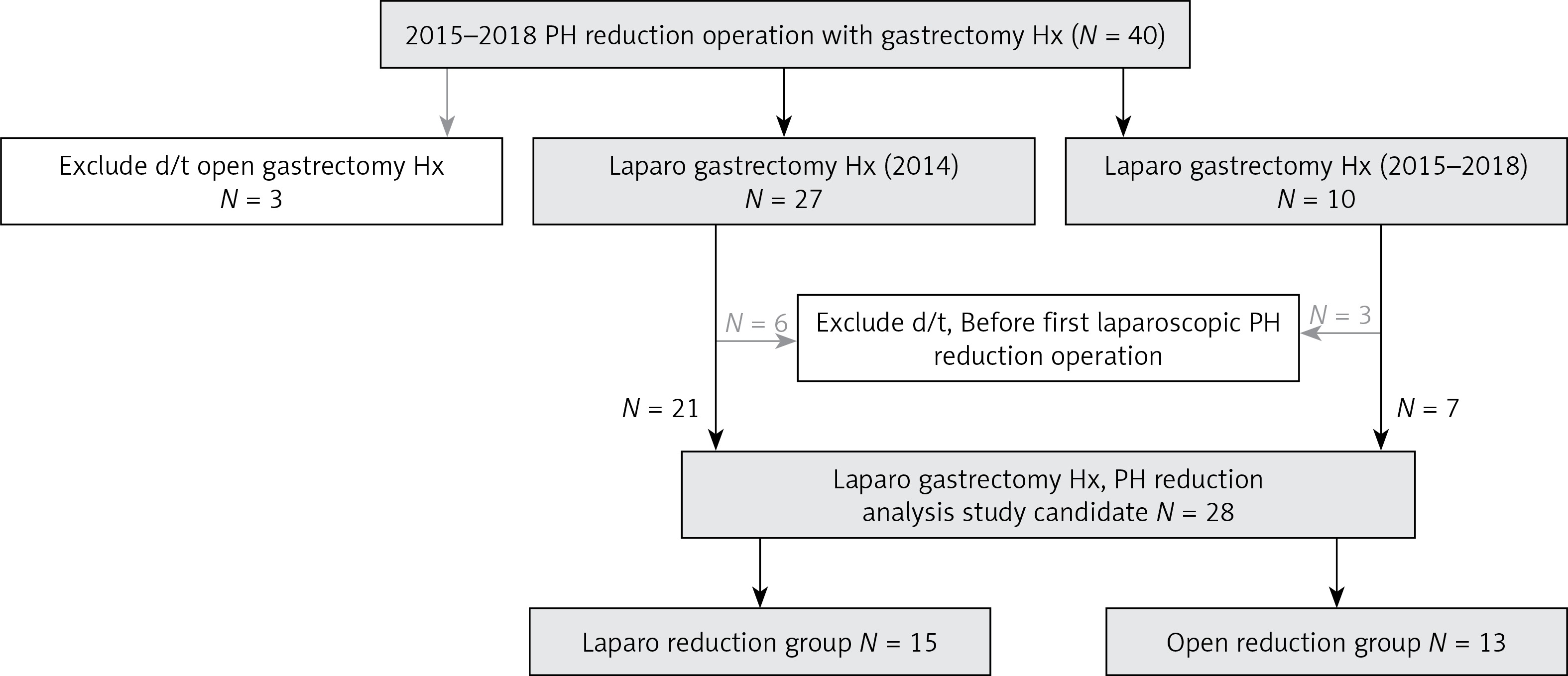
Data of patients who underwent surgery from 2015 to 2018 for intestinal obstruction caused by PH were collected (Figure 1). The inclusion criteria of this study were as follows: 1) previous radical surgery for histologically proven primary gastric adenocarcinoma; 2) no evidence of other distant metastases; 3) previous laparoscopic or robotic gastrectomy; and 4) reconstruction by RNY reconstruction or the gastrojejunostomy (GJ) procedure.
We excluded patients according to the following criteria: 1) preoperative patient condition of septic shock; and 2) experience of the initial operation because laparoscopic PH reduction is a rare procedure. There is a need to determine evidence of the possibility of laparoscopic PH reduction for each surgeon.
Methods for CT scan
CT scans were performed using a multidetector scanner (Brilliance iCT; Philips Healthcare, Cleveland, OH, USA). The CT scanner was set to have the following parameters: detector collimation = 64 × 0.625 mm; helical pitch = 1.173, 120 kVp, 120 effective mAs, section thickness/interval = 3/3 mm. Abdominal surgery CT protocols included triple-phase dynamic CT. Unenhanced scans were obtained, followed by arterial-, portal-, and delayed-phase scans using a 19-s delay after the attenuation of the aorta at the thoracolumbar junction had reached 150 HU (arterial phase), a fixed 55-s delay (portal phase) and a 275-s delay (delayed phase) after an intravenous injection of 120 ml of iohexol (Omnipaque, GE Healthcare) administered at a rate of 3 ml/s with an autonomic injector. Abdominal pelvic CT protocols included unenhanced scans and single portal-phase scans using a fixed 70-s delay after an intravenous injection of 130 ml of iobitridol (Xenetix 300, Guerbet) administered at a rate of 3 ml/s with an autonomic injector. Coronal reformatted images were created using the source CT dataset, with the slice thickness and reconstruction interval set to 3 mm.
Steps to analyze CT profiles for laparoscopic reduction of PH
Extraction of factors related to laparoscopic reduction after four surgeons reviewed all CT images.
Identification of CT characteristics through cross-checking with a radiology specialist.
Identification of five factors in a single-variable analysis of the laparoscopic reduction CT profiles.
Prediction of the possibility of laparoscopic reduction of PH using significant CT profiles.
Definitions of CT profiles for laparoscopic reduction of PH (Photo 1)
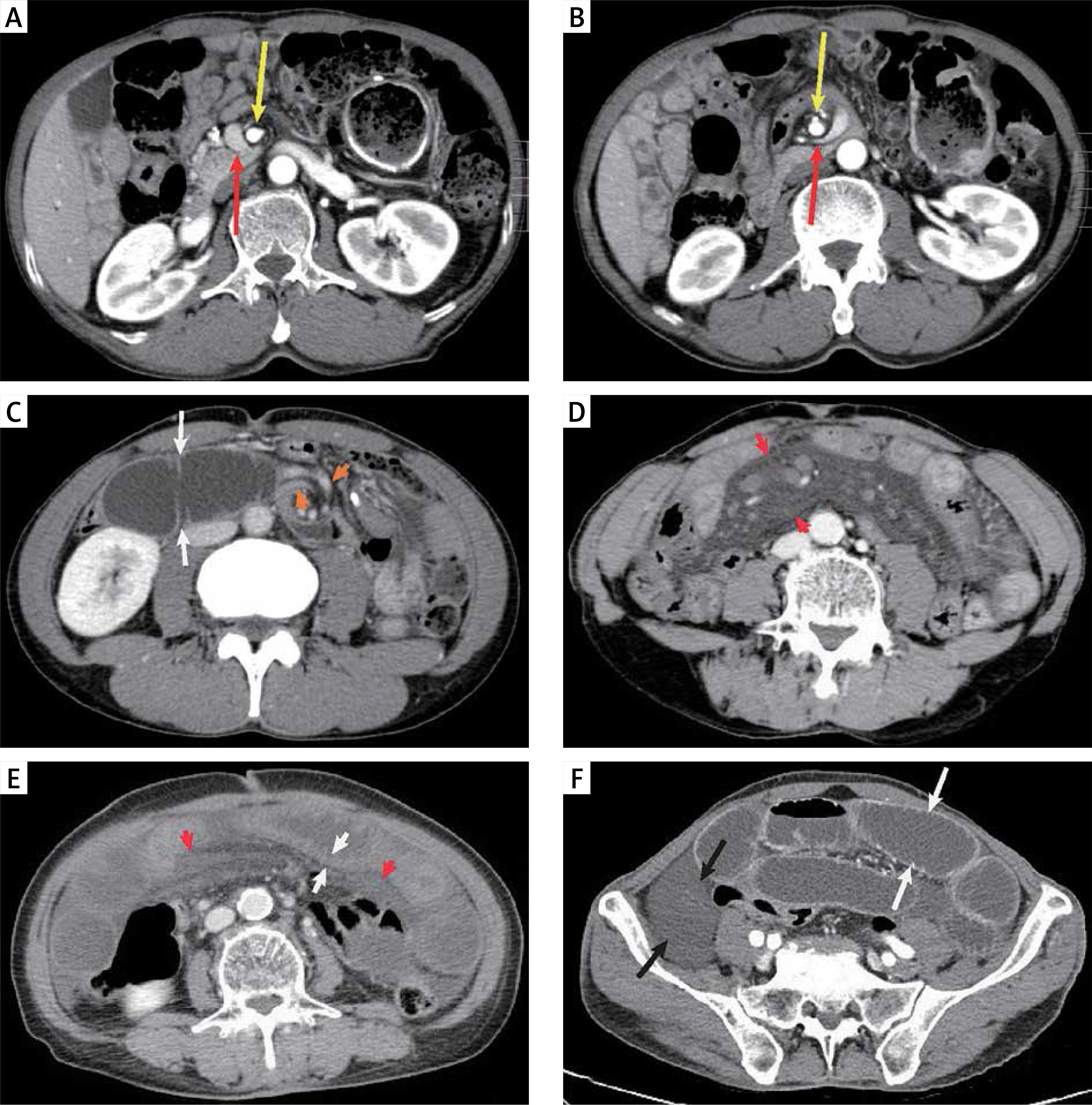
Whirl sign: An encircling of the small bowel loop and the SMV around the superior mesenteric artery (SMA) is observed [9]; the SMV (red arrows) is twisted toward the SMA (yellow arrows) in a clockwise or counterclockwise pattern (Photos 1 A, B).
Narrowing of the SMV [10]: An abrupt termination or narrowing of the proximal mesenteric vein occurs (more than 50%), with distal branch dilation; SMV collapse (red arrow in Photo 1 B) and distal branch dilation are observed (orange arrowheads in Photo 1 C).
Dilated duodenum (≥ 3 cm in diameter): The 2nd and 3rd duodenal portions (white arrow) are filled and dilated with fluid (Photo 1 C).
Mesenteric fat stranding [11]: Increased attenuation in the mesentery is observed compared with the adjacent normal mesentery due to mesenteric venous congestion. Photo 1 D shows extensive mesenteric fat stranding (red arrowheads).
Small bowel wall thickening (≥ 3 mm in diameter) [12]: Photo 1 E shows small bowel wall thickening (white arrowheads) and mesenteric fat stranding (red arrowheads).
Small bowel dilation (defined as diameter ≥ 3 cm) [6]: Photo 1 F shows small bowel dilation (white arrows), and a mean number of small bowel dilations > 3 cm was detected (white arrow) at the level of the anterior superior iliac spine (ASIS).
Intraperitoneal fluid: Fluid collection is noted in the abdominal or pelvic cavity (black arrow, Photo 1 F) [6].
Operations
Indications for laparoscopic reduction
The patients with stable vital signs with no evidence of bowel perforation or necrosis underwent emergent laparoscopic reduction surgery. A surgeon decided whether it would be possible to create a laparoscopic field due to mild to moderate abdominal distension.
Photo 1
Characteristic CT profiles of Petersen’s hernia. The proximal SMA (yellow arrow) and SMV (red arrow) were patent (A), and the distal SMA was patent, but the distal SMV (red arrow) was collapsed, as indicated by whirled mesentery (B). After whirling, the second and third duodenal portions (white arrow) were dilated and distended, the distal SMV branches were dilated (orange arrowhead) (C), and mesenteric fat stranding developed (red arrowhead, D). After SMV narrowing, the small bowel wall was thickened (white arrow), with mesenteric fat stranding (red arrowhead) in the early phase (E). In the late phase, we found small bowel dilation (white arrow) and intraperitoneal fluid (F)
Laparoscopic reduction
The first trocar was inserted by an open method with a new incision at the level of the lower abdomen. Commonly, three or four trocars were used for laparoscopic reduction. The intra-abdominal reduction process was the same as in the open method with laparoscopic closure of the herniated Petersen’s space with nonabsorbable sutures at the final step. Careful handling of the herniated small bowel was essential because of the high possibility of bowel injury during laparoscopic reduction. If it became difficult to implement laparoscopy, for example, if severe intra-abdominal adhesions interfered with creating a pneumoperitoneum, if the laparoscopic field of view was insufficient due to excessive obstructed bowel dilation, or if the bowel or mesentery was fragile due to severe edema or bowel necrosis, we conducted conversion to open reduction immediately.
Statistical analysis
We used SPSS Statistics version 24 (IBM SPSS, Inc., Chicago, IL, USA) for statistical analysis. Continuous data were compared using Student’s t-test and are presented as the means ± standard deviations, and noncontinuous variables were assessed with the χ2 test. In all analyses, p-values less than 0.05 were considered statistically significant. A binary logistic regression model was used for univariate and multivariate analyses.
Results
Patient demographics
We found 40 PH patients with a history of gastrectomy who underwent reduction surgery between 2015 and 2018. Figure 1 shows the patient flow diagram. We excluded 3 patients due to a history of open gastrectomy. Among 37 patients, 27 underwent gastrectomy before 2015, and 10 underwent gastrectomy between 2015 and 2018. The incidence of PH was 0.4% (10/2417) among gastrectomy patients from 2015 to 2018 (n = 2417), and the incidence of PH among GJ or esophagojejunostomy (EJ) patients was 1.3% (10/758).
Thirty-seven patients with a history of laparoscopic gastrectomy developed PH and underwent surgery, and 9 patients were excluded because the surgeon had no experience with laparoscopic hernia reduction. Therefore, there were 28 PH patients with a history of laparoscopic gastrectomy eligible for analysis. We compared the laparoscopic group (n = 15) and the open reduction groups (n = 13, 3 open conversion + 10 open cases).
Table I shows the demographics of the patients. The average patient age was 62.0 ±11.8 years. The male-to-female ratio was approximately 6 : 1. Analysis of the TNM stages revealed stage I, stage II and unknown stage in 64.3% (n = 18), 21.4% (n = 6) and 14.2% (n = 4) of patients, respectively. Among the types of previous operations, DG with B-II was the most common procedure (39.3%, n = 11), followed by total gastrectomy with RNY EJ (RNY-EJ, 25%, n = 2), DG with RNY GJ (RNY-GJ, 7.1%, n = 2), DG with uncut RNY-GJ (12.0%, n = 9), proximal gastrectomy with double tract reconstruction (7.1%, n = 2), and 2 unknown procedures due to the previous operations being performed at different hospitals. The mean period between the previous operation and the hernia reduction operation was 26.2 ±27.4 months.
Table I
Patients’ demographics
| Factors | Value |
|---|---|
| Age [years] | 62.0 ±11.8 |
| Sex: | |
| Male | 24 (85.7%) |
| Female | 4 (14.3%) |
| TNM stage of gastric cancer*: | |
| I | 18 (64.3%) |
| II | 6 (21.4%) |
| Unknown | 4 (14.2%) |
| Previous operation: | |
| TG with RNY-EJ | 7 (25%) |
| DG with B II | 11 (39.3%) |
| DG with RNY-GJ | 2 (7.1%) |
| DG with uncut RNY-GJ | 4 (14.3%) |
| PG with double tract | 2 (7.1%) |
| Unknown | 2 (7.1%) |
| Petersen’s space repair: | |
| No | 20 (71.4%) |
| Yes | 1 (3.6%) |
| Unknown | 7 (25%) |
| Periods between previous operation [months] | 26.2 ±27.4 |
| Time from pain to hernia operation [h] | 20.7 ±20.6 |
| Approach method: | |
| Open reduction | 10 (35.7%) |
| Laparoscopic reduction | 15 (53.6%) |
| Open conversion of laparoscopic reduction | 3 (10.7%) |
| Operation time [min] | 81.5 ±25.6 |
| Small bowel injury during reduction | 3 (10.7%) |
Regarding the operative information, there was 1 case of previous Petersen’s space closure, 20 cases of no repair and 7 cases of unknown repair due to the previous operation being performed at a different hospital. The time between abdominal pain and the hernia operation was 20.7 ±20.6 h. Regarding the approach, laparoscopic reduction, open reduction, and open conversion were performed in 53.6% (n = 15), 35.7% (n = 10), and 10.7% (n = 3) of patients, respectively. The causes of open conversion from laparoscopic reduction were small bowel and mesentery thickening with severe congestion (n = 1) and difficulty in creating a secure intra-abdominal field via pneumoperitoneum due to excessive small intestine dilation (n = 2). There were 3 cases of small bowel injury during reduction. The mean operation time for reduction was 81.5 ±25.6 min. The mean duration of postoperative hospital stay was 10.8 ±7.6 days. There were 2 cases of mortality due to sepsis with multiorgan failure.
Clinical characteristics in the laparoscopic and open reduction groups
Comparing the laparoscopic and open groups, we found that patients in the laparoscopic group (55.7 ±10.4 years) were younger than those in the open group (69.3 ±9.1 years, p = 0.001, Table II). However, there were no differences between the two groups in terms of sex, initial symptoms, time since previous operation, TNM stage, previous closure of Petersen’s space, time between pain and hernia operation, operation method, or inflammatory laboratory findings (e.g., white blood cell count, erythrocyte sedimentation rate, C-reactive protein level).
Table II
Clinicopathologic comparison between laparoscopic reduction group (Laparo group) and open reduction group (Open group)
| Factors | Laparo group (n = 15) | Open group (n = 13) | P-value |
|---|---|---|---|
| Age [years] | 55.7 ±10.4 | 69.3 ±9.1 | 0.001 |
| Sex: | |||
| Male | 13 | 11 | 1.0 |
| Female | 2 | 2 | |
| Initial symptom: | |||
| Nausea | 6 | 5 | 0.70 |
| Vomiting | 14 | 12 | 1.0 |
| Pain | 0 | 2 | 1.0 |
| Periods between previous operation [months] | 25.4 ±20.2 | 27.3 ±36.1 | 0.86 |
| TNM stage of gastric cancer*: | |||
| I | 10 | 8 | 0.22 |
| II | 5 | 1 | |
| Unknown | 0 | 4 | |
| Previous closure of Petersen’s space: | |||
| No | 12 | 8 | 0.33 |
| Yes | 0 | 1 | |
| Unknown | 3 | 4 | |
| Time from pain to hernia operation [h] | 22.4 ±23.0 | 18.9 ±18.8 | 0.67 |
| Previous operation: | |||
| TG with RNY EJ | 4 | 3 | 0.48 |
| DG with B II | 7 | 4 | |
| DG with RNY | 1 | 1 | |
| DG with uncut RNY | 3 | 1 | |
| PG with double tract | 0 | 2 | |
| Unknown | 0 | 2 | |
| Postoperative small bowel obstruction | 1 | 0 | 1.0 |
| Laboratory: | |||
| WBC | 8,971 ±2,794 | 11,565 ±6,049 | 0.09 |
| ESR | 16.3 ±13.9 | 31.8 ±34.1 | 0.23 |
| CRP | 0.7 ±1.1 | 6.4 ±11.7 | 0.12 |
Comparison of CT profiles between the laparoscopic and open reduction groups
We found that all patients in the open and laparoscopic groups showed whirling signs (p = 1.0) (Table III, Photos 1 A, B). All patients (100%) in the open group and 20% patients in the laparoscopic group showed SMV narrowing (p = 0.02, Table III, Photos 1 A, B). There was no difference in duodenal dilation (open/laparoscopic, 7.7%/40%, p = 0.90) (Photo 1 C, white arrow), mesentery fat stranding (open/laparoscopic, 69.2%/33.3%, p = 0.32) (Photo 1 D, white arrow) or small bowel wall thickening (open/laparoscopic, 76.9%/40%, p = 0.32) (Photo 1 E, white arrow) between the two groups.
Table III
Comparison of laparoscopic reduction CT profile betweenl reduction group (Laparo group) and open reduction group (Open group)
Small bowel dilation was observed in 92.3% (12/13) of patients in the open group and 13.3% (2/15) of patients in the laparoscopic group (p = 0.01) (Photo 1 F, white arrow). The mean numbers of small bowel dilations (more than 3 cm) were 0.1 ±0.3 in the laparoscopic group and 5.3 ±2.2 in the open group at the ASIS level (p < 0.001). There was no difference in intraperitoneal fluid (open/laparoscopic, 69.2%/33.3%, p = 0.29) (Photo 1 F, black arrow) between the two groups.
On univariate analysis by the binary logistic regression model, narrowing of the SMV and small bowel dilation were significant CT profiles (p < 0.05, Table IV). On multivariate analysis, small bowel dilatation was an independent factor of the laparoscopic approach for PH reduction (p = 0.01).
Table IV
Multivariate analysis of significant CT profiles for patients who received laparoscopic reduction for Petersen’s hernia
| CT finding | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| P-value | P-value | Odds ratio | 95% confidence interval | |
| Narrowing of SMV | 0.02 | 0.70 | ||
| Small bowel dilatation (> 3 cm, at ASIS level) | 0.01 | 0.01 | 0.16 | 0.03–0.74 |
Discussion
The aim of this study was to identify objective predictors of patient suitability for laparoscopic emergent surgery by a comparative analysis between PH patients treated by laparoscopic and open reduction. We found that among the eight CT profiles, small bowel dilatation was the most important CT profile for identifying PH patients contraindicated for laparoscopic reduction.
PH is a rare disease, and the incidence of PH has been reported to be 0.4–9%, especially after laparoscopic RNY anastomosis [3, 13–17]. Kang et al. reported that they experienced only 27 cases of PH among 6474 patients who underwent gastrectomy for gastric cancer [15]. In our study, the incidence of PH in patients who underwent laparoscopic gastrectomy with EJ or GJ was 1.3% (10/758). We also added 18 patients who underwent laparoscopic gastrectomy before 2015. We analyzed a total of 28 cases from 4 institutions, which is not a small number of cases compared with other reports on PH. When deciding on the surgical approach for PH, surgeons use clinical signs, including physical findings, vital signs, laboratory data, and CT profiles, as important objective criteria. Even when laparoscopic surgery has been selected, these clinical signs are integrated. Therefore, we conducted this analysis to examine which patients are suitable for laparoscopic surgery.
In the current study, clinical data, except for patient age, did not differ between the laparoscopic and open reduction groups. Consequently, we searched for objective indicators for the laparoscopic approach. CT profiles were thought to be very useful in determining whether to perform open or laparoscopic surgery for PH. The hypothetical processes of PH that can be identified on CT are as follows: (1) duodenal dilation indicated by whirled mesentery; (2) SMV narrowing; (3) mesenteric fat stranding due to venous congestion; (4) small bowel wall thickening due to venous congestion; (5) small bowel dilation; (6) intraperitoneal fluid collection; and (7) strangulation of the small bowel. We investigated under which conditions laparoscopic reduction could be possible.
If PH occurs with symptoms, such as abdominal pain, emergent reduction surgery should be performed as soon as possible using an open or laparoscopic approach. Laparoscopic surgery has several advantages over open surgery. Laparoscopic gastrectomy for gastric cancer has shown benefits over open surgery in terms of better cosmetic outcomes, lower complication rates, faster recovery, and less pain [18]. The advantages of laparoscopic surgery for the treatment of PH have not been reported; however, they are expected to be similar to those of laparoscopic gastrectomy. Therefore, we believe that the laparoscopic approach can enhance patient recovery. However, there is also a possibility of intestinal injury during the insertion of trocars or the reduction of edematous dilated intestine. In the current study, therefore, it was impossible to apply laparoscopic reduction surgery in all PH patients.
There are many ways to detect PH, the most obvious of which is CT. Yamashita et al. reported the typical diagnostic CT profiles of PH to differentiate it from other internal hernias in patients who have undergone gastrectomy with RNY gastric bypass [19]. They confirmed that CT is useful to detect PH and found that the hooking intestine sign might also be useful for diagnosing PH on CT. Additionally, other researchers have reported that CT can used to precisely diagnose internal hernia after surgery [20]. They analyzed the detailed findings from abdominal CT scans evaluated by radiologists and reported a maximum sensitivity of 85.0% and a maximum specificity of 94.8%. However, it was not easy to use CT profiles as objective operative indicators of PH due to a lack of sufficient evidence, especially regarding mesenteric and bowel edema. Additionally, the indications for open reduction or open conversion were not only CT profiles but also signs of shock. It is not easy to extract definite parameters to indicate the approach, but we attempted to extract such parameters from CT profiles. We performed a multivariate analysis of the CT profiles, which suggested that small bowel dilatation was the most significant factor for laparoscopic reduction surgery.
There were some limitations to our study. First, this was a retrospective analysis. Second, there were a small number of PH reduction procedures, especially open reduction procedures. Third, there is a risk of bias due to the subjective decision of the surgeon regarding the use of a laparoscopic or an open approach. Fourth, the assessments of the CT scans were subjective, including the identification of CT characteristics. However, this is the first report of an analysis of laparoscopic reduction of PH.
Conclusions
We found that small bowel dilatation is the most important CT profile for identifying PH patients contraindicated for laparoscopic reduction. Despite the retrospective design of this study, these CT profiles are expected to define the scope of laparoscopic reduction in PH patients and to establish indications for the laparoscopic approach.