








Introduction
Percutaneous lumbar discectomy (PLD) is a minimally invasive procedure for the treatment of intervertebral disc protrusion. It has been extensively applied for the treatment of lumbar disk herniation. External drainage (ED) is used for the drainage of abscesses of various organs. In clinical practice, intervertebral disc infection with epidural abscess is considered as an indication for surgery. So, PLD combined with ED for the treatment of intervertebral disc infection with epidural abscess is rarely reported. As an attempt, we adopted combined miniinvasive treatment to treat successfully 12 cases of patient with intervertebral disc infection with epidural abscess.
Aim
The aim of this study was to discuss the feasibility, safety and efficacy of PLD and ED for the treatment of intervertebral disc infection with epidural abscess.
Material and methods
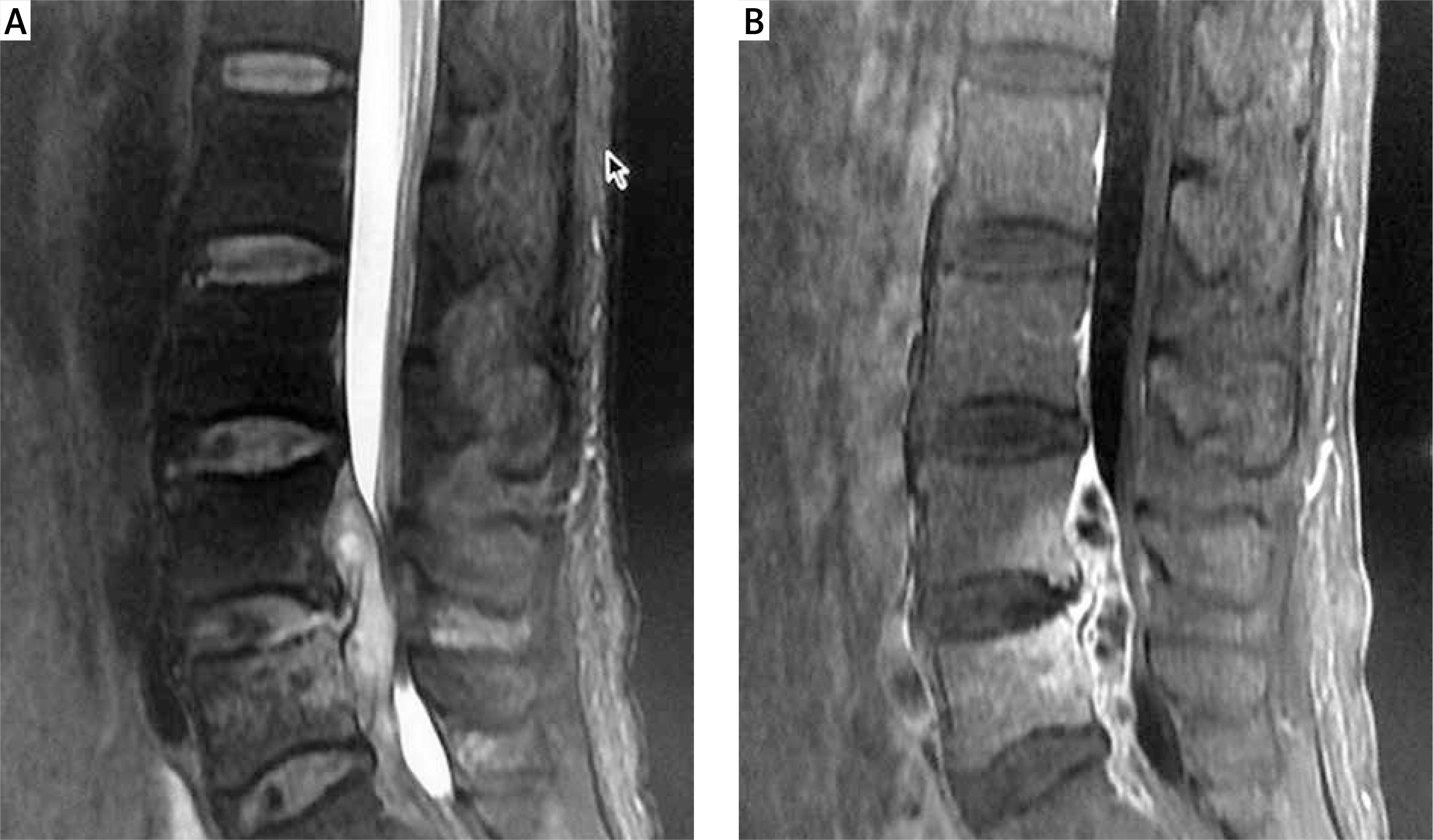
Hospital ethics board human ethics approval was obtained prior to the initiation of this trial. We collected 12 cases of patients with intervertebral disc infection with epidural abscess who underwent PLD combined with ED between June 2010 and June 2012 in our department (Table I): 6 male cases (n = 6), 6 female cases (n = 6). The average age was 58.3 ±1.2 years. The enrolled patients were required to meet the following conditions: 1) they all showed the corresponding clinical symptoms and signs; 2) the symptoms had not been relieved or aggravated after conservative therapy; 3) intervertebral disc infections with epidural abscess were suggested on computed tomography (CT) and magnetic resonance imaging (MRI) preoperatively; 4) the range of abscess was no more than three vertebral bodies (Photo 1).
Table I
Information of patients
Photo 1
Non-enhanced Sagittal. A – T2-Weighted-MRI shows a fusiformis hyperintensity can be seen in the spinal dura involving the L5 vertebral and the intervertebral disk at the L4-L5 levels. The spinal canal is stenosis. Enhanced sagittal. B – T1-weighted MRI demonstrates a fusiformis abnormal signal was enhancement inhomogeneous
Apparatus and equipment
Bard Truguide Coaxial Biopsy Needle (Bard Peripheral Vascular, Inc USA), working cannulas (Dragon-Crown, Jinan, China) penultimate cannula (Dragon-Crown, Jinan, China), a marrow nucleus rongeur (Dragon-Crown); guide wire (COOK, American); external drainage catheters (COOK, American); DSA (Axiom Artis dra, Simmens, Germany), 3.0 T MRI (GE HDxt-3T, GE American) 64 Row CT (Toshiba Aquilion).
Index of efficacy
The clinical efficacy was evaluated by the standard Macnab’s evaluation [1] and visual analog scale (VAS) scores. The pain intensity is evaluated by VAS (0–10; 0 represent no pain; 10 represents the worst pain). Improvement in Macnab’s evaluation standard was divided into four grade. Excellent: No pain, no restriction of mobility, return to normal work and level of activity. Good: Occasional non-radicular pain, relief of presenting symptoms, able to return to modified work. Fair: Some improved functional capacity, still handicapped and/or employed. Poor: Continued objective symptoms of root involvement, additional operative invention needed at index level irrespective of length of postoperative follow-up. Postoperation CT (Toshiba Aquilion, Japan) and MRI (GE HDxt-3T, GE, American) of vertebrae was examined.
Procedure
Informed consent for participation in this study was obtained from the patient. A lateral position was required during the course of the operation under the guidance of the Digital subtraction angiography (DSA, Axiom Artis dra, Simmens, Germany). The patient’s back skin was sterilized, and local anesthesia was applied on the puncture route. After administration of local anesthetic (2% lidocaine), a small incision was made with a scalpel blade. With continuous fluoroscopic monitoring, a 15-G Bard Truguide Coaxial Biopsy Needle (Bard Peripheral Vascular, Inc USA) was inserted at the site of the anterior part of the L4-5 intervertebral disc, followed by sequential dilation of the tract with working cannulas (Dragon-Crown Co, Jinan, China) until the last working cannula (5 mm in diameter) reached the anterior portion of the L4-5 intervertebral disc. After removal of the penultimate cannula (Dragon-Crown, China), a marrow nucleus rongeur (Dragon-Crown, China) was inserted into the intervertebral disc through the last working cannula and the purulent materials and marrow tissues were extracted slowly, as much as possible (Photo 2). Then a 0.035 inch guide wire (COOK, American) was inserted through the work cannula (Photo 3). Two 8.5 Fr external drainage catheters (COOK, American) were inserted into the intervertebral disc through the guide wire (Photo 4). After the operation, one external drainage catheter (COOK, American) was used for irrigating saline and another external drainage catheter (COOK, American) was connected to a drainage pack, which was maintained all the time. The input and output were recorded every day. Meanwhile, systematic antibiotic therapy was also administered. Postoperation CT (Toshiba Aquilion, Japan) and MRI (GE HDxt-3T, GE, American) of vertebrae was examined.



Results
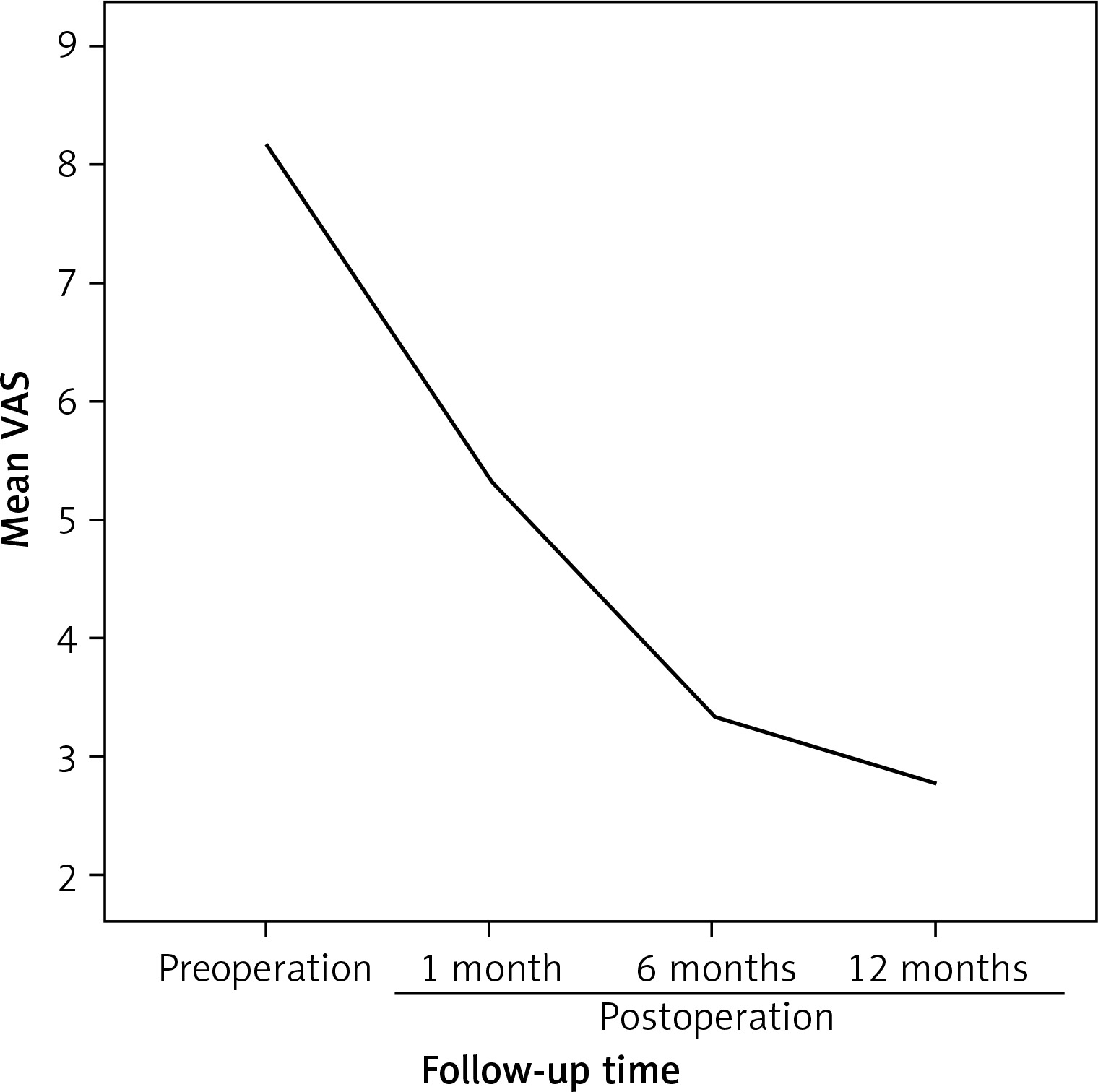
The basic information of patients is shown in Table I. The ages of patients (male 6, female 6) ranged from 47 to 75 years, with a median 58 years. The operation technical success rate was 100%. Preoperation mean VAS score was 8.18 ±0.98; 5.36 ±1.50 postoperation 1 month; 3.36 ±2.24 postoperation 6 months; 2.77 ±0.31 postoperation 12 months. The comparison of preoperation and postoperation VAS showed a significant difference (all p < 0.05). According to standard Macnab’s evaluation, postoperation 12 months, of all 12 cases – excellent 4 cases, good 7 cases, poor 1 case (Table II). No serious complications were recorded. Postoperation efficacy rate was 91.6%; only 1 case was poor. The postoperation VAS score was dramatically reduced compared with the preoperation score (Figure 1). The comparison of preoperation and postoperation VAS showed a significant difference (p < 0.05). Postoperatively the CT and MRI imaging showed that the abscess had disappeared (Photo 5) .

Discussion
Intervertebral disc infection with epidural abscess is an important problem that often requires aggressive therapy or even surgery. If the epidural abscess is not diagnosed and treated fast, the patient may suffer serious complications such as paraplegia and death [2]. The most frequently affected level was the lumbar level, followed by the thoracic and cervical levels, and lastly, the sacral level. The initial symptoms of intervertebral disc infection with epidural abscess were not specific, and the classical triad of spinal pain, fever, and neurological deficits was present in only 10–15% of patients at presentation [3]. Measurement of ESR and CPR level, together with radiological diagnostic imaging, was fundamental in the initial assessment and assessment of the patient’s response to therapy. ESR was a useful screening parameter, with a 94% sensitivity [4]. Meanwhile, MRI was the diagnostic test of choice because its sensitivity and specificity are > 90% [5].
The therapy duration for intervertebral disc infection with epidural abscess depends on the infection-causing microorganism. The recommended duration ranges from 4 weeks to 3 months [6]. Intervertebral disc infection was classified as either pyogenic or granulomatous. For patients with pyogenic infection, Staphylococcus aureus was the most common agent, being isolated in more than 50% of pyogenic spinal infections [7]. Meanwhile, granulomatous infections are mainly due to brucellosis and tuberculosis. The frequency of intervertebral disc infection in brucellosis ranges from 2% to 53% of patients [7]. The incidence rate of tuberculosis intervertebral infection was approximately 50%.
To date, conservative therapy and antibiotic therapy with bracing have been the primary methods for the treatment of intervertebral disc infection. Intervertebral disc infection with epidural abscess is an indication for surgery. Once the patient shows any neurologic deficit, surgical decompression should be considered [8]. Although the period of antibiotic therapy for epidural abscess is still being debated, it is preferable to continue treatment for at least 4 weeks, because studies have shown a 25% rate of relapse in patients who were treated for less than 4 weeks [9–11]. In patients with panspinal epidural abscess, it was impracticable to perform a classic decompressive laminectomy, and in such case less extensive surgery, such as a limited laminotomy with cranial and caudal insertion of epidural catheters for drainage and irrigation, should be considered [12]. For intervertebral disc infection with epidural abscess, surgery was the most frequently reported treatment method. Timeothy et al. [13] reported 128 cases of spinal epidural abscess that were medically managed or surgically managed in combination with medical management. They concluded that early surgery could improve neurological outcomes and that medical management failed in approximately 41% of the patients, requiring surgical decompression. Carefully selected patients can be safely managed with antibiotics alone [4]. Carpenter et al. [14] reported a case of spinal epidural abscess with discitis and vertebral osteomyelitis that was successfully treated with 6-week administration of intravenous antibiotics. Zhang et al. [15] reported a case of cervical epidural abscess with a combination of intravenous vancomycin and imipenem/cilastatin.
In the case of intervertebral disc infection, especially with epidural abscess, performing multilevel laminectomies may predispose the patient to complications such as increased blood loss, cardiac and respiratory difficulties, increased postoperative pain and recovery time, and late kyphotic deformity and instability. At present, instrumentation placement has been accepted during active spinal infection as long as debridement of decreased tissue was complete and an appropriate course of antibiotics was followed [16]. A review of the literature [17] concluded that the infection recurrence rate of spinal instrumentation in the infected spine was 1.74%.
Although intervertebral disc infection with epidural abscess was an indicator of surgery, we used a marrow nucleus rongeur to remove the infected disc material and epidural abscess through the posterior approach and then inserted two external drainage catheters in the intervertebral disc, because the PLD combined with ED was minimally invasive and easy to perform, with little trauma and lower risk for complications compared with surgery. To our knowledge, PLD combined with ED for the treatment of intervertebral disc infections with epidural abscess has rarely been reported. Lyu et al. [18] reported a case of spinal epidural abscess that was treated with percutaneous, computed tomography-guided, needle aspiration and parenteral antibiotic therapy. In this study, we used PLD combined with ED to treat an intervertebral disc infection with epidural abscess and obtained satisfactory results that were similar to those of surgery decompression. Postoperatively the VAS score was dramatically reduced and the pain was relieved. The efficacy was 96.1%; only 1 case result was poor. To our excitement, no serious complications occurred. Compared with surgery, PLD combined with ED does not alter the spinal structure and stability, and it could accelerate the drainage of infectious materials compared with the use of IV antibiotics alone.
Our study had some limitations. Firstly, the number of patients treated by PLD combined with ED was relatively small, which may mask the advantage or disadvantage of the procedure. Secondly, lacking a control group, the clinical efficacy of PLD combined with ED for the treatment of intervertebral disc infection with epidural abscess was not proved to have an advantage over single surgery. So, further research will be carried out in the future.