








Introduction
In recent years, with the acceleration of population aging, the incidence of lung cancer in the elderly is increasing annually [1]. The elderly are often burdened by multiple organ dysfunction, underlying diseases, and low immunity, which increases the risk of complications of traditional lung cancer surgery [2, 3]. Currently, uniportal video-assisted thoracoscopic surgery (VATS) is being increasingly used in thoracic surgery. Compared with traditional multi-portal surgery, uniportal VATS has achieved the quintessential level in minimally invasive incisions and is gradually accepted by more and more thoracic surgeons, especially young physicians [4, 5]. However, the literature regarding the application of uniportal video-assisted thoracoscopic segmental resection of the lung in patients aged over 65 years with non-small cell lung cancer (NSCLC) is sparse. This paper reports 175 cases of uniportal video-assisted thoracoscopic segmental resection of the lung performed at the center, of which 63 patients were over 65 years old.
Aim
To investigate the safety and feasibility of uniportal video-assisted thoracoscopic segmental resection of the lung in elderly patients aged over 65 years with NSCLC.
Material and methods
Research objects
A retrospective analysis of 175 NSCLC patients who underwent uniport video-assisted thoracoscopic segmental resection of the lung in the center from August 2018 to August 2020 was conducted, and patients were divided into two groups according to their age. A total of 175 patients were divided into two groups according to age. Among them, 63 patients were divided into the elderly group because they were 65 years old or older, and the other 112 patients aged less than 65 were in the non-elderly group. There were 28 males and 35 females in the elderly group, and 44 males and 68 females in the non-elderly group.
Ethics statement
The study was conducted in accordance with the principles of the Declaration of Helsinki, and the study protocol was approved by the ethics committee of our hospital (register number: 2020(036)). All patients signed informed consent and were informed that their data would be used for study purposes.
Inclusion criteria
(1) Preoperative computed tomography (CT) revealed pure ground-glass nodules (GGN) or mixed ground-glass nodules (mixed GGN), and the solid component of mixed GGN was < 50%. (2) Tumor size was < 2 cm, and the postoperative staging was T1N0M0 peripheral NSCLC. (3) Wedge resection could not be performed or wedge resection margin distance was not > 2 cm for GGN.
Surgical methods
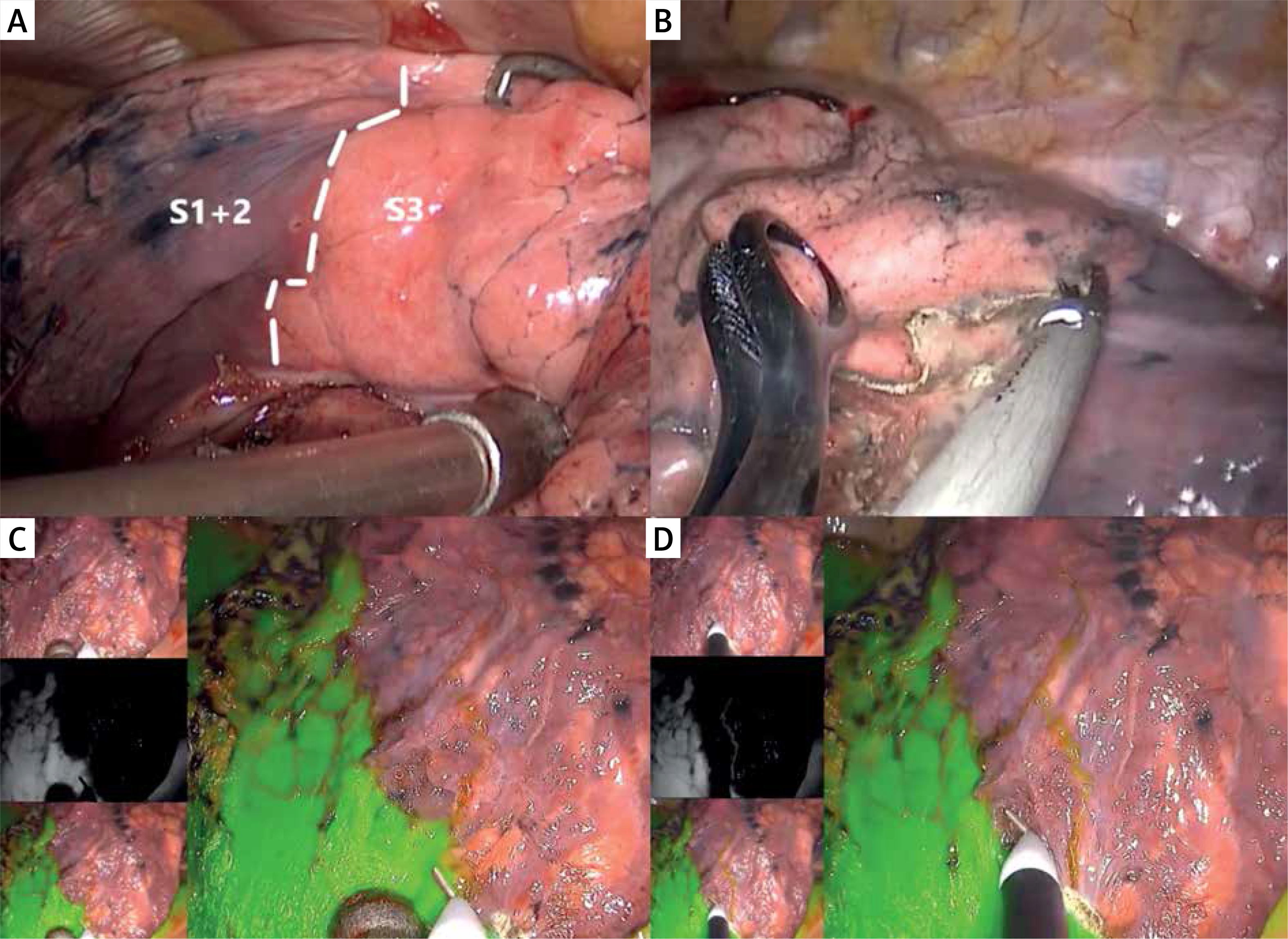
Conventional preoperative ZiWeiDiXing interactive medical image control system (ZWDX, China) was used to convert two-dimensional (2D) lung CT images into three-dimensional (3D) images, and the bronchi and blood vessels in the lung segment where pulmonary nodules were located were studied for the best surgical planning (Photo 1). Under intravenous-inhalation combined anesthesia, the patients were intubated with a double-lumen endotracheal tube and maintained in the 90° decubitus position on the healthy side. In the 4th or 5th intercostal space, a single incision with the length of 3 cm was made between the anterior axillary line and midaxillary line. The incision protective cover, the video camera of the thoracoscopy, and all surgical instruments were placed in the incision. First, the condition of the diseased lung was examined to determine the location of the pulmonary nodules and lung segment to be resected. According to the preoperative 3D images, the target segmental pulmonary artery, segmental pulmonary vein and bronchus were dissociated and processed. To determine the boundary between the lung segments, the inflation-deflation method was used for the majority of patients, and the anesthesiologist was asked to use pure oxygen low pressure ventilation to expand the lung. The boundaries between segments could be displayed after about 10 min (Photos 2 A, B). According to the CT findings, the indocyanine green (ICG) reverse staining method was used to determine the boundary between the lung segments for patients preoperatively diagnosed with emphysema. At this time, the thoracoscopy system was changed to fluorescence mode, and patients were injected with 25 mg of ICG via the peripheral vein. After ICG reached the lung tissue through the pulmonary artery, the target segment to be resected did not display color, whereas the remaining lung tissue showed green color, forming a clear boundary on the surface of the lung. Electrocautery was used to label the intersegmental plane, and then the thoracoscopy exited fluorescence mode (Photos 2 C, D). Finally, the target lung segment was resected. An endoscopic stapler can be used to deal with the intersegmental fissure, segmental bronchus, and thicker segmental pulmonary vessels. Ultrasonic knife, ham-o-loc, or silk thread ligation can be used for the pulmonary arteriole. After rapid frozen pathology of the resected lesion, the mediastinal lymph nodes should only be sampled when the result shows adenocarcinoma in situ or microinfiltrative adenocarcinoma, or mediastinal lymph node dissection is required systematically when the result shows infiltrative adenocarcinoma. In general, the lymph nodes in groups 4–12 were dissected in the left lung, while those in groups 2, 3, 4, 7–12 were dissected in the right lung, and the recurrent laryngeal nerve was protected. When suturing the incision, two sutures were drawn from the sutured muscle layer to fix the thoracic drainage tube. The fishbone suture of Johnson & Johnson was used for the intradermal suturing of the skin layer.

Statistical analysis
Continuous data were expressed as the mean ± standard deviation (SD). Significance between the two groups was determined by the χ2 test or Student’s t-test. Fisher’s exact test was used instead if cell frequencies less than 5 were expected. All statistical analyses were carried out using SPSS Statistics, version 24.0 (IBM, Armonk, NY, USA), and p < 0.05 was considered significant.
Results
The operations of all patients were completed without death or conversion to open surgery. In Table I, the general perioperative data of the two groups of patients are listed and statistically analyzed. There were no statistically significant differences in gender, occupational type, body mass index (BMI), postoperative pathological type, family history, smoking history, or the prevalence of coronary heart disease between the two groups (p > 0.05). The prevalence of emphysema in the elderly group was significantly higher compared to that in the non-elderly group, and the difference between the two groups was statistically significant (p = 0.001). Moreover, the prevalence of hypertension and diabetes in the elderly group was also higher compared to that in the non-elderly group; the difference between the two groups was statistically significant (p < 0.05).
Table I
Baseline characteristics data before operation
| Parameter | Elderly group (n = 63) | Non-elderly group (n = 112) | P-value |
|---|---|---|---|
| Sex: | 0.506 | ||
| Male | 28 | 44 | |
| Female | 35 | 68 | |
| Family history | 6 | 14 | 0.553 |
| Smoking history | 13 | 24 | 0.875 |
| Emphysema | 11 | 3 | 0.001a |
| Hypertension | 20 | 11 | 0.000 |
| Diabetes | 14 | 10 | 0.014 |
| Coronary heart disease | 6 | 4 | 0.103a |
| Occupation: | 0.743 | ||
| Manual workers | 31 | 58 | |
| Mental workers | 32 | 54 | |
| BMI [kg/m2]: | 0.870 | ||
| < 24 | 34 | 59 | |
| ≥ 24 | 29 | 53 | |
| Pathological type: | 0.830 | ||
| Adenocarcinoma in situ | 21 | 40 | |
| Microinvasive adenocarcinoma | 16 | 31 | |
| Invasive adenocarcinoma | 26 | 41 |
Table II shows the lung segments resected in the two groups of patients. In the elderly group, except for LS4, LS10, RS4, RS5, and RS10, all other lung segments were resected, including complex combined segmental resection of the lung for LS8+9, LS9+10, RS8+9, and RS9+10. The lung segment with the highest resection rate in the elderly group was LS6 (11 cases), RS6 (10 cases), and LS1+2 (10 cases). In the non-elderly group, resection of all segments of the lung except RS5 was performed, including complex combined segmental resection of the lung for LS8+9, LS9+10, RS8+9, and RS9+10. Compared to the elderly group, the lung segments with the highest resection rate in this group were LS1+2 (22 cases), RS6 (16 cases), and LS6 (15 cases).
Table II
Resected lung segments of the two groups
| Left | Elderly group | Non-elderly group | Right | Elderly group | Non-elderly group |
|---|---|---|---|---|---|
| LS1+2 | 10 | 22 | RS1 | 4 | 6 |
| LS3 | 2 | 2 | RS2 | 5 | 12 |
| LS4 | 0 | 2 | RS3 | 2 | 2 |
| LS5 | 1 | 3 | RS4 | 0 | 2 |
| LS6 | 11 | 15 | RS5 | 0 | 0 |
| LS8 | 3 | 6 | RS6 | 10 | 16 |
| LS9 | 1 | 2 | RS8 | 3 | 2 |
| LS10 | 0 | 2 | RS9 | 1 | 2 |
| LS8+9 | 2 | 4 | RS10 | 1 | 2 |
| LS9+10 | 3 | 3 | RS8+9 | 3 | 3 |
| RS9+10 | 1 | 3 |
The perioperative observation indicators and related complications of the two groups are listed in Table III and statistically analyzed. Perioperative observation indicators include: surgery time, intraoperative blood loss, retention time of thoracic drainage tube, postoperative hospital stay, and patient satisfaction with the incision. There was no statistically significant difference in these observation indicators between the two groups (p > 0.05). It is noteworthy that uniportal video-assisted thoracoscopic segmental resection of the lung was performed for all patients in the two groups, without conversion to open surgery. The postoperative complications counted included pulmonary infection, alveolar leakage, arrhythmia, pulmonary embolism, incision infection, fever, and dyspnea, and the differences in these complications between the two groups were not statistically significant (p > 0.05).
Table III
Postoperative complications and early surgical effect
| Parameter | Elderly group (n = 63) | Non-elderly group (n = 112) | P-value |
|---|---|---|---|
| Surgical time [min] | 144.57 ±21. 14 | 153.34 ±18.65 | 0.405 |
| Blood loss [ml] | 119.18 ±53.57 | 126.67 ±56.21 | 0.367 |
| Conversion to thoracotomy | 0 | 0 | |
| Tube retention time [days] | 2.37 ±1.37 | 2.12 ±1.42 | 0.421 |
| Hospital stay after surgery [days] | 3.75 ±1.40 | 3.50 ±1. 17 | 0.752 |
| Satisfaction with incision: | 0.786a | ||
| Satisfactory | 59 | 106 | |
| Unsatisfactory | 4 | 6 | |
| Complications: | |||
| Pulmonary infection | 3 | 4 | 0.700a |
| Pulmonary air leakage | 5 | 8 | 0.848 |
| Arrhythmia | 4 | 6 | 0.786 |
| Pulmonary embolism | 1 | 0 | 0.360a |
| Incision infection | 0 | 0 | |
| Fever | 7 | 13 | 0.865 |
| Dyspnea | 2 | 3 | 0.851a |
Discussion
Standard VATS lobectomy is performed with a greater risk for elderly patients with lung cancer who are often complicated with extrapulmonary underlying diseases, multiple organ dysfunction, and slow postoperative recovery, particularly for those with poor cardiopulmonary function, where the clinical application is limited [6, 7]. In recent years, it has been reported that the sublobar resection in elderly patients with NSCLC can achieve similar effects as lobectomy [8]. Some researchers even proposed that the recent clinical efficacy of VATS sublobar resection in the treatment of elderly patients with NSCLC deserved greater acknowledgment, and recommended it as the clinically preferred surgical method [9, 10]. Therefore, uniportal VATS segmental resection of the lung was performed for patients with lung cancer aged over 65 years with GGN on CT.
Uniportal VATS has the advantages of small trauma, esthetic wound, and only a single incision [5, 11], with the most commonly used being the intercostal incision. The intercostal incision is usually located between the anterior axillary line and midaxillary line, between the 4th or 5th intercostal space, with a length of about 3 cm. The experience of our center is, when the incision is closer to the midaxillary line, it is more convenient for the surgeon to dissect the hilar structure and mediastinal lymph nodes; however, the linear cutting suture device is more difficult to place, making the surgical technique more complex for the surgeon. If the incision is more forward, the intercostal space will be slightly wider, farther from the hilum. Other thoracoscopic incisions have also been reported clinically. In 2017, Stamenovic et al. reported 20 cases of uniportal video-assisted thoracoscopic lobe resection and segmental resection of the lung from the back approach [12]. The incisions of these procedures were located at the 6th intercostal “triangle of auscultation” of the back, with a length of 3.5–4.5 cm. This incision was more beneficial for the exposure of the dorsal bronchus and blood vessels, it was easier to dissect the corresponding mediastinal lymph nodes, and the incision location was more hidden. In 2018, Shen et al. reported a case of uniportal video-assisted thoracoscopic right upper lobectomy through an axillary incision parallel to the skin fold and about 4 cm in length, which was highly esthetic [13]. Compared with the traditional surgery, uniportal VATS reduces the huge damage to the chest wall of elderly patients, effectively shortens the patient’s postoperative recovery time, reduces the risk of complications, and improves the esthetics of traditional incisions [14–16]. In this study, a method with improved sutured incisions and a fixed thoracic drainage tube was used (Photo 3 A), which made the surgical incision esthetic after removing the thoracic drainage tube (Photo 3 B). The incision satisfaction of patients in both groups reached a high level, and there was no statistically significant difference between the two groups (93.7% vs. 94.6%, p = 0.786).
Photo 3
A novel method of suturing incision. A – After the operation, the incision was sutured with fishbone suture and the thoracic drainage tube was fixed. B – The wound healing of the patient was reexamined 3 months later

In uniportal video-assisted thoracoscopic segmental resection of the lung, it is difficult to master the technique due to the variation of anatomical structure of the lung segments among different individuals [16, 17]. Due to the variation of the pulmonary vessels, beginners may transect the artery, adjacent to the lung segment, resulting in no blood supply to the lung tissue [18, 19]. It is inaccurate to determine the intersegmental boundary by using the inflation-deflation method. If the pulmonary artery of the target pulmonary segment is not completely transected, the intersegmental boundary is also inaccurate, and the hilum cannot be lifted, causing some lung segment tissues, which should be retained, to be resected [20]. Moreover, if the pulmonary veins that are not part of the target lung segment are transected, it will cause venous return disorder, postoperative hemoptysis, and a second operation is required for lobectomy in severe cases [21]. If the pulmonary vein of the target lung segment is not completely transected, misjudgment will occur when judging the intersegmental boundary based on the intersegmental veins, and the lung tissue that should have been resected may be retained [22, 23]. The experience is that preoperative MIMICS is used to convert 2D CT images into 3D images to accurately determine the vessels and bronchi of the target lung segment and guide the surgeon to perform the surgery.
In general, a simple inflation-deflation method is used to determine the intersegmental boundary of segmental resection of the lung [24]. However, elderly patients are often complicated with the presence of emphysema and lung hyperinflation, which makes it difficult to obtain the intermidsection boundary with this method [25, 26]. In the study, 11 (17.5%) patients in the elderly group suffered from emphysema, with a high incidence. For such patients, the near-infrared fluorescence guided thoracoscopic ICG reverse staining method was used to quickly and accurately confirm the intersegmental boundary. Moreover, this method can save time for the lung inflation and deflation, making the surgery process faster [27, 28]. In this research center, the surgery time of the elderly group (144.57 ±21.14) was slightly lower compared to that of the non-elderly group (153.34 ±18.65); however, the difference was not statistically significant. This may be because although the near-infrared fluorescence guided thoracoscopic IGG reverse staining method was used for 11 patients with emphysema in the elderly group to determine the intersegmental boundary, the simple inflation-deflation method was used to determine the intermidsection boundary for the other 52 cases. After the intersegmental boundary is confirmed and marked, it is not easy to transect the lung segments precisely without affecting the inflation of the remaining lung tissue. On the basis of the experience, during the surgery, an ultrasonic knife is used to separate the originally 3D intersegmental structure into a plane along the intersegmental boundary. The high-frequency vibration energy of the ultrasonic knife can enable precise transecting and effective hemostasis synchronously, without eschar, thus ensuring the accuracy of the surgical field and deep surgery. Finally, the remaining plane is accurately processed by the linear transecting and suture device. This can not only ensure the precise resection of the target lung segment, but also make the wound clean, the remaining lung stretched and well inflated, and minimize the loss of lung function.
Early NSCLC patients with GGN often have no symptoms, and a large number are accidentally discovered during physical examination [29]. In addition, due to the large number of underlying diseases, it is difficult to distinguish the early lung cancer of elderly patients from their own chronic respiratory diseases, thus delaying the opportunity of treatment [30]. Some elderly patients recover slowly after surgery, and are prone to psychological characteristics such as anxiety and self-abandonment, which often become a major difficulty in treatment [31]. Moreover, with the increase of age, the internal organ function and immunity of elderly patients become poor, with complications of chronic diseases such as hypertension and diabetes before surgery [32, 33]. Surgical methods with longer postoperative recovery time and greater trauma will undoubtedly have a greater impact on patients’ physiology and psychology [34, 35], while the application of uniportal video-assisted thoracoscopic segmental resection of the lung has advantages that do not exist in traditional thoracotomy: 1) Small surgical trauma, avoids damage to the ribs and muscles, reduces intraoperative blood loss and shortens postoperative recovery time, thereby avoiding a series of complications such as severe postoperative pain and poor wound healing due to large surgical wounds in elderly patients [36]; 2) Uniportal VATS has a clearer local exposure and a good visual angle, which is similar to the surgical field under the direct vision of thoracotomy. It can ensure the accuracy of the surgery, accurately identify the location of lesions and lymph lesions, and under the guidance of 3D images, can completely utilize the advantages of fine anatomy, maximize the remaining lung function of elderly patients, and improve the postoperative quality of life [37]; 3) The more esthetic wound makes the patient more satisfied with the prognosis, avoids the psychological and life disorders due to postoperative scar, is more conducive to the long-term recovery of the patients, and reduces the long-term impact of the surgery on the patient’s mind and movement [38].
Conclusions
Uniportal video-assisted thoracoscopic segmental resection of the lung is feasible and safe in elderly patients with NSCLC aged over 65 years. Compared with non-elderly patients, the use of appropriate technology does not increase the difficulty and time of the surgery, or increase the postoperative complications, and is worthy of clinical promotion.