








Introduction
Laparoscopic adrenalectomy (LA) was first reported by Gagner in 1992 [1]. With the development of instruments and skills, LA has improved to give better cosmetic results, less blood loss, and shorter length of hospital stay [2, 3]. Therefore, LA has been the gold standard surgical treatment for benign adrenal lesions [4, 5]. The right adrenal gland is partially retrocaval and drains directly to the inferior vena cava through a short central vein [6, 7]. Due to the anatomical features, right laparoscopic adrenalectomy (RLA) could be more challenging than left laparoscopic adrenalectomy (LLA) [6, 8]. However, other studies found the opposite results [7, 9].
Therefore, the perioperative and postoperative outcomes of RLA versus LLA are still controversial. Indeed, it is necessary to analyse the current evidence and draw objective conclusions. The purpose of this study is to perform a meta-analysis to evaluate the challenging factors of RLA versus LLA.
Aim
The aim of this study is to compare RLA with LLA and determine whether there are significant differences in terms of operative time, estimated blood loss (EBL), conversion, complications, and length of hospital stay.
Material and methods
Search strategy
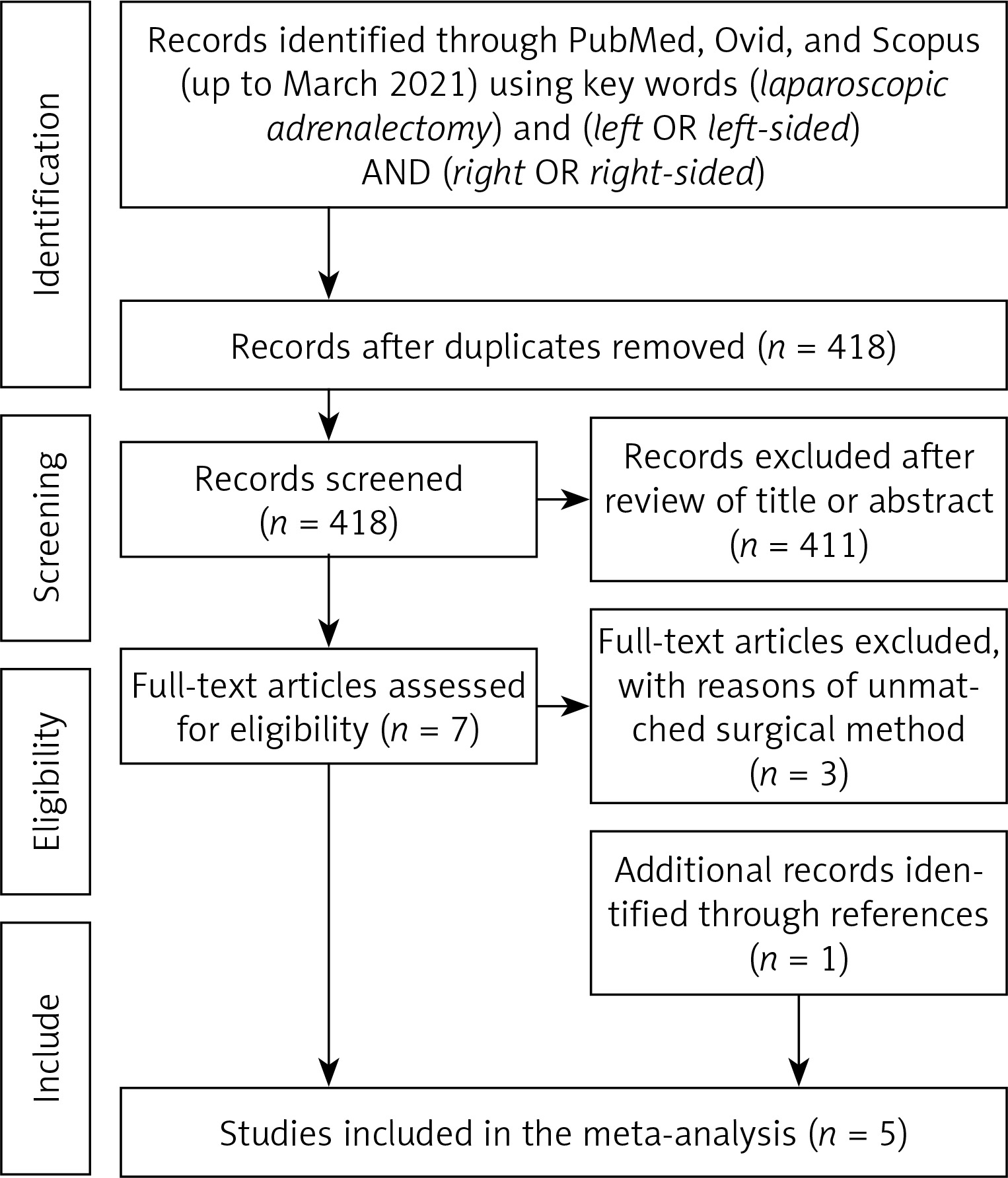
We conducted a comprehensive electronic literature search on the PubMed, Ovid, Scopus databases (up to March 2021) and reference lists to identify eligible studies comparing RLA and LLA for adrenal lesions. The search strategy was “(laparoscopic adrenalectomy) and (left OR left-sided) AND (right OR right-sided)”. The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) criteria were used for article selection (Figure 1). Two investigators (YW and ZY) independently screened all citations and abstracts to identify potentially eligible studies. Relevant references were also checked for additional eligible articles.
Inclusion and exclusion criteria
Inclusion criteria: (1) original studies comparing RLA to LLA; (2) written in English laguage for adult patients. Exclusion criteria: (1) children’s studies; (2) non-English laguage articles; (3) studies without primary or sufficient data (i.e. reviews, commentaries, conference abstracts).
Data extraction
Two investigators (XC and ZT) independently extracted data using a predefined data extraction form, including demographic characteristics (age, gender, body mass index (BMI), tumour size), peri-operative outcomes (operative time, EBL, and conversion), and post-operative outcomes (complications, Clavien-Dindo score ≥ 3 complications, and length of hospital stay). Any discrepancy was resolved in consultation with YW.
Quality assessment
Two investigators (JL and YZ) independently evaluated the evidence level of included studies according to the Oxford Centre for Evidence-based Medicine (Table I).
Table I
Basic characteristics of included studies in this meta-analysis
| Study | Period | Approach | Region | Right/Left (n) | LE |
|---|---|---|---|---|---|
| Gunseren 2019 [6] | 2006–2017 | Transperitoneal | Turkey | 135/137 | 4 |
| Cianci 2016 [7] | 2010–2015 | Transperitoneal | Italy | 21/21 | 4 |
| Chiang 2013-R [8] | 2000–2011 | Retroperitoneal | China | 31/51 | 4 |
| Chiang 2013 [8] | 2000–2011 | Transperitoneal | China | 24/21 | 4 |
| Rieder 2010 [9] | 1998–2007 | Transperitoneal | USA | 54/109 | 4 |
| Kokorak 2016 [11] | 2006–2016 | Transperitoneal | Slovak | 96/80 | 4 |
Statistical analysis
A meta-analysis was conducted using Cochrane Collaboration’s Review Manager (RevMan) 5.4 software (Cochrane Collaboration, Oxford, UK). For continuous variables, the weighted mean difference (WMD) was used with 95% confidence intervals (CI). For dichotomous variables, the odds ratio (OR) was calculated with 95% CI. For studies that only reported medians and ranges, a validated mathematical model reported by Hozo et al. was used to convert the median (range) to the mean (standard deviation) [10]. Statistical heterogeneity was defined based on the Cochrane Q p-value and I2 statistic. If p > 0.1 or I2 < 50%, a fixed-effects model was used. While, if p < 0.1 or I2 > 50%, a random-effects model was used. A p-value < 0.05 was considered statistically significant. Funnel plots were examined to evaluate publication bias.
Results
Overall, 5 studies including 780 patients (RLA 361; LLA 419) were included in this analysis (Figure 1) [6–11]. Table I shows the basic characteristics and quality assessment of the included studies.
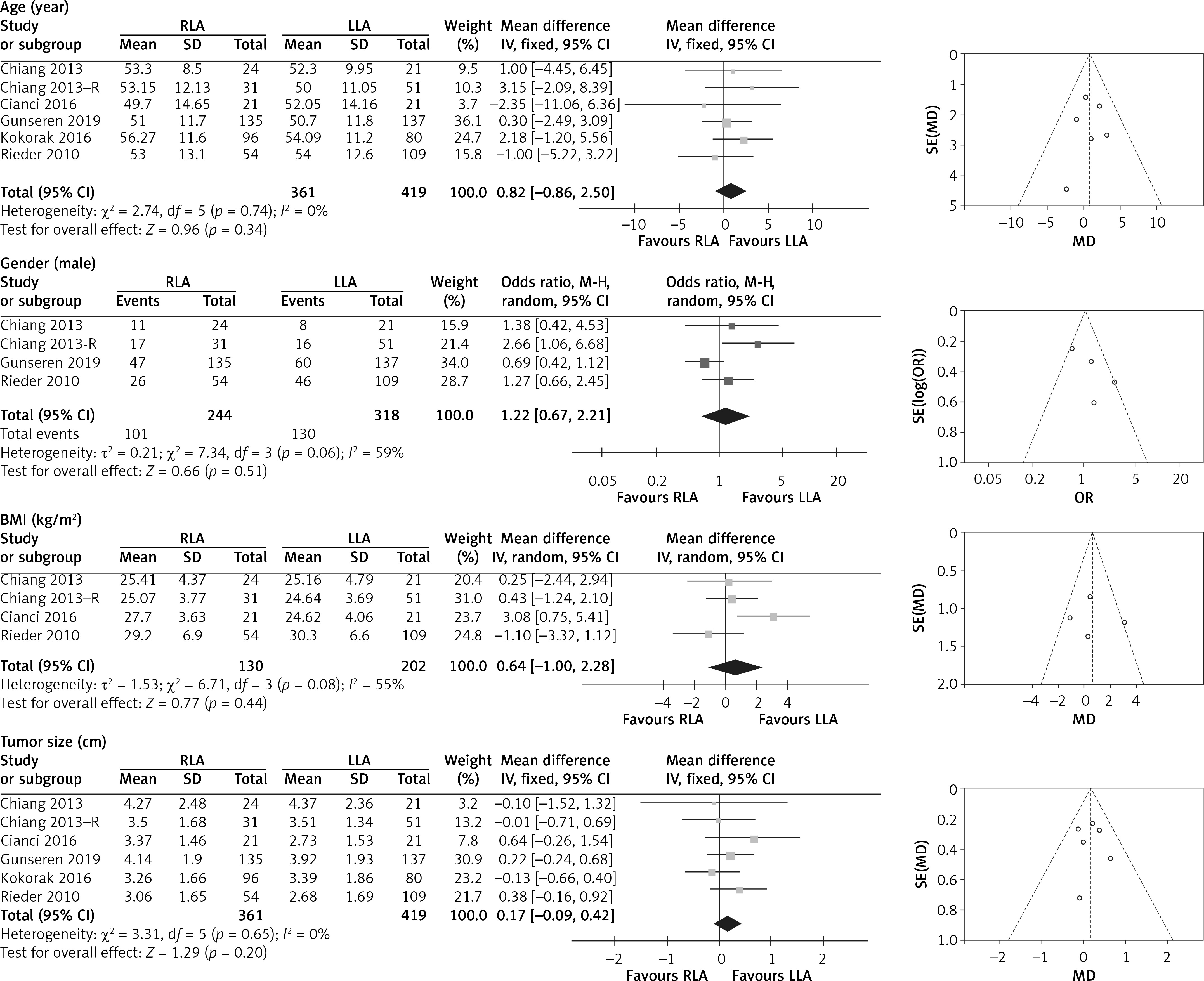
There was no significant difference in age (WMD 0.82 years, 95% CI: –0.86 to 2.50; p = 0.34), proportion of male patients (OR = 1.22, 95% CI: 0.67 to 2.21; p = 0.51), BMI (WMD 0.64 kg/m2, 95% CI: –1.00 to 2.28; p = 0.44), and tumour size (WMD 0.17 cm, 95% CI: –0.09 to 0.42; p = 0.20) (Figure 2).
Figure 2
Forest and funnel plots of demographic patient characteristics of right laparoscopic adrenalectomy (RLA) vs. left laparoscopic adrenalectomy (LLA)
Chiang 2013–R – retroperitoneal approach data from Chiang 2013, BMI – body mass index, SD – standard deviation, CI – confidence interval.
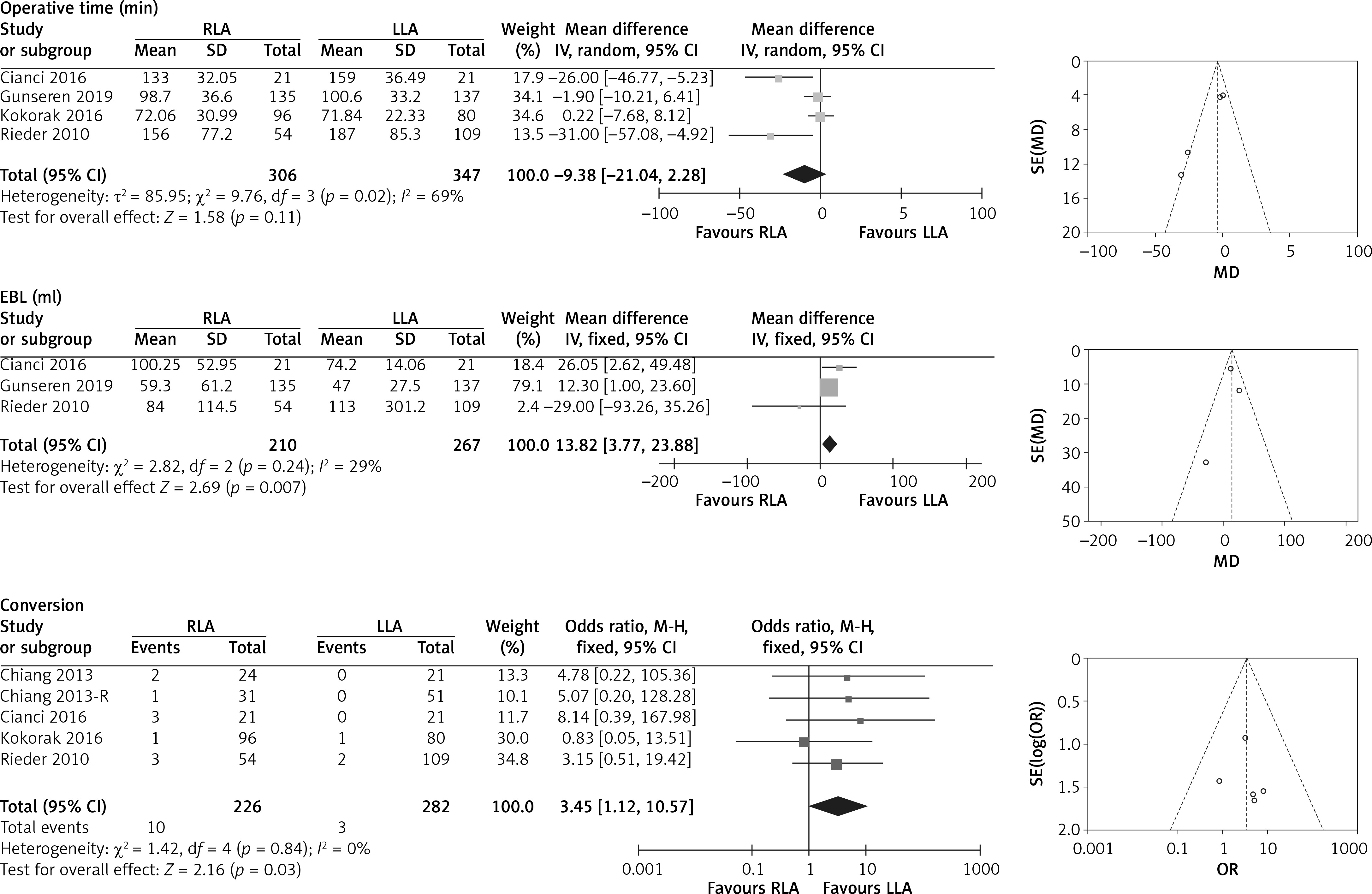
Four studies including 653 patients (RLA 306; LLA 347) reported operative time [6, 7, 9, 11]. There was no significant difference in operative time (WMD –9.38 min, 95% CI: –21.04 to 2.28; p = 0.11). Three studies including 477 patients (RLA 210; LLA 267) reported EBL [6, 7, 9]. Meta-analysis of these studies showed more EBL for RLA (WMD 13.82 ml, 95% CI: 3.77, 23.88; p = 0.007). Four studies including 508 patients (RLA 226; LLA 282) reported the conversion rate [7–11]. RLA was associated with higher conversion rate compared with LLA (OR = 3.45, 95% CI: 1.12 to 10.57; p = 0.03) (Figure 3).
Figure 3
Forest and funnel plots of peri-operative outcomes of right laparoscopic adrenalectomy (RLA) vs. left laparoscopic adrenalectomy (LLA)
EBL – estimated blood loss, Chiang 2013–R – retroperitoneal approach data from Chiang 2013, SD – standard deviation, CI – confidence interval.
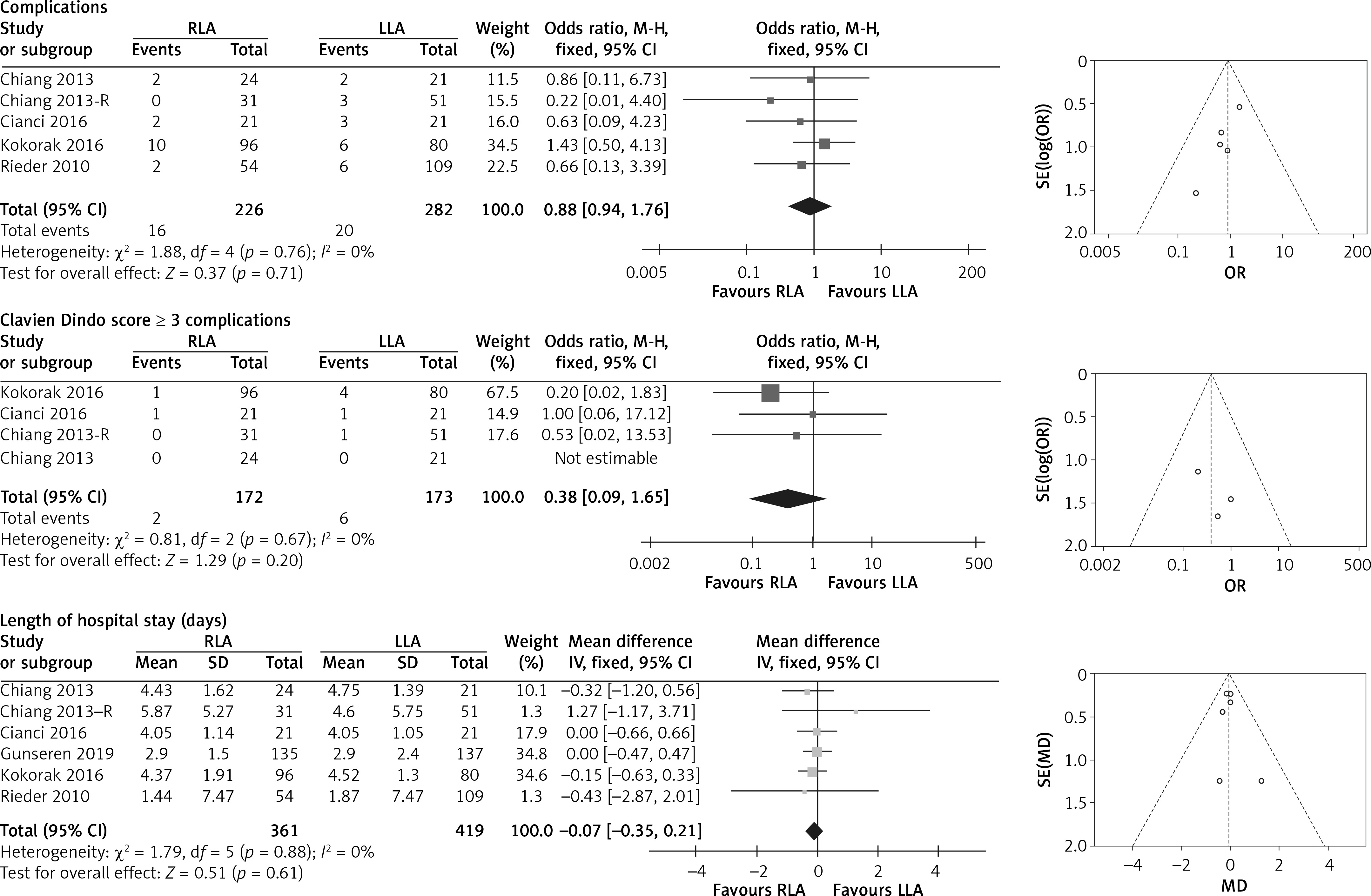
Four studies including 508 patients (RLA 226; LLA 282) reported complications [7–9, 11]. Three studies including 345 patients (RLA 172; LLA 173) reported Clavien-Dindo score ≥ 3 complications [7, 8, 11]. Five studies including 780 patients (RLA 361; LLA 419) reported the length of hospital stay [6–9, 11]. Meta-analysis of these studies showed that RLA had similar rate of complications (OR = 0.88, 95% CI: 0.44 to 1.76; p = 0.71), rate of Clavien-Dindo score ≥ 3 complications (OR = 0.38, 95% CI: 0.09 to 1.65; p = 0.20), and length of hospital stay (WMD –0.07 days, 95% CI: –0.35 to 0.21; p = 0.61) (Figure 4).
Figure 4
Forest and funnel plots of post-operative outcomes of right laparoscopic adrenalectomy (RLA) vs. left laparoscopic adrenalectomy (LLA)
Chiang 2013–R – retroperitoneal approach data from Chiang 2013, SD – standard deviation, CI – confidence interval.
Most of the studies compared RLA versus LLA via transperitoneal approach, and only 1 study reported retroperitoneal results. This could lead to bias. Therefore, we analysed the transperitoneal approach data to reduce heterogeneity.
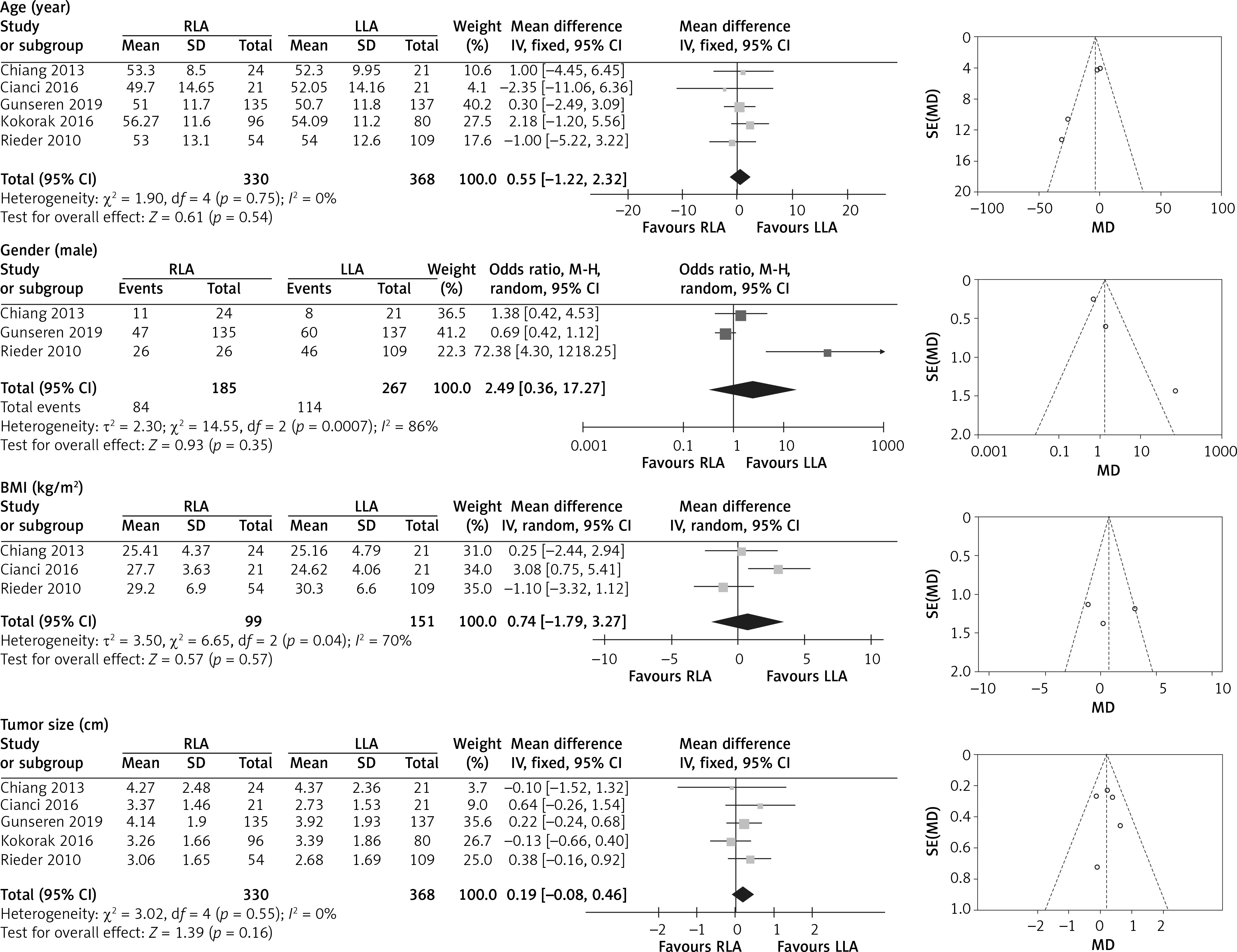
There was no significant difference in age (WMD 0.55 years, 95% CI: –1.22 to 2.32; p = 0.54), proportion of male patients (OR = 2.49, 95% CI: 0.36 to 17.27; p = 0.35), BMI (WMD 0.74 kg/m2, 95% CI: –1.79 to 3.27; p = 0.57), and tumour size (WMD 0.19 cm, 95% CI: –0.08 to 0.46; p = 0.16) (Figure 5).
Figure 5
Forest and funnel plots of demographic patient characteristics of right laparoscopic adrenalectomy (RLA) vs. left laparoscopic adrenalectomy (LLA) for transperitoneal approach
BMI – body mass index, SD – standard deviation, CI – confidence interval.
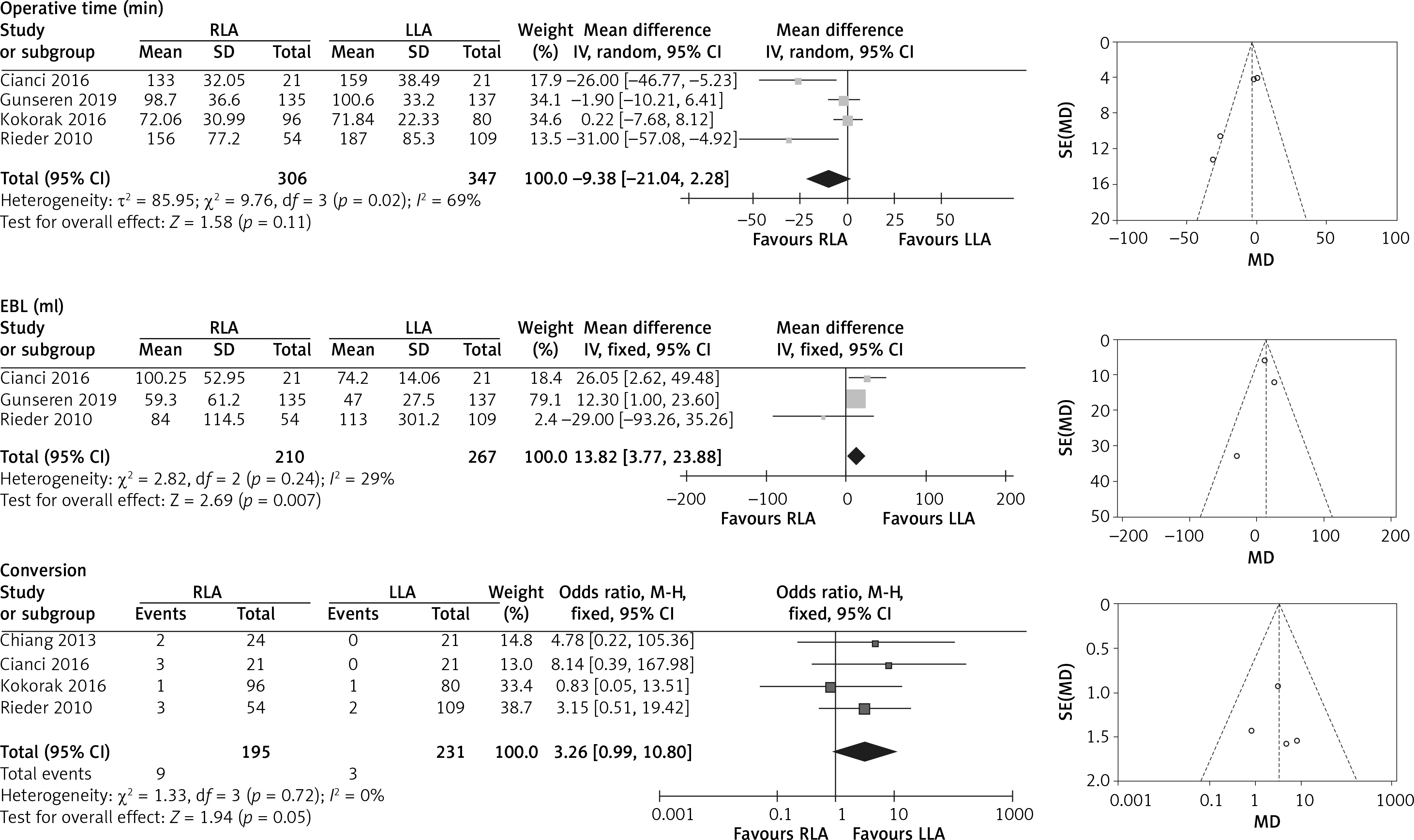
Four studies including 653 patients (RLA 306; LLA 347) reported operative time [6, 7, 9, 11]. There was no significant difference in operative time (WMD –9.38 min, 95% CI: –21.04 to 2.28; p = 0.11). Three studies including 477 patients (RLA 210; LLA 267) reported EBL [6, 7, 9]. Meta-analysis of these studies showed more EBL for RLA (WMD 13.82 ml, 95% CI: 3.77, 23.88; p = 0.007). Four studies including 426 patients (RLA 195; LLA 231) reported the conversion rate [7–9, 11]. RLA was associated with higher conversion rate compared with LLA (OR = 3.26, 95% CI: 0.99 to 10.80; p = 0.05) (Figure 6).
Figure 6
Forest and funnel plots of peri-operative outcomes of right laparoscopic adrenalectomy (RLA) vs. left laparoscopic adrenalectomy (LLA) for transperitoneal approach
EBL – estimated blood loss, SD – standard deviation, CI – confidence interval.
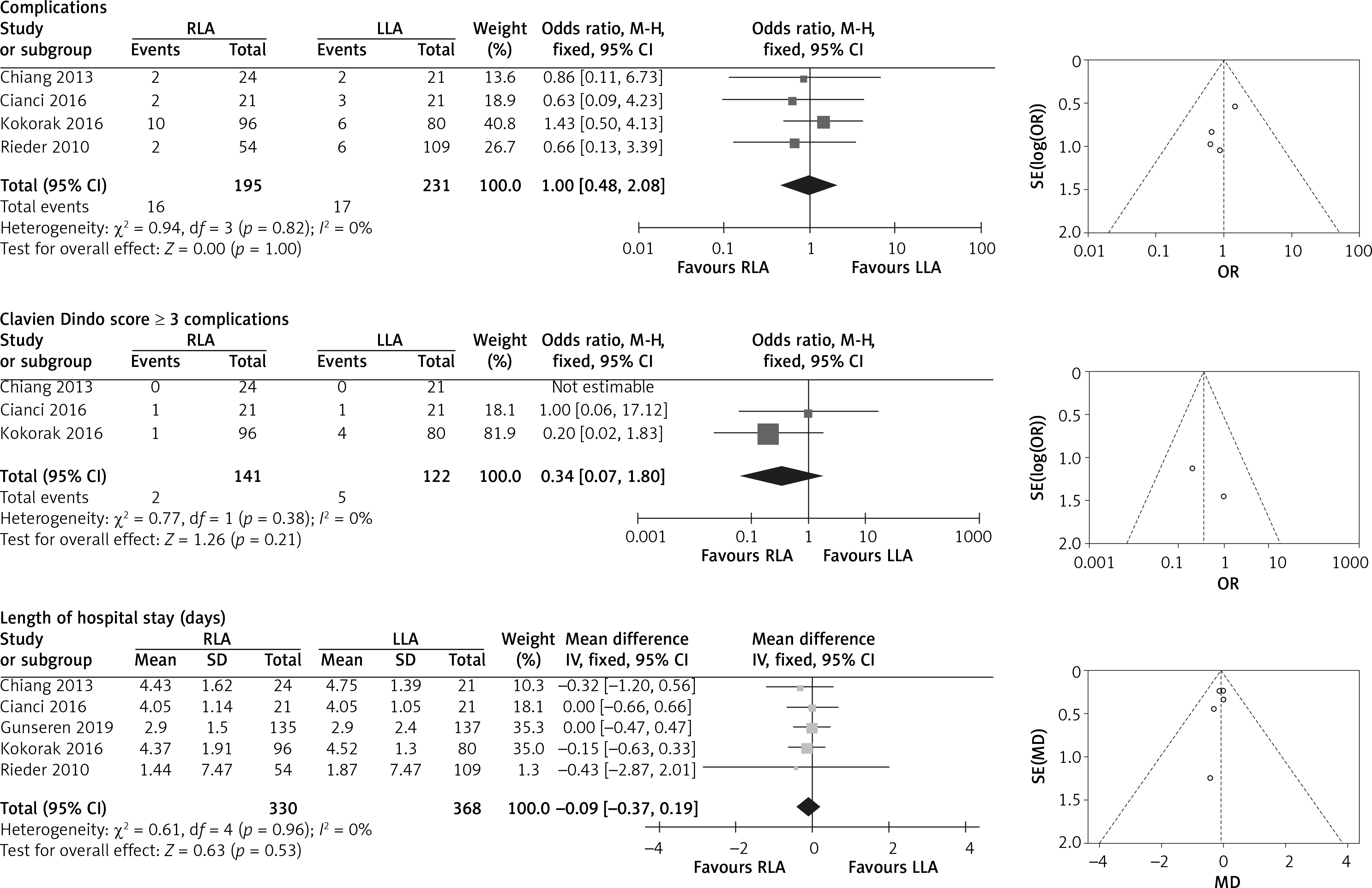
Four studies including 426 patients (RLA 195; LLA 231) reported the complications [7–9, 11]. Three studies including 263 patients (RLA 141; LLA 122) reported Clavien-Dindo score ≥ 3 complications [7, 8, 11]. Five studies including 698 patients (RLA 330; LLA 368) reported the length of hospital stay [6–9, 11]. Meta-analysis of these studies showed similar rates of complications (OR = 1.00, 95% CI: 0.48 to 2.08; p = 1.00), rate of Clavien-Dindo score ≥ 3 complications (OR = 0.34, 95% CI: 0.07 to 1.80; p = 0.21), and length of hospital stay (WMD –0.09 days, 95% CI: –0.37 to 0.19; p = 0.53) (Figure 7).
Figure 7
Forest and funnel plots of post-operative outcomes of right laparoscopic adrenalectomy (RLA) vs. left laparoscopic adrenalectomy (LLA) for transperitoneal approach
SD – standard deviation, CI – confidence interval.
There was no significant publication bias in this study.
Discussion
In the past decade, LA has been the gold standard method for the treatment of benign adrenal lesions. Recently, Sahbaz et al. reported that LA can be safely performed on large adrenal masses without obvious perioperative and postoperative complications [12]. Because the right adrenal gland is partially retrocaval and drains directly to the inferior vena cava through a short central vein, there is an opinion that RLA is more challenging than LLA [6, 8, 13]. While, Kokorak et al. reported similar results between RLA and LLA [11]. However, some studies reported that LLA was more challenging than RLA [7, 9, 14]. Therefore, it is necessary to conduct a meta-analysis to evaluate the efficacy and safety of RLA and LLA.
In our meta-analysis, patients treated with RLA and LLA were similar in age, gender, BMI, and tumour size. After omitting the only retroperitoneal approach data, the results were consistent. These reflected the homogeneity of the included studies.
The meta-analysis of our study showed comparable operative time. RLA showed more EBL and higher conversion rate. The transperitoneal approach data showed the same results. Due to the anatomical characteristics of the right adrenal gland, RLA should be riskier. Our results also supported this theory. However, some studies have emphasized that LLA via transperitoneal approach was more complex for a variety of reasons. First, it is difficult to dissect the tail of the pancreas for better exposure of the left adrenal gland. Varkarakis et al. reported an 8% rate of pancreatic injury during LLA [15]. Second, mobilization of the splenic flexure of the colon is required for a better exposure of the left adrenal gland. Anatomical variations of the spleen are very common, which make the dissection more complicated. However, the retraction of the liver is more simple on the right side [7]. Third, the dissection of the left renal hilum for vascular control of the adrenal vein is more complicated. All these reasons indicate that the procedure on the left is more complex than the procedure on the right. Nonetheless, the left adrenal gland anatomy is more complex. An experienced surgeon can quickly complete renal hilus dissection and mobilization of the spleen and splenic colonic flexure without any problems [6]. This can also be concluded from the similarity of operative time. However, even for experienced surgeons, there was a greater possibility of bleeding from the right side. Although the RLA group had more EBL, the mean EBL was approximate 100 ml, hardly requiring any transfusion. This reflects the safety of RLA and LLA. Indeed, there were some episodes of significant bleeding possibly requiring transfusion. In this meta-analysis, Rieder et al. reported significant bleeding for LLA. Nevertheless, RLA still had more EBL than LLA. This reflects the higher overall bleeding risk of RLA [9]. In addition, the open conversion was more common on the right side [6, 13, 16, 17]. These results revealed that RLA could be riskier than LLA.
Our meta-analysis showed similar complications, Clavien Dindo score ≥ 3 complications, and length of hospital stay. In the overall perspective, there was no significant difference in postoperative results between RLA and LLA. These results reflected the safety of the 2 procedures.
There are several limitations to this study. First, the retrospective nature of the included studies limited the quality of the results. Second, the surgical approach was not standardized. Third, the small sample size limited the reliability of the results. Fourth, the pathological data were not available for analysis. Fifth, the follow-up time was unclear. Multicentre randomized controlled trials are needed to further conform the results.