
INTRODUCTION
Vitamin D is a fat-soluble secosteroid involved in mineral homeostasis and bone metabolism [1, 2]. Vitamin D deficiency remains common in both developed and developing countries, with a global prevalence estimated to affect up to 1 billion people [1]. Beyond its classical role in calcium and phosphate metabolism, vitamin D participates in numerous enzymatic, metabolic, physiological, and pathophysiological processes across multiple organs and systems, including modulation of innate and adaptive immune responses [2–4].
Human papillomavirus (HPV) infection occurs in approximately 7–12% of the general population [5]. Clinical manifestations depend on the viral genotype and the site of infection. More than 200 types of HPV have been identified, with approximately 40 types infecting the oral and anogenital mucosa [5–7]. Many HPV-associated lesions show poor response to treatment and frequent recurrence, which has led to increasing interest in improving therapeutic strategies.
Various immunotherapeutic approaches have been investigated in recent years, including intradermal administration of purified protein derivative (PPD) from Mycobacterium tuberculosis, measles-mumps-rubella (MMR) vaccine, Bacillus Calmette-Guérin (BCG) vaccine, Candida antigen and extract, and vitamin D [8].
Recent studies evaluating intralesional and topical vitamin D for the treatment of cutaneous and anogenital warts suggest that it may represent a promising therapeutic option. In addition, several investigations have explored the relationship between vitamin D status and susceptibility to HPV infection. Therefore, this review aims to provide a comprehensive overview of the role of vitamin D in cutaneous and anogenital HPV-associated infection.
VITAMIN D
Sources and metabolism
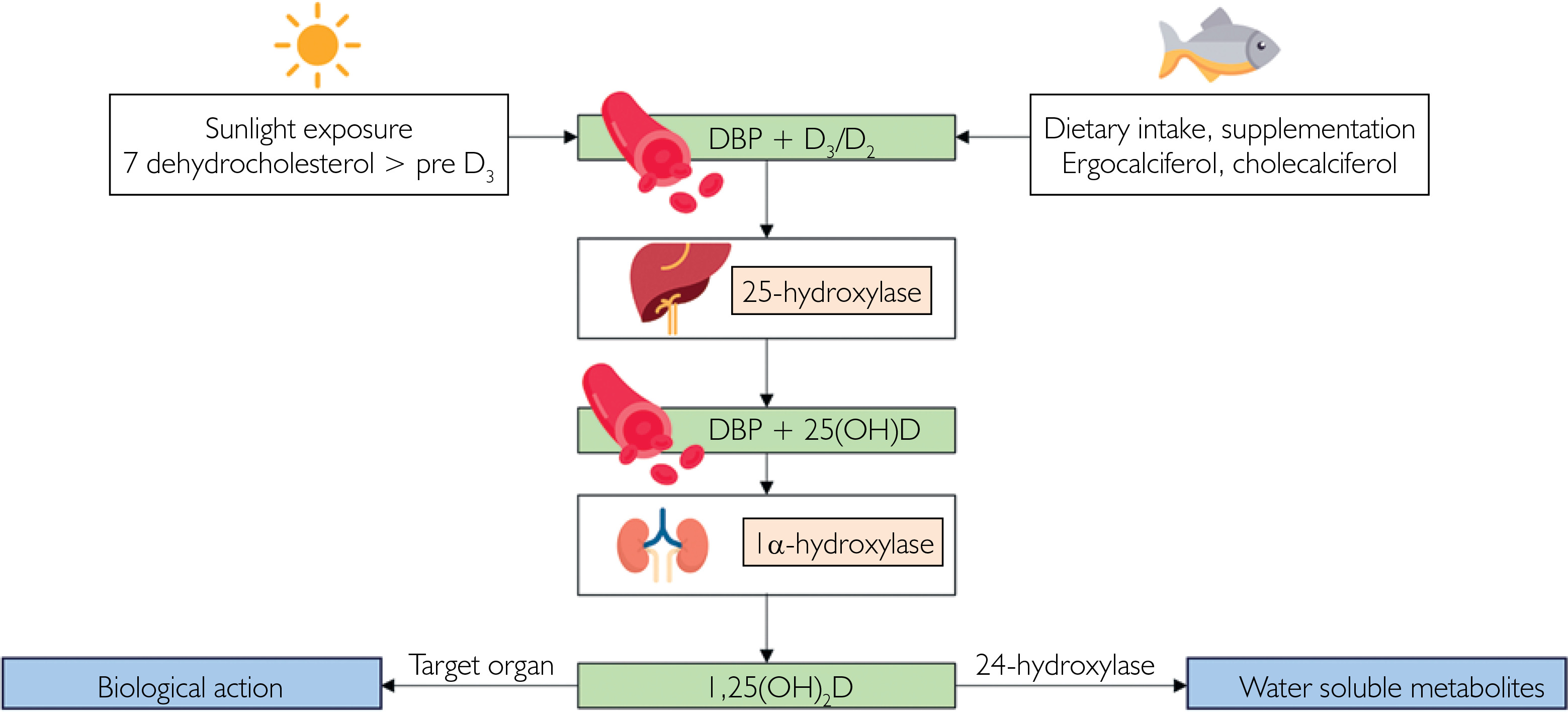
The majority of vitamin D is synthesized in the skin through exposure to ultraviolet (UV) B radiation, which converts 7-dehydrocholesterol into unstable previtamin D3 that is subsequently transformed into vitamin D3 [2, 9]. Excessive UV exposure leads to the formation of inactive metabolites, serving as a protective mechanism against vitamin D3 toxicity [9–11]. Cutaneous production depends on several factors, including age, skin pigmentation, season, weather conditions, latitude, altitude, duration of sun exposure, clothing, the extent of exposed skin, and sunscreen use [2, 9, 12–14].
A smaller portion of vitamin D is obtained from dietary sources. Vitamin D2 is mainly present in plant-based products, whereas vitamin D3 is derived from animal sources [2, 9, 11, 15]. Additional intake may come from fortified foods and supplements.
Vitamin D metabolism is illustrated in figure 1. In the bloodstream, vitamin D binds to vitamin D binding protein (DBP) and is transported to the liver. Both vitamin D2 and D3 undergo hydroxylation by 25-hydroxylase to form 25-hydroxyvitamin D (25(OH)D), the main marker of vitamin D status influenced by sun exposure and dietary intake [2, 3, 9, 11, 15]. Subsequently, 25(OH)D is transported to the kidneys, where 1α-hydroxylase converts it into the biologically active form, 1,25-dihydroxyvitamin D (1,25(OH)2D). This metabolite promotes its own degradation through activation of 24-hydroxylase, leading to the formation of inactive, water-soluble products [2, 3, 9, 11, 15]. As the active hormonal form, 1,25(OH)2D mediates the biological effects of vitamin D.
Biological actions
The activity of 1,25(OH)2D is mediated by the vitamin D receptor (VDR). After binding to its ligand, VDR forms a heterodimer with the retinoid X receptor (RXR) and interacts with vitamin D response elements (VDRE) in the nucleus, thereby regulating gene transcription [15].
Parathyroid hormone (PTH) increases calcium release from bone, enhances renal reabsorption of calcium, and stimulates calcitriol synthesis. Activated VDR promotes intestinal absorption of calcium and phosphate. Together with PTH, it also induces osteoclast maturation via RANK ligand expression on osteoblasts, leading to bone resorption [1, 2].
VDR is widely expressed in multiple tissues, allowing vitamin D to exert effects beyond calcium and bone metabolism [2–4, 9, 12, 16]. In the skin, 1,25(OH)2D regulates keratinocyte differentiation, supports hair cycle phases, exhibits antitumor activity, reduces oxidative stress and inflammation, promotes skin barrier repair, and increases LL-37 expression, which contributes to inflammation control and angiogenesis [9, 10, 13, 16].
Role of vitamin D in immunity
Vitamin D influences both innate and adaptive immune responses. This role is supported by the presence of VDR in immune cells such as monocytes, macrophages, and dendritic cells, as well as by the expression of CYP27B1 enzyme responsible for local conversion of 25(OH)D into its active form [2–4, 12].
In innate immunity, 1,25(OH)2D induces transcription of genes encoding CD14, which participates in the activation of antimicrobial peptides including LL-37, α-defensin, and β-defensin-2 (fig. 2 A) [3, 9, 12, 13, 16–18]. These peptides inhibit viral replication, disrupt viral membranes, and prevent viral entry into host cells. Vitamin D also increases VDR and CYP27B1 expression in macrophages through activation of toll-like receptor (TLR) 2, and enhances TLR2 and TLR4 expression in keratinocytes [3, 4, 12]. In addition, 1,25(OH)2D promotes autophagy in macrophages [4]. TLR2 and TLR4 are responsible for recognition of pathogen-associated molecular patterns [3, 17].
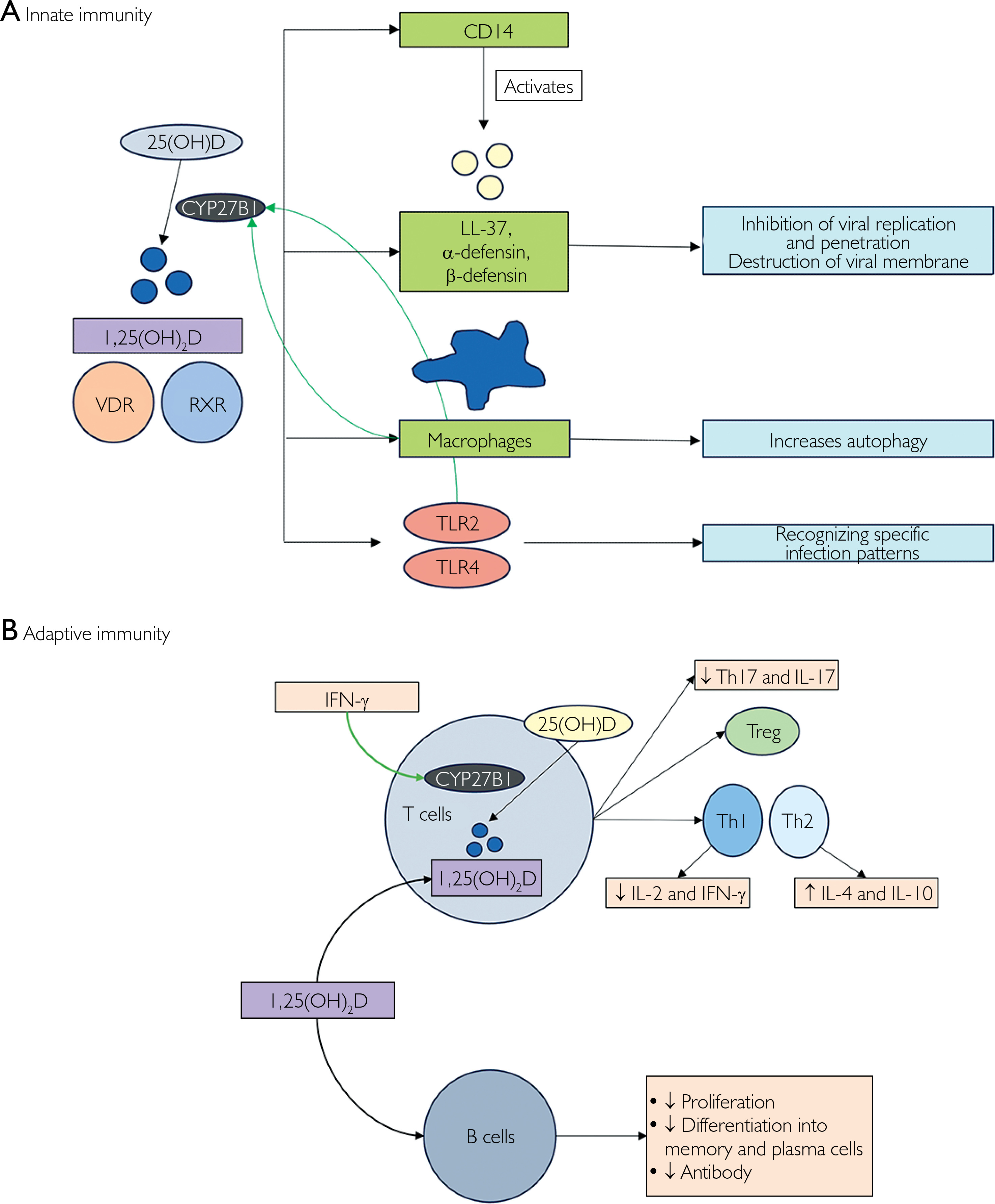
Within adaptive immunity (fig. 2 B), 1,25(OH)2D shifts the immune response toward a humoral profile by suppressing Th1 cytokines (IL-2, IFN-γ) and increasing Th2 cytokines (IL-4, IL-10). It promotes differentiation of regulatory T cells, inhibits Th17 development and IL-17 production, and modulates IFN-γ-induced CYP27B1 expression [3, 9, 17]. In B lymphocytes, 1,25(OH)2D limits excessive immune activation by reducing proliferation, differentiation, and antibody production [3, 9].
HPV INFECTION
Epidemiology
HPV infection occurs worldwide and affects individuals of all age groups. Cutaneous warts are most common in children and young adults, with an estimated prevalence of 30–70% among school-aged children [5]. Genital HPV infection, typically transmitted through sexual contact, is more prevalent in young adults, with an estimated prevalence of 10–20%, although only about 1% of infected individuals develop clinical symptoms [19]. Malignancy usually results from persistent infection with high-risk HPV over several years.
Virology and pathomechanism
HPV belongs to the Papillomaviridae family and is a circular double-stranded DNA virus, approximately 8,000 base pairs in length, enclosed within a 60 nm icosahedral capsid [5, 20–23]. The viral genome consists of three major regions: early, late, and the long control regions (LCR) [6, 21, 24]. The early region encodes open reading frames (ORF) involved in viral replication, whereas the late region encodes structural capsid proteins [5, 21]. The LCR contains regulatory elements controlling viral gene expression and DNA replication [21, 24].
HPV infects squamous epithelium through microabrasions on the skin or mucosa. The virus enters basal keratinocytes with the assistance of the L1 and L2 late region proteins, and viral DNA is transported to the nucleus during mitosis [5, 20, 21, 23, 24]. During latent phase, the viral genome persists as an episome without causing clinical symptoms [5, 21, 25]. In the early stage of replication, E1 and E2 proteins facilitate viral DNA replication. Virion assembly occurs in differentiated keratinocytes, supported by the E4 protein, and newly formed virions are released as these cells mature and are shed [5, 21].
HPV relies entirely on host cell enzymes for replication and stimulates keratinocyte proliferation, leading o lesion formation. Although the immune system – particularly T cells and cytokines – plays a crucial role in viral clearance, HPV avoids immune detection by restricting viral gene expression and virion release to the upper epithelial layers, where immune surveillance is limited [6, 26].
Most infections resolve spontaneously within 1 to 2 years. However, persistent infection may lead to integration of viral DNA into the host genome [23]. This process increases expression of the E6 and E7 oncoproteins, which inactivate the tumor suppressor proteins p53 and pRb [6, 21–23]. As a consequence, cellular proliferation becomes dysregulated, promoting carcinogenesis and neoplastic transformation of epithelial tissue.
HPV-associated diseases
HPV-associated lesions are diverse and include cutaneous warts, anogenital warts, epidermodysplasia verruciformis, recurrent respiratory papillomatosis, as well as precancerous and malignant lesions [5, 7]. Over 200 HPV types have been identified and classified into five main genera based on anatomical and pathological tropism [5, 6, 20, 22, 23]. These types are further categorized as high-risk or low-risk according to their oncogenic potential. Table 1 summarizes HPV types and their associated diseases.
Table 1
Cutaneous warts are the most common HPV-associated skin lesions and typically occur on the hands, feet, and other areas of the body [5, 27]. They include several clinical variants, such as common warts (HPV27, HPV57, HPV2), flat warts (HPV3, HPV10), plantar warts, and filiform warts.
Anogenital warts are caused primarily by low-risk HPV types, most frequently HPV6 and HPV11, and are transmitted through sexual contact [5, 20, 28]. These types may also affect the oral cavity, producing oral warts [24]. Morphologically, anogenital warts are classified into four types: condyloma acuminata, papular, hyperkeratotic, and flat-topped lesions. A rare but more aggressive form, giant condyloma of Buschke-Löwenstein, represents a locally destructive precancerous lesion [20, 28].
Several other HPV-associated conditions may occur in childhood. Epidermodysplasia verruciformis is a rare autosomal recessive genodermatosis caused by mutations in the EVER1/TMC6 and EVER2/TMC8 genes. This disorder may progress to cutaneous squamous cell carcinoma (SCC), particularly in cases associated with HPV5 and HPV8 infection [29].
Recurrent respiratory papillomatosis is a benign neoplasm in the respiratory tract caused by HPV6 and HPV11, mainly transmitted during child-birth [30].
Persistent infection with high-risk HPV is associated with malignant transformation. Anogenital intraepithelial neoplasia encompasses dysplasia across various anogenital sites, including the vulva, vagina, cervix, penis, perianal skin, and anus [5, 28]. These lesions represent precursors of SCC driven mainly by HPV16 and HPV18 [5, 28].
In immunocompetent individuals, warts rarely progress to malignancy. Although high-risk HPV infections are usually cleared by the host immune system, persistent infection may occasionally lead to intraepithelial or invasive neoplasia, including Bowen’s disease, Bowenoid papulosis, erythroplasia of Queyrat, and SCC [31].
Prevention
Vaccination is an effective strategy for the prevention of anogenital HPV infection [21, 22]. Because certain HPV types are transmitted through sexual contact, patient education remains essential, particularly regarding consistent condom use and limiting the number of sexual partners [5, 19]. Screening programs also play a key role in early detection of HPV infection and prevention of HPV-associated diseases and cancers [19].
Management
The management of cutaneous lesions associated with HPV infection depends on several factors, including lesion type, anatomical location, severity, and previous treatment response [5, 7]. The main therapeutic goals are lesion eradication, symptom relief, and prevention of recurrence [7]. Numerous treatment modalities are available for HPV-related lesions (table 2) [5, 7, 25].
Table 2
Treatment outcomes vary among patients, largely due to differences in host immune responses. In recent years, novel therapeutic strategies – particularly immunomodulatory approaches – have been developed and evaluated in clinical studies. Immunotherapy aims to stimulate the host immune system to enhance antiviral activity and promote clearance of HPV-infected cells [8]. Agents used in this approach include PPD of Mycobacterium tuberculosis, MMR vaccine, BCG vaccine, Candida antigen and extract, and vitamin D.
ROLE OF VITAMIN D IN HPV INFECTION
Vitamin D status, supplementation, and HPV infection
Vitamin D deficiency and its supplementation have been investigated in several studies, yielding inconsistent results. Both oral and vaginal vitamin D supplementation have been evaluated and, in some reports, were associated with improved HPV clearance and reduced cervical lesions [32–34]. Lower vitamin D levels have been observed in individuals with cutaneous warts and cervicovaginal HPV infections [35–38]. In addition, the risk of cervicovaginal HPV infection increases with each 10 ng/ml decrease in serum vitamin D levels [36]. An association between vitamin D deficiency and oral HPV infection has also been reported in women, although this relationship was not observed s at other anatomical sites or in men [39].
Systemic vitamin D supplementation may enhance host defense by improving metabolic and nutritional status, reducing insulin resistance, and lowering inflammatory and oxidative stress markers such as hs-CRP and MDA, thereby creating conditions less favorable for viral persistence [32, 34]. Local administration may additionally support epithelial differentiation and barrier integrity while modulating the local immune microenvironment to facilitate viral clearance [33]. These findings suggest that vitamin D may influence HPV-related outcomes through both systemic metabolic-immune pathways and local epithelial mechanisms.
However, several studies have reported no significant association between vitamin D status and cervicovaginal HPV infection or cutaneous warts [40–42]. One study found no correlation between vitamin D levels and the incidence, number, or recurrence of anogenital warts [43]. Similarly, vitamin D supplementation for six months did not significantly improve cervical HPV clearance [44]. In pediatric populations, Cao et al. reported that vitamin D levels in children with cutaneous warts were not significantly lower than those in children with other dermatological conditions [8]. Interestingly, Mendelian randomization analysis demonstrated a positive causal relationship between higher vitamin D levels and increased risk of wart development [8]. These findings suggest that supplementation in children, particularly those with sufficient baseline levels, should be considered with caution.
Vitamin D as a therapeutic modality for HPV infection in the skin and anogenital mucosa
Vitamin D has also been evaluated as a therapeutic option for HPV-related lesions of the skin and anogenital mucosa, both as monotherapy (table 3) and in comparison with other immunotherapeutic agents (table 4). The most commonly used approach is intralesional (IL) administration of vitamin D3 at doses ranging from 12,000 to 600,000 IU or up to 7.5 mg. Injections are typically administered every 2 to 4 weeks for a total of three to seven sessions.
Table 3
Studies using vitamin D for the therapy of HPV-associated diseases
| Author, year | Diagnosis | Intervention | n | Treatment regimen | Outcome |
|---|---|---|---|---|---|
| Aryal et al. (2024) [45] | Recalcitrant cutaneous warts | IL vitamin D3 | 92 | Every 4 weeks, up to 3 sessions | 76.08% complete response |
| Almuhyi et al. (2024) [70] | Cutaneous warts | IL vitamin D3 vs. Topical calcipotriol | 28/28 | Every 2 weeks, up to 4 sessions | 59% vs. 95% complete response |
| Merry et al. (2024) [55] | Cutaneous warts | IL vitamin D3 vs. IL placebo | 41/36 | Every 4 weeks, up to 3 sessions | 30% vs. 31% complete response |
| Ali et al. (2023) [46] | Plantar warts | IL vitamin D3 | 65 | Every 2 weeks, up to 4 sessions | 70.8% clinical improvement |
| Al-Sabak et al. (2023) [47] | Cutaneous warts | IL vitamin D3 | 40 | Every 4 weeks | 81.9% complete response |
| Noureen et al. (2023) [48] | Common warts | IL vitamin D3 | 70 | Every 2 weeks, up to 4 sessions | 28.6% complete response |
| Sharma et al. (2023) [49] | Cutaneous warts | IL vitamin D3 | 55 | Every 2 weeks, up to 4 sessions | 63.63% complete response |
| Alfetory and Duweb (2023) [53] | Cutaneous warts | IL vitamin D3 | 36 | Every 2 weeks, up to 4 sessions | 89% complete response |
| Latif et al. (2021) [50] | Common warts | IL vitamin D3 | 41 | Every 2 weeks, up to 6 sessions | 65.85% complete response |
| Jha (2021) [68] | Anogenital warts | IL vitamin D3 | 1 | Every 2 weeks, up to 3 sessions | Complete response, no recurrence at 6 months |
| Tawfik et al. (2020) [69] | Anogenital warts | IL vitamin D3 | 20 | Every 2 weeks, up to 4 sessions | 11.11% complete response |
| Sorour et al. (2020) [51] | Common warts | IL vitamin D3 | 20 | Every 2 weeks, up to 3 sessions | 40% complete response; increased LL-37 expression |
| Mohta and Jain (2020) [54] | Recalcitrant cutaneous warts | IL vitamin D3 | 1 | Every 3 weeks, 3 sessions | Complete response, no recurrence at 3 months |
| Elmas et al. (2020) [71] | Plane warts | Topical calcipotriol | 1 | Daily for 8 weeks | Complete response, no recurrence at 6 months |
| Abdel-Azim et al. (2020) [52] | Cutaneous warts | IL vitamin D3 vs. IL saline | 32 / 32 | Every 2 weeks, up to 4 sessions | 56.25% complete response |
Table 4
Studies comparing vitamin D to other immunotherapeutic agents for the therapy of HPV-associated diseases
| Author, year | Diagnosis | Intervention | n | Duration | Outcome |
|---|---|---|---|---|---|
| Shaafie et al. (2025) [56] | Cutaneous warts | IL vitamin D3 vs. IL PPD | 53/53 | Every 2 weeks, up to 4 sessions | 70.6% vs. 75.5% complete response |
| Chaudhary et al. (2023) [57] | Cutaneous warts | IL vitamin D3 vs. IL MMR vs. IL PPD vs. IL Candida antigen | 25/25/25/25 | Every 3 weeks, up to 3 sessions | 100% vs. 62% vs. 84% vs. 84% complete response |
| Fathy et al. (2023) [58] | Recalcitrant plantar warts | IL vitamin D3 vs. IL Candida antigen vs. IL saline | 20/20/20 | Every 3 weeks, up to 3 sessions | 70% vs. 25% vs. 0% complete response |
| Lahoria et al. (2023) [59] | Cutaneous warts | IL vitamin D3 vs. IL MIP vs. IL MMR vs. IL Placebo | 50/48/49/50 | Every 2 weeks, up to 7 sessions | 66% vs. 58% vs. 55% vs. 64% complete response |
| Nasr et al. (2023) [60] | Cutaneous warts | IL vitamin D3 vs. IL Candida antigen vs. ICVT | 25/25/25 | Every 2 weeks, up to 5 sessions | 48% vs. 60% vs. 28% complete response |
| Abdelaal et al. (2021) [61] | Plantar warts | IL vitamin D3 vs. IL Candida antigen | 20/20 | Every 3 weeks, up to 3 sessions | 45% vs. 40% complete response |
| Abdel Razik et al. (2021) [67] | Recalcitrant common warts | IL vitamin D3 IL Candida antigen vs. IL saline | 30/30/20 | Every 3 weeks, up to 4 sessions | 20% vs. 76.7% vs. 0% complete response |
| Abd El-Magid et al. (2021) [62] | Plantar warts | IL vitamin D3 vs. IL zinc sulfate 2% | 20/20 | Every 2 weeks, up to 4 sessions | 80% vs. 70% complete response |
| Mohta et al. (2021) [66] | Recalcitrant cutaneous warts | IL vitamin D3 vs. IL MMR vs. IL saline | 35/35/35 | Every 2 weeks, up to 4 sessions | 75.7% vs. 87.8% vs. 12.5% complete response |
| El-Sayed et al. (2020) [63] | Plantar warts | IL vitamin D3 vs. IL zinc sulfate 2% vs. IL saline | 35/35/35 | Every 2 weeks, up to 4 sessions | 62.5% vs. 71.4% vs. 40% complete response |
| Ghaly et al. (2020) [64] | Plantar warts | IL vitamin D3 vs. IL PPD vs. IL saline | 20/20/20 | Every 2 weeks, up to 3 sessions | 70% vs. 50% vs. 0% complete response |
| Nofal et al. (2020) [65] | Plantar warts | IL vitamin D3 vs. IL zinc sulfate 2% vs. IL Candida antigen vs. IL saline | 38/38/38/38 | Every 3 weeks, up to 4 sessions | 89.5% vs. 52.7% vs. 65.7% vs. 21.2% complete response |
As monotherapy for cutaneous warts, IL vitamin D3 has demonstrated variable efficacy, with complete response rates ranging from 30% to 100% [45–54]. However, one study reported limited effectiveness, with complete clearance achieved in only 30% of subjects receiving IL vitamin D3 compared to 31% in the placebo group [55]. This outcome may be related to that relatively low dose used (12,000 IU) and insufficient description of the placebo preparation.
Comparative studies evaluating IL vitamin D3 against other immunotherapeutic agents have reported variable efficacy, with complete response rates ranging from 20% to 100% [55–67]. Several studies demonstrated superior outcomes compared with Candida antigen [57, 58, 60, 61, 65]. When compared with purified protein derivative (PPD), IL vitamin D3 showed similar or slightly better efficacy [56, 64]. In some studies, results were also comparable or superior to those obtained with 2% zinc sulfate [62, 63, 65]. Placebo groups receiving normal saline consistently demonstrated significantly lower response rates, supporting the effectiveness of immunotherapeutic approach.
Evidence regarding the effectiveness of vitamin D therapy for anogenital warts remains limited. A case report by Jha in 2021 described complete resolution after three sessions of IL vitamin D3 [68]. In contrast, Tawfik et al. reported low efficacy, with only 11% of subjects achieving complete clearance [69]. These differences may reflect variation in treatment response among HPV types, particularly types 6 and 11 compared with cutaneous HPV strains.
Topical formulations have also been investigated. Calcipotriol, a synthetic analogue of 1,25(OH)2D, has demonstrated similar therapeutic potential. Almuhyi et al. reported faster and more pronounced improvement with calcipotriol compared with IL vitamin D3 in cutaneous warts [70]. An 8-week course resulted in complete resolution of verruca plana without recurrence [71]. Topical therapy has also been associated with fewer adverse effects than IL administration [70].
Vitamin D exhibit antiviral activity, particularly against DNA viruses such as HPV, likely through modulation of both innate and adaptive immune responses [4]. Through VDR-dependent pathways, it promotes epithelial differentiation and keratinocyte homeostasis while suppressing oncogenic signaling, including hypoxia, complement activation, inflammatory pathways, and TNF-α/NF-κB, with additional inhibition of IL-6–JAK–STAT3 signaling [72]. It also enhances antimicrobial defense through upregulation of CD14, reduces oxidative stress, and modulates immune cell infiltration by increasing CD8+ T cells and NK cells while reducing Tregs. Increased LL-37 expression further contributes to antiviral activity and lesion regression [4, 48, 72]. Collectively, these mechanisms support the formation of an antiviral microenvironment that may reduce viral persistence.
Differences in treatment outcomes likely reflect variation in lesion type, patient characteristics, dosing regimens, and definitions of response. Additional factors, including smoking and older age, may also influence treatment efficacy [73]. Although several studies demonstrate promising results, others suggest greater effectiveness of alternative immunotherapies. Overall, both IL and topical vitamin D3 may represent useful therapeutic options, particularly when other treatment modalities are unavailable or contraindicated.
CONCLUSIONS
Vitamin D shows potential in the management of HPV-related infections due to its immunomodulatory and antiviral properties; however, available evidence remains inconsistent. Both IL and topical formulations demonstrate variable efficacy in the treatment of cutaneous and anogenital warts. Differences in HPV type, patient characteristics, treatment regimens, age, and smoking status likely contribute to heterogeneous outcomes. Further well-designed studies with standardized protocols are required to confirm its clinical effectiveness.










