








Introduction
Since the introduction of laparoscopic surgery (LS) in 1987, surgery has shifted from conventional surgical procedures towards less invasive alternatives [1]. The LS, a minimally invasive procedure, brought about many attractive and promising advantages for patients, including decreased postoperative pain, shorter hospital stay and more rapid recovery compared with open surgical procedures. Rapid recovery following LS is particularly accomplished through a reduction of postoperative incisional site pain. However, post-laparoscopic shoulder pain (PLSP), which is often underestimated by healthcare professionals, may accompany laparoscopy procedures in a varying incidence, ranging from 35% to 80% [2]. Although the exact mechanism underlying shoulder pain has not yet been clearly elucidated, carbon dioxide accumulation and phrenic nerve irritation as a result of diaphragmatic stretching are the most accepted explanations [3, 4].
A number of techniques that are proposed to diminish shoulder pain via reducing phrenic nerve irritation have not been translated into daily practice because of being impractical or not effective enough to achieve the benefit required in routine clinical use. Among them, the pulmonary recruitment manoeuvre (PRM), which consists of five manual pulmonary inflations performed with a maximal pressure of 40–60 cm H2O, has attracted attention and revealed promising results in the reduction of PLSP [5]. The PRM, which is performed immediately after the operation, mechanically increases the intraperitoneal pressure and assists the removal of the remaining CO2 in the body.
The semi-Fowler position, defined as a body position at 30° head-of-bed elevation, has been shown to be beneficial in increasing intra-abdominal pressure [6]. However, little is known regarding its advantages when it comes to reducing shoulder pain after LS.
Aim
In the current study, we aimed to investigate the impact of semi-Fowler positioning in addition to the PRM on PLSP.
Material and methods
Patient selection
A total of 106 patients aged between 18 and 70 years who presented with an American Society of Anesthesiologists (ASA) physical status score of 1 and 2 and who were scheduled for gynaecologic LS for non-malignant pathologies (e.g., hysterectomy, myomectomy, sacrocolpopexy, cystectomy, etc.) in Istanbul Health Sciences University, Kanuni Sultan Suleyman Education and Research Hospital, between January 2017 and February 2018 were consecutively included in this randomised, double-blinded, prospective study. Patients with previous lung and shoulder surgery, chronic shoulder and epigastric pain, chronic emphysema and pneumothorax were excluded. In addition, women who were pregnant at the time of the study, those unable to express active pain and patients requiring concomitant upper abdominal surgery were not included.
Before randomisation, all eligible subjects received standardised verbal and written information from a research fellow, and written informed consent was obtained from all patients. Using random allocation software (www.randomization.com), the subjects were randomly assigned to a control group receiving no PRM in which abdominal gas was evacuated using passive exsufflation or to one of two intervention groups: group 1 involved patients who received the PRM, which consisted of five manual pulmonary inflations where each positive pressure inflation was done for 5 s at a maximum pressure of 40 cm H2O in the neutral position, and group 2 comprised patients to whom the PRM was applied with a body position at 30° head-of-bed elevation (semi-Fowler position). The study protocol was approved by the Institutional Ethics Committee (KAEK/2017.3.3) and registered with the National Ministry of Health, Health Sciences University (Turkey, Istanbul); the study was performed in accordance with the most recent version of the Helsinki Declaration.
Anaesthesia and surgical procedure
Because a standardised anaesthesia protocol was applied to all patients, 0.03 mg/kg of midazolam intravenously was administered for premedication. General anaesthesia was induced with intravenous propofol 2 mg/kg, fentanyl 1 mg/kg and 0.8 mg/kg rocuronium and was then maintained with sevoflurane 2–3 vol%. Ventilation was performed in a volume-controlled mode at a tidal volume of 7–9 ml/kg. Positive end-expiratory pressure (PEEP) was not used for any patient. All LS procedures were performed by the same surgical team that was experienced in laparoscopic abdominal surgery.
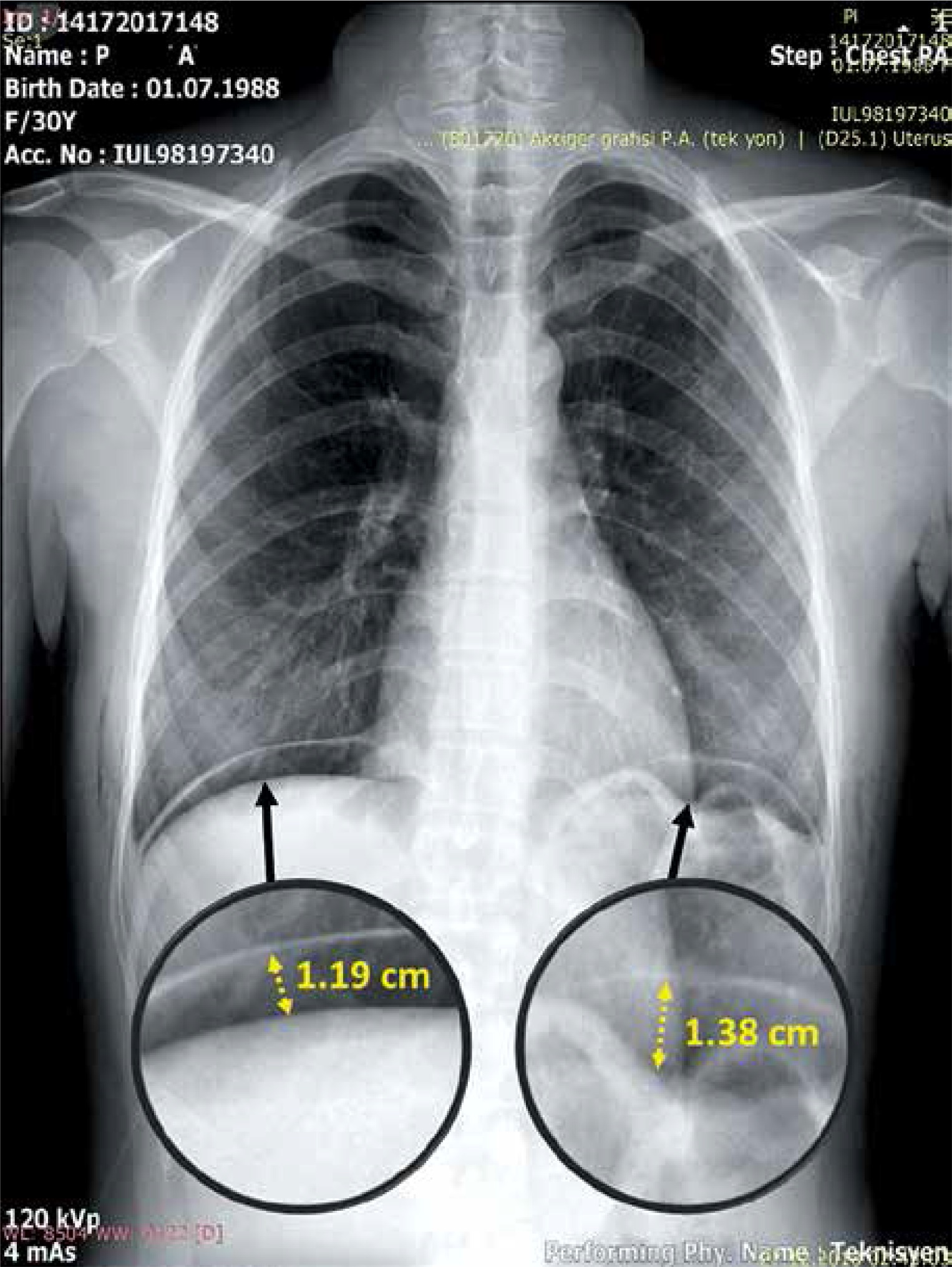
All patients underwent a multiport laparoscopic procedure comprising a 12-mm optical port placed at the umbilicus, 5-mm additional operating ports placed in the lower left and right quadrants and a 5-mm suprapubic port. The intra-abdominal pressure was kept at 12 ml during the procedure. Trendelenburg positioning at 15–20° was applied to each patient. Lateral ports were removed following the surgery, and intra-abdominal gas was evacuated through the main umbilical port. A randomisation envelope was then opened to identify the study group of the index patient. The main port was removed following gas evacuation in the control group. In group 1, the main port was removed following the PRM and following the PRM in the semi-Fowler position in group 2. Upright posteroanterior (PA) chest X-ray imaging was performed in all patients at the postoperative 24th h, and the height of the gas bubble under each hemi-diaphragm was measured to estimate the residual gas volume; their sums were recorded (Photo 1).
Primary and secondary outcomes
The intensity of PLSP was the primary outcome measure. The wound pain score, the height of the residual pneumo-peritoneum at 24 h postoperatively, the analgesic requirements, the time of unassisted ambulation, the time of oral intake and the time of return of bowel function were secondary outcomes. A blinded investigator recorded postoperative data regarding postoperative wound and shoulder pain at postoperative 6, 12 and 24 h using a visual analogue scale (VAS) based on a 0–10 scale, with 0 meaning no pain and 10 the most intense pain ever experienced. The radiologist who calculated the pneumoperitoneum height was also blinded. Dexketoprofen trometamol (50 mg i.v.) was administered as a rescue analgesic to patients with VAS > 4 pain.
Statistical analysis
Statistical analyses were performed using IBM SPSS 20.0 software (SPSS Inc., Armonk, NY, USA). Continuous variables are expressed as mean ± standard deviation (SD), discrete variables as median (range) and categorical variables as number and percentage. The Kolmogorov-Smirnov test was used to assess the normal distribution of the data. For group comparisons, an independent analysis of variance (ANOVA) was used. The Tukey test was performed for the posthoc analysis. The χ2 test was used to compare categorical variables. A p-value smaller than 0.05 was accepted as statistically significant. Power calculations based on our pilot study with 33 patients to detect a significant difference in postoperative 6th hour PLSP scores indicated that at least 31 patients were needed in each group (G power 3, Dusseldorf University).
Results
Patient characteristics, laboratory measurements and surgical duration were similar among the three groups (Table I). The PLSP scores in group 1, group 2 and the control group at postoperative 6 h (5.71 ±0.86, 5.28 ±0.84 and 6.61 ±0.91, respectively, p < 0.001), 12 h (4.41 ±0.83, 4.01 ±0.82 and 5.32 ±0.97, respectively, p < 0.001) and 24 h (3.24 ±0.78, 2.44 ±0.73 and 4.34 ±0.85, respectively, p < 0.001) were significantly different among the groups. At all time intervals, the lowest PLSP scores were recorded in patients who received the PRM in the semi-Fowler position compared with those receiving the PRM in the neutral position and the controls. The wound pain score at 6 h postoperatively was significantly lower in the controls compared with patients receiving PRM in the semi-Fowler position or in the neutral position (6.07 ±0.95 to 6.94 ±0.97 and 6.73 ±0.98, respectively, p < 0.001 for all; Table II). However, at the postoperative 12th and 24th h, wound pain scores were similar across the three groups. The number of patients receiving rescue analgesics was significantly higher for the control patients compared with patients who received the PRM in the semi-Fowler position or in the neutral position (27 to 11 and 9, respectively, p = 0.024).
Table I
Baseline characteristics of the study population
Table II
Postoperative wound and shoulder pain scores (VAS)
| Parameter | Group 1 (n = 33) | Group 2 (n = 32) | Control group (n = 41) | Overall p-value |
|---|---|---|---|---|
| WP at 6 h | 6.73 ±0.98 | 6.94 ±0.97 | 6.07 ±0.95 | 0.002b,c |
| WP 12 h | 5.33 ±0.92 | 5.56 ±0.91 | 4.83 ±0.86 | 0.0456 |
| WP at 24 h | 3.58 ±1.02 | 3.94 ±0.86 | 3.68 ±0.95 | 0.381 |
| PLSP at 6 h | 5.71 ±0.86 | 5.28 ±0.84 | 6.61 ±0.91 | < 0.001a,b,c |
| PLSP at 12 h | 4.41 ±0.83 | 4.01 ±0.82 | 5.32 ±0.97 | < 0.001a,b,c |
| PLSP at 24 h | 3.24 ±0.78 | 2.44 ±0.73 | 4.34 ±0.85 | 0.002a,b,c |
| PRRA, n (%) | 10 (30) | 7 (22) | 27 (61) | 0.024b,c |
The height of the pneumoperitoneum (17.21 ±3.24 mm to 7.97 ±3.06 mm and 3.03 ±1.34 mm, respectively, p < 0.001 for all) and time of unassisted ambulation (17.27 ±1.61 h to 15.55 ±1.35 h and 14.43 ±1.43 h, respectively, p < 0.001 for all) were significantly higher in the control group compared with those who received the PRM in the semi-Fowler position or in the neutral position (Table III). The lowest height of pneumoperitoneum was recorded in patients who received the PRM in the semi-Fowler position. The time of oral intake, time of return of bowel function, and duration of hospitalisation were similar across the groups.
Table III
Secondary outcomes
| Parameter | Group 1 (n = 33) | Group 2 (n = 32) | Control group (n = 41) | Overall p-value |
|---|---|---|---|---|
| Pneumoperitoneum [mm] | 7.97 ±3.06 | 3.03 ±1.3 | 17.21 ±3.2 | 0.001a.b.c |
| Time of ambulation [h] | 15.5 ±1.5 | 14.4 ±1.4 | 17.27 ±1.6 | 0.001a.b.c |
| Time of oral intake [h] | 14.3 ±3.1 | 14.4 ±3.2 | 14.34 ±3.2 | 0.972 |
| Time of bowel function [h] | 18.32 ±2.6 | 17.94 ±2.4 | 16.8 ±2.6 | 0.084 |
| Hospitalization [days] | 1.93 ±0.6 | 2.01 ±0.5 | 2.03 ±0.6 | 0.146 |
Discussion
The present study is the first to demonstrate that when compared with the PRM in the neutral position and no PRM, the PRM in the semi-Fowler position seems to better evacuate the remaining intra-abdominal CO2 and provides a significantly lower PLSP for up to 24 h following laparoscopic gynaecologic procedures. In addition, the PRM in the neutral position also provides a significant reduction in PLSP intensity compared with no PRM, albeit lower than the PRM with a semi-Fowler positioning. Moreover, the height of the pneumoperitoneum and time to unassisted ambulation were also significantly reduced when the PRM was applied in the semi-Fowler position.
Enhanced recovery after surgery (ERAS) is a multimodal approach that was introduced to standardise the surgical process by preventing surgery-related trauma and organ dysfunction, with the main goal of ERAS being to reduce hospital length of stay; this programme mainly focuses on decreasing perioperative stress, resumption of gastrointestinal function, achieving satisfactory pain control and obtaining early mobilisation. Here, minimally invasive techniques provide enhanced recovery following surgery by preventing surgery-related trauma, preventing surgical pain and decreasing the length of hospital stay. Several new methods that are shown to enhance procedure safety, including inferior epigastric artery damage during the introduction of ancillary trocars in gynaecologic laparoscopic procedures, have also been established recently [7, 8]. We believe that the results of the current study are more valuable in terms of achieving ERAS.
The introduction of LS by Philippe Mouret in 1987 was a major advance in the history of surgery and was accepted as a revolution in the surgical armamentarium. Since then, LS has been performed successfully for various kinds of surgical procedures, even in emergency situations. Compared with conventional laparotomy, LS is associated with a more favourable postoperative course. The LS provides early mobilisation and accordingly reduces the risk of thromboembolism. Recent data indicate that LS in women for gynaecologic benign diseases does not require any mechanical or pharmacological thromboprophylaxis in the absence of risk factors although thromboprophylaxis is still of concern in patients undergoing LS for gynaecological malignancies [9, 10]. In the current study, we applied medical thromboprophylaxis only to patients with additional risk factors.
Although the exact mechanism in the development of shoulder pain has yet to be identified, 35–80% of patients undergoing laparoscopic procedures experience shoulder pain for up to 72 h following the operation [11]. Irritation of the phrenic nerve caused by distension-induced neuropraxia, acid intraperitoneal milieu and residual intra-abdominal CO2 are believed to be major contributors to shoulder pain development following LS [4, 12]. Jackson et al. reported that subdiaphragmatic gas volume and the surface area of the gas in contact with the diaphragm were directly related to the severity of pain [3]. Similarly, Sabzi Sarvestani et al. and Song et al. observed a significant relation between the residual pneumoperitoneum and intensity of shoulder pain in patients scheduled for laparoscopic cholecystectomy and gynaecologic procedures, in which patients with no or mild residual pneumoperitoneum had lower pain scores [13]. In another study that included patients scheduled for laparoscopic cholecystectomy, the authors reported that patients in the NO2-induced pneumoperitoneum group experienced less postoperative pain compared with those in the CO2-induced pneumoperitoneum group, indicating the responsive role of insufflated CO2 gas in the development of postoperative pain [14]. In addition, a number of trials conducted in patients undergoing LS found reduced shoulder pain with more effective gas efflux, indicating that shoulder pain observed after LS was mainly derived from CO2 retention within the abdomen [15, 16].
Several interventions have been proposed to decrease post-laparoscopic shoulder pain, particularly addressing the remaining postoperative gas volume. Reducing the remaining gas volume and decreasing phrenic nerve stimulation by administering several drugs are the most used methods in these studies. Tsai et al. investigated the role of a postoperative intra-abdominal injection of 25–30 ml/kg of normal saline solution to expedite the removal of residual CO2 and reported a 40.7% reduction in the ratio of patients with shoulder discomfort and epigastric pain [17]. With the intention of decreasing residual gas volume, the placement of a subdiaphragmatic gas drain has been investigated in several studies; however, no significant benefit was derived from this intervention in reducing PLSP [18]. The implementation of intraperitoneal local anaesthetic to reduce PLSP has been investigated in a number of trials. A meta-analysis including these randomised controlled trials revealed that the application of intraperitoneal local anaesthetics was associated with a decreased incidence of shoulder pain and postoperative opioid consumption [19]. Trials investigating the potential benefits of reduced or gasless laparoscopy and laparoscopy with decreased insufflation pressures demonstrated reduced postoperative pain scores by the use of low-pressure pneumoperitoneum but no change in PLSP with gasless laparoscopy [20, 21]. In addition, studies investigating the administration of nonsteroidal anti-inflammatory drugs (NSAIDs) or corticosteroids to reduce PLSP reported these drugs as having some efficacy in terms of pain and recommended their use only when other interventions applied to reduce pain had failed [22]. Although many of the aforementioned techniques have provided some benefits to decrease PLSP, their implementation and application in daily use seem impractical because of the time-consuming pattern of these interventions, additional costs and their potential adverse effects, which might have a deleterious impact on recovery in the postoperative period.
The PRM involves a series of positive pressure ventilations after the completion of the laparoscopic procedure and allows for the efflux of residual intra-abdominal gas by increasing the intra-abdominal pressure. As a practical, less time-consuming and costless technique, the PRM gained popularity among anaesthesiologists regarding its likely effects in reducing PLSP. Application of the PRM increases the intrathoracic pressure and causes a downward shift of the diaphragm, which further increases the intra-abdominal pressure and improves the outward efflux of the remaining gas. Studies have shown that a low-pressure PRM (40 cm H2O) was sufficient to remove the residual gas from the peritoneal cavity [23]. Substantial data indicate that the PRM improves postoperative pain scores and reduces pain intensity from 61% to 31% among patients who have undergone laparoscopy surgery for various reasons. A previous study conducted by Phelps et al. revealed that the PRM might effectively remove residual CO2 from the abdominal peritoneal cavity and accordingly lead to decreased intra-abdominal acidosis, and phrenic nerve and peritoneal irritation [2]. More recently, Güngördük et al. found that the PRM, with a positive pressure of 40 cm H2O applied at the end of surgery, significantly reduced the incidence of shoulder and upper abdominal pain, as well as pain scores at 12 and 24 h postoperatively [24].
Intra-abdominal pressure of about 5–7 mm Hg is accepted as normal for non-obese individuals, with higher baseline levels in morbidly obese patients of about 9–14 mm Hg. In the semi-Fowler position, where the head of the bed is elevated 30–45°, the intra-abdominal pressure measured through the bladder is higher than in the supine position [25]. A previous study conducted by Cheatham et al. demonstrated up to a 4-mm-Hg increase in intra-abdominal pressure when the head of the bed was elevated from the supine position to 30° [26]. Another study by Vasquez et al. showed that a gradual increase in intra-abdominal pressure occurred when the body position was gradually elevated [6]. Although current scientific data are limited regarding the role of semi-Fowler positioning in decreasing PLSP, the elevated intra-abdominal pressure gained by semi-Fowler positioning may facilitate the outward efflux of the remaining abdominal gas and consequently lead to a decrease in PLSP.
To the best of our knowledge, the present study is the first to demonstrate an improvement in PLSP gained by semi-Fowler patient positioning, which provides additional benefits to what is achieved with PRM alone. Despite the data clarifying the role of PRM in decreasing the PLSP, information regarding the semi-Fowler patient position and its impact on PLSP is still lacking. The limited data concerning the semi-Fowler position typically focus on the relation of intra-abdominal pressure and its relation with semi-Fowler positioning. Our results increase the knowledge regarding both the semi-Fowler position and PRM. Our results reveal that the remaining postoperative CO2 is better evacuated when the semi-Fowler position is accompanied with the PRM compared with PRM alone. Our findings also indicate a lower degree of pneumoperitoneum when using semi-Fowler positioning. Our results reveal that the remaining postoperative CO2 is better evacuated when the semi-Fowler position is accompanied with the PRM compared with PRM alone. In view of this, we suggest that achieving increased intra-abdominal pressures using the semi-Fowler position in addition to PRM, which consequently leads to increased outward efflux of the remaining CO2, provides less phrenic nerve irritation and less diaphragmatic stretching, resulting in less PLSP. Implementation of this rapid, simple and costless intervention will likely provide less PLSP and decrease the postoperative administration of analgesics and opioids, leading to a more rapid recovery and discharge in patients undergoing LS.
The current study has several limitations. The mean age of the study population was relatively low because we conducted the study on patients undergoing gynaecologic procedures. Implementation of semi-Fowler positioning for different types of surgery and in patients with comorbidities would provide more information regarding the efficacy of this intervention. Although analgesics can significantly reduce pain perception, unfortunately, the amount of analgesics administered in the current study was not recorded. The follow-up for pain scoring was only maintained for 24 h; shoulder pain persisting for up to 7 days has been reported previously. Moreover, measurement of intra-abdominal pressure was not performed.
Conclusions
The present study demonstrated that a simple intervention called semi-Fowler positioning in addition to the PRM significantly reduces post-laparoscopic shoulder pain and has an efficacy lasting up to 24 h. In addition, semi-Fowler positioning reduces residual abdominal gas and the time to unassisted ambulation. We suggest that these beneficial effects of semi-Fowler positioning in addition to the PRM are mainly derived from its potential to better evacuate the remaining CO2 following a laparoscopic procedure. The use of this simple intervention to reduce post-laparoscopic pain will likely improve comfort in patients undergoing LS.