Introduction
Infertility is a major global problem of reproductive health. It is defined as the inability of sexually active couples to achieve pregnancy after 12 consecutive months of unprotected sex [1, 2]. Unfortunately, in many countries, infertility is under-diagnosed. It is estimated that 15% of all couples are infertile, and it is identified that a male factor plays a role in about half of the cases [3].
Furthermore, about 70% of cases of male infertility are idiopathic [2], and multiple factors are associated with the rest, such as genetic, hormonal, inadequate lifestyle, psychological stress, pro-inflammatory cytokines, as well as sexually transmitted infections (STIs), including Chlamydia trachomatis (CT) [4, 5]. CT is an intracellular Gram-negative bacterium that causes infertility, although it may also cause urethritis and prostatitis in men [6, 7]. In male infertility, there is considerable variability in the rate of CT infection, ranging from 0 to 90.3%, and, in general, its prevalence is high in developing countries, such as Mexico [7].
Infections impair male fertility by different mechanisms including damaging spermatogenesis and loss of sperm function [5], and induce immunological responses where pro-inflammatory cytokines and other immunoregulatory molecules are involved by interacting with cell types [8, 9], causing chronic inflammation and damage to spermatozoa [6, 8]. There are few reports concerning the relationship between CT infection, alteration in seminal parameters [10], and elevated levels of pro-inflammatory cytokines as causes of male infertility [11].
For this reason, this study aims to investigate the CT infection and its effects on seminal parameters and cytokines in asymptomatic patients with teratozoospermia.
Material and methods
Study design and population
The present study was conducted at the “Hospital Militar de Especialidades de la Mujer y Neonatología” of the National Defense Ministry (SEDENA), Mexico City.
The Institutional Human Research Ethical Committee approved the protocol and the informed consent forms. All experiments were examined and approved by the appropriate ethics committee and therefore were performed in accordance with the ethical guidelines of the Declaration of Helsinki, and the official Mexican Standard NOM-012-SSA3-2012.
One hundred four semen samples were obtained between January and November 2016 from military men aged 22 to 49 years old. Men were eligible for participation if they 1) were male partners from couples attending the clinic for inability to conceive within at least one year of unprotected regular sexual intercourse, 2) underwent sperm parameters analysis, and 3) provided semen by masturbation. Additionally, a clinical examination was done.
Semen analysis and criteria
Specimens were allowed to liquefy at room temperature for 30 minutes; then, their macroscopic and microscopic examinations were performed according to the World Health Organization (WHO) [1]. The men were considered to have teratozoospermia if the percentage of spermatozoa with normal morphology was ≤ 4%.
Detection of Chlamydia trachomatis by PCR
Semen samples were collected, and DNA extraction was performed using the DNeasy Blood and Tissue Kit (QIAGEN Ltd., U.K.), according to the manufacturer’s instructions. The amplification was carried out using specific primers KL1 and KL2 of CT [9]. The β-globin gene was used as a positive control for DNA extraction and PCR methods.
Cytokines in seminal plasma
Cytokine determinations were performed on seminal plasma (dilution 1 : 1) per duplicate, using sandwich enzyme-linked immunosorbent assay (ELISA) for the pro-inflammatory cytokines interleukin (IL)-1β (range: 8-1000 pg/ml), IL-6 (range: 24-1500 pg/ml), IL-8 (range: 16-1000 pg/ml), tumor necrosis factor α (TNF-α) (range: 31-2000 pg/ml) and interferon γ (IFN-γ) (range: 8-3000 pg/ml), as well as for the anti-inflammatory cytokines IL-4 (range: 16-1000 pg/ml), and IL-10 (range: 23-3000 pg/ml) (PeproTech, USA). Standard curves were developed for each cytokine according to the manufacturer’s instructions.
Statistical analysis
The frequency of CT infection was expressed as a percentage. Descriptive statistics were used for comparison of cytokines from infertile men. For continuous data, the nonparametric Mann-Whitney U test was applied for the contrast of seminal parameters and cytokines from CT-infected versus non-CT infected men. Data was analyzed by SPSS statistical software, version 24 (IBM Corp., USA) and Microsoft Excel (Windows 10). In all cases, a statistical significance was assumed when p < 0.05.
Results
In this study, a ratio of 33/104 (31.7%) asymptomatic teratozoospermic patients were positive for CT infection.
Table 1 summarizes seminal parameters in non-CT-infected and CT-infected asymptomatic patients with teratozoospermia. Interestingly, CT-infected men showed an increased pH in semen. The concentrations of seminal cytokines were high in the population studied (Table 2). The levels of pro-inflammatory cytokines IL-1β and IL-6 in the CT-infected group were higher than in the non CT-infected group (Table 3).
Table 1
Seminal parameters in the population studied
[i] Values are media ± SD. Significance refers to Mann-Whitney test for difference between groups; the significance level is p ≤ 0.05. The normal parameters are those considered in the WHO laboratory manual for the examination and processing of human semen, Handbook, 5th ed., WHO 2010. CT – Chlamydia trachomatis
Table 2
Descriptive statistics of seminal pro-inflammatory cytokines in the population studied
[i] Concentration of cytokines reported by aPolitch et al., 2007, bMoretti et al., 2008, cOmu et al., 1999, dSeshadri et al., 2009, eJiang et al. 2016, fMartínez-Prado and Camejo, 2009 for comparison. IFN-γ – interferon-γ, TNF-α – tumor necrosis factor-α, IL-4 – interleukin-4, IL-1β – interleukin-1β, IL-6 – interleukin-6, IL-8 – interleukin-8. Values are median (range) in pg/ml in all results, except the reference values of Omu et al., 1999, which are mean ±SD.
Table 3
Levels of seminal pro-inflammatory cytokines in non-Chlamydia trachomatis (CT)-infected and CT-infected patients
Discussion
Recently, infection and inflammation of the male reproductive tract have been recognized as severe risk factors of male infertility, where CT infection is among the most prevalent sexually transmitted disease in the world [12-14]. This study examined the relationship between CT infection and its effects on seminal parameters and inflammatory markers.
Firstly, a CT infection was found in 31.7% of the semen samples from asymptomatic teratozoospermic men. This prevalence rate is very similar to other reports from Mexico and Latin America, which demonstrated a prevalence of 31.9% [7], and 38.6% [15] in infertile patients, respectively; while in a specific population with teratozoospermia the prevalence was reported to be 35% [7].
In terms of sperm quality, according to the WHO criteria [1], the population herein studied was similar to other reports [10, 16, 17] because they also presented a higher pH value related to the CT infection (pH = 7.65 vs. 7.94). Recent findings suggest that CT infection may influence a change in pH to alkaline values in the female reproductive tract [18]. It has been observed that an alkaline pH favors a shift in the seminal microbiota, such as Lactobacillus, in healthy men [19]. Microbial imbalance harms semen parameters, including sperm motility and morphology, and the host becomes susceptible to other infections and diseases [19].
Concerning the immunological response, the results are consistent with other studies that have reported the presence of high levels of diverse cytokines in seminal plasma from infertile men, such as the pro-inflammatory cytokines IL-6 [20-23], TNF-α [18, 19, 21, 22, 25], IL-8 [19, 25, 26], IL-1β [20, 25], and IFN-γ [29], as well as the anti-inflammatory cytokines IL-4 [24] and IL-10 [30], among others [29, 30]. As in the case of most infections, the immune system is a crucial element in the body’s attempts to eradicate pathogens such as Chlamydia trachomatis, which infect the epithelial cells and produce tissue damage. CT infection is characterized by clinical manifestations from subclinical disease to a robust inflammatory response; unfortunately, 50% of men are asymptomatic which may lead to repeated transmission [6, 14]. Chronic inflammation by infections can lead to urethritis, epididymitis, epididymo-orchitis, and potentially prostatitis and infertility in men [6, 8, 31]; nevertheless, this process has been poorly studied.
Interestingly, the activation of immunological responses due to infection was evidenced in this study, as well as others. Other authors have suggested that the CT infection often causes tissue lesions that stimulate IL-1, which in turn activates polymorphonuclear cells (PMN) and macrophages, and subsequently, the production of IL-6, IL-8, IL-10, TNF-α, and IFN-γ is induced [8].
The IL-6 level in the seminal plasma has also been observed to be higher in infertile men [17, 33] compared to fertile men [34, 35]; however, the results found herein are the highest so far reported. Other authors have suggested that IL-6 is involved in lipid peroxidation (LP). This conclusion was confirmed due to the detection of a byproduct (malondialdehyde, MDA) added to IL-6, simultaneously [36]. These reactions activate oxidative stress, which contributes to male infertility [8].
It is essential to consider that the population studied here consisted of infertile military men, whose condition contributes to presence of several neurochemical, endocrinological, and immunological alterations due to stress, as reported by other authors in military communities [36, 37]. This may also have contributed to modulated inflammatory cytokine levels. For example, studies on hypercortisolemia in military trainees suggest that this hormone also contributes to infertility due to decreases of testosterone by the repetition of psychological stress [37], and more in socially dominant subjects [38]. In addition, cortisol has been found to increase IgE synthesis in response to IL-4, which suppresses the TNF-α production by monocytes [37]. The CT infection probably is chronic and accompanied by other pathogens in semen which are responsible for altered pro-inflammatory cytokine levels and an inadequate response of Th2 cytokines such as IL-10 and IL-4.
Furthermore, both low and non-significant levels of IFN-γ and TNF-α were found. This suggests that most of these patients were suffering from chronic infection with CT, as reported by Feodorova et al. [10]. It is proposed that IFN-γ participates in the activation of the innate immune response at the beginning of the infection [6, 38]. CT infection exerted its effect on motility at high concentrations, as reported by other authors [39]; hence, it may be assumed that this cytokine is no longer protecting against the chronic CT infection.
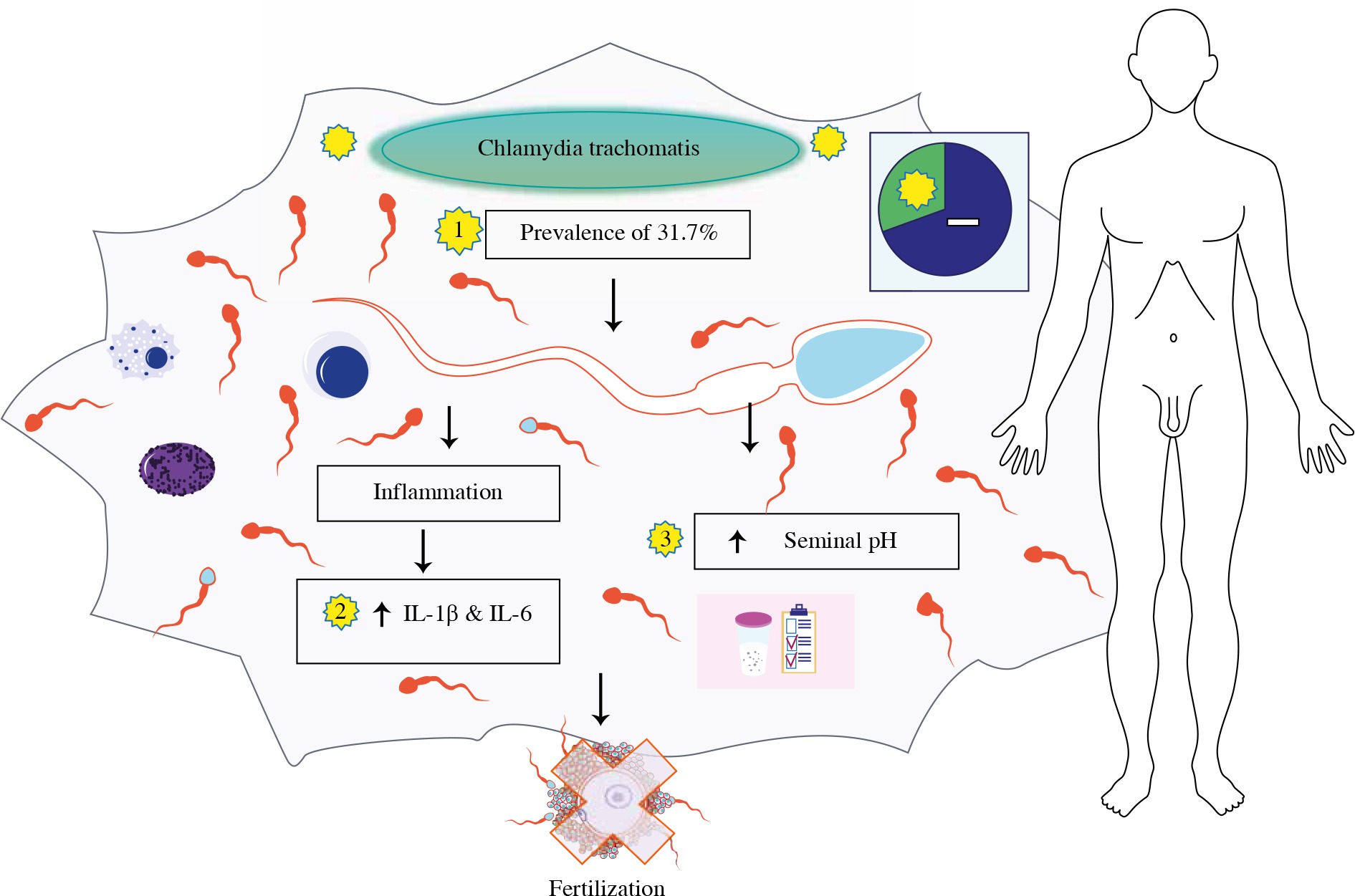
Taken together, the results suggest a strong pro-inflammatory response and a possible chronic CT infection, which can cause effects on the health of men and lead to pathologies such as chronic prostatitis with subfertility [40]. In conclusion, CT infection causes immunological responses because it increases IL-1β and IL-6, also increasing seminal pH (see Fig. 1), suggesting a potential role of infection and inflammation in asymptomatic patients with teratozoospermia.
Fig. 1
Chlamydia trachomatis infection increases seminal pH, also interleukin (IL)-1β and IL-6 pro-inflammatory cytokines in asymptomatic patients with teratozoospermia. Image modified from Motifolio Toolkit licence (http://www.motifolio.com)