
Dear Editor,
We would like to present a case of a 65-year-old female admitted to a gastroenterology and hepatolo-gy department for the optimization of Crohn’s disease treatment – the patient developed antibodies to inflixi-mab. The patient was malnourished, with body mass index 17.5 kg m–2 (body weight 45 kg). Haemoglobin (Hb) concentration at admission was 110 g L–1 and over 4 days it dropped to 100 g L–1. The following day the Hb concentration was 66 g L–1 (error 1). There were no signs of bleeding. The patient did not present any signs or symptoms of anaemia (error 2). The decision to transfuse the patient with 2 (error 3) units of red blood cell (RBC) without buffy coat (error 4) was made. The RBC transfusion was carried out over approximately 3 hours (error 5) in the evening hours (error 6). Shortly after completion of transfusion of the second RBC, the patient developed acute respiratory failure. Urgent anaesthesiology consultation was requested. The patient was found with dyspnoea, tachypnoea (40 breaths min–1), peripheral oxygen saturation (SpO2) 88% on an oxygen mask with a reservoir (15 L min–1), and crackles audible over the entire chest. The patient had tachycardia (120 bpm) and hypertension (blood pressure 160/90 mmHg). Lung ultrasound revealed B profile in all lung points and fluid in the pleural cavities (4 cm on the right side, 1 cm on the left side). The arterial blood gas analysis revealed pH 7.44, pCO2 31.8 mmHg, pO2 54 mmHg, HCO3 22.9 mmol L–1, BE –2.6 mmol L–1, Hb 134 g L–1. Considering the patient’s low body weight, the large volume of transfused RBC (600 mL), age (suspicion of heart failure), and absence of symptoms suggesting alternative post-transfusion reaction, transfusion-associated circulatory overload (TACO) was diagnosed. Furosemide was given (20 mg IV), and the patient was cathe-terized with a resulting urine output of 1000 mL. The patient’s respiratory status improved within 30 min., oxygen therapy was reduced to 5 L min–1, SpO2 was 97%, and the respiratory rate dropped to 18 min–1. After stabilization of the patient the following examinations were ordered: brain natriuretic peptide (pro-BNP) (4293 pg mL–1), C-reactive protein (36.4 mg L–1), haemoglobin (129 g L–1), and computed tomography examination of the chest (Figure 1).
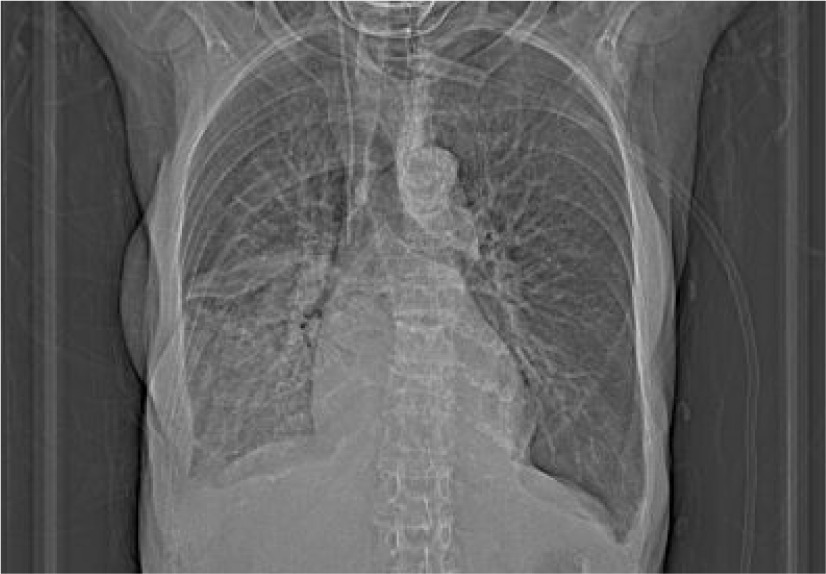
FIGURE 1
Computed tomography examination of the chest showing fluid in interlobar fissures with accompanying atelectasis, fluid in pleural cavities – 2 cm bilaterally, lobar pneumonia
After 3 h another bolus of 20 mg of furosemide was given. Pro-BNP on the 2 successive days was 9411 and 18128 pg mL–1 (reference range < 125 pg mL–1), therefore a cardiology consultation was requested: echo examination revealed normal sized chambers, left ventricle ejection fraction of 60%, and mode-rate mitral and tricuspid regurgitation; a suggestion of intensification of diuretic therapy was made.
This case report shows a series of errors leading to life-threatening TACO. The first error was the fact that the low haemoglobin result was likely to have been a pre-analytical error; the patient’s Hb concentration before this spurious result was 100–110 g L–1. Different pre-analytical errors hamper the accuracy of laboratory results: sample clotting, insufficient volume of blood in a test tube, diluted sample, haemolysis, wrong test tube for an intended test, wrong identification label on a test tube, etc. [1, 2]. There were no symptoms of acute bleeding. Taking this into account, the Hb determination should have been repeated. The second error was the fact that the patient did not present any signs/symptoms of anaemia before RBC transfusion. According to clinical practice guidelines from the Association for the Advancement of Blood and Biotherapies, in non-bleeding patients RBC should be transfused at a restrictive threshold (i.e. Hb < 70 g L–1). The decision to transfuse RBC should not be based solely on the Hb concentration; it should take into account symptoms of anaemia [3] or a broader clinical context [4]. The signs and symptoms of anaemia that should be looked for are dizziness, light-headedness, headache, problems with concentration, attention deficit, shortness of breath, tachycardia, hypo-tension, chest pain, and new electrocardiogram changes. Cardiological and respiratory symptoms should be present despite attempts to improve tolerance of anaemia in patients through optimization of haemodynamics (adequate cardiac output) and oxygenation (liberal oxygen therapy aiming at SpO2 100%/pO2 200 mmHg) [5]. In patients hospitalized in the intensive care unit, in whom neurological impairment or sedation may preclude the diagnosis of neurologic symptoms of anaemia, an algorithm based on anaerobic markers of metabolism may be used [5]. These markers, called physiological transfusion triggers, reflect the balance between global oxygen delivery and consumption. The following anaerobic markers of metabolism can be used: arterial-venous oxygen difference, oxygen extraction ratio, mixed venous oxygen saturation, central venous oxygen saturation, and lactate concentration. The third error was transfusion of 2 RBC units in a single transfusion episode. It has been suggested that the Hb concentration and signs/symptoms of anaemia should be rechecked after transfusion of a single RBC [6]. The fourth error was transfusion of RBC without buffy coat. The modern approach to RBC transfusion is the use of leukoreduced RBCs, what decreases the risk of febrile non-haemolytic transfusion reactions due to the presence of leukocyte-derived cytokines [7], transmission of cytomegalovirus [8] and Epstein-Barr virus [9], alloimmunization, and impaired perfusion caused by cytokines released by leukocytes. The type of transfused RBC was of particular importance in this patient, who was prone to anaemia, with potential requirement for RBC transfusion and alloimmunization with human leukocyte antigens, and who was receiving biological treatment for her primary diagnosis. The fifth error was transfusion of a large volume (600 ml) of RBC over a relatively short period of time (3 h). Colloids are characterized by nearly 100% intravascular expansion effect; therefore, infusion of large volumes over a short period of time leads to increased pulmonary capillary pressure, causing cardiogenic pulmonary oedema in patients at risk. In patients at risk of TACO, transfusion of a single RBC should be extended [10]. A single unit RBC transfusion can last up to 4 hours according to the Polish regulations [11]. The sixth error was the fact that this elective RBC transfusion was performed outside normal working hours, with lower staff levels than in normal working hours. The Serious Hazards of Transfusion report from 2005 showed that 37% of transfusion errors occur outside normal working hours [12]. The post-transfusion Hb concentration (129 g L–1) confirms that in this case over-transfusion of RBC occurred.
The presented case report shows that there is an urgent need to educate clinicians on the appropriate indications for RBC transfusion and proper management of the transfusion procedure, to reduce the risk of severe post-transfusion reactions.