








Introduction
Congenital malrotation of the intestine is due to obstruction of the intestinal tube rotation during embryonic development, which is complicated by intestinal obstruction or volvulus [1]. Intestinal malrotation is more common in the neonatal period, often with bile-like vomiting and typical X-ray findings, and the diagnosis is not difficult [2]. The pathogenesis of congenital malrotation is that during embryonic intestinal development, abnormal rotation around the superior mesenteric artery leads to a series of pathological changes such as intestinal volvulus, duodenum and jejunum compression. The pathological types are usually complicated and the clinical manifestations are specific. Sex is not obvious, so misdiagnosis often occurs, which poses a serious threat to the health and life safety of newborns [3, 4].
Congenital malrotation of the intestine is mainly treated by surgery, and the common surgical method is laparotomy and cecal lysis [5]. In the laparoscopic Ladd procedure, the size of the visual field is related to the success or failure of the operation. It is believed that the biggest difficulty in the operation is to identify the abnormal anatomical relationship [6]. Older patients should be selected for the laparoscopic-assisted Ladd procedure. The abdominal cavity operation space is relatively large, and the anatomical relationship is relatively clear. After the operation starts, the subumbilical incision is the first choice to observe the abdominal cavity and the operation hole. You can choose the left lower abdomen, which is convenient for surgical operation [7]. Intestinal malrotation is mainly based on loosening the adhesion zone and rearranging the position of the intestine [8]. Based on this, in order to explore the short-term effects of laparoscopic-assisted surgery and the effect on gastrointestinal function in patients with congenital intestinal malrotation, the current research results are reported as follows.
Aim
The aim of this study was to evaluate the short-term curative effect of laparoscopic assisted surgery on patients with congenital intestinal malrotation and its effect on gastrointestinal function in very low birth weight infants
Material and methods
General information
All records of patients’ identities included in this study will be kept in hospitals as required, and public reports on the results of the study will not disclose all records of patients’ identities. All patients had informed consent before being enrolled in the group, fully communicated with the patients before the experiment, introduced the content and process of the experiment, related risks and possible adverse reactions, signed the informed consent form after obtaining the consent of the patients, and informed the patients of the test results in strict accordance with the experimental procedures. We selected 100 patients with congenital intestinal malrotation who underwent surgery in our hospital in the period from June 2019 to June 2021 as the subjects of this prospective study. According to the random residue grouping method, they were divided into a control group and an observation group with 50 cases each. Indications for laparoscopic surgery: (1) No serious heart and lung function damage. (2) The coagulation function is normal. (3) Abdominal distension is lighter. (4) Malrotation of the intestine is suspected before surgery, but the diagnosis is questionable. Before the start of the study, the patients and their families were asked to sign an informed consent form in accordance with the principles of voluntariness, confidentiality, benefit and harmlessness. General data such as gender and age of the two groups of patients had no effect on this test, as shown in Table I.
Table I
Comparison of general information between the two groups (n, x ± SD)
Inclusion and exclusion criteria
Inclusion criteria: 1) All patients in this study met the diagnostic criteria of Chinese Open Fracture Diagnosis and Surgical Guidelines (2019 Edition) [9] for the diagnosis of congenital intestinal malrotation; 2) Patients were admitted to the hospital with an age of ≤ 28 days, suffering from congenital intestinal malrotation, confirmed by surgery; 3) No history of intrauterine distress and hypoxic asphyxia; the selected patients had good compliance and all informed consent. Exclusion criteria: 4) Patients with other systemic malformations and contraindications to the surgery and drugs used in this study; 5) Patients with severe heart, liver, and kidney dysfunction; 6) In patients with other contraindications to laparoscopic surgery or suspected intestinal strangulation open surgery is directly recommended. Patients with congenital diaphragmatic hernia, abdominal fissure, or umbilical bulge, those who disagree with clinical surgical observation or whose clinical data are incomplete, or those who are not suitable to participate in this study due to other factors.
Method
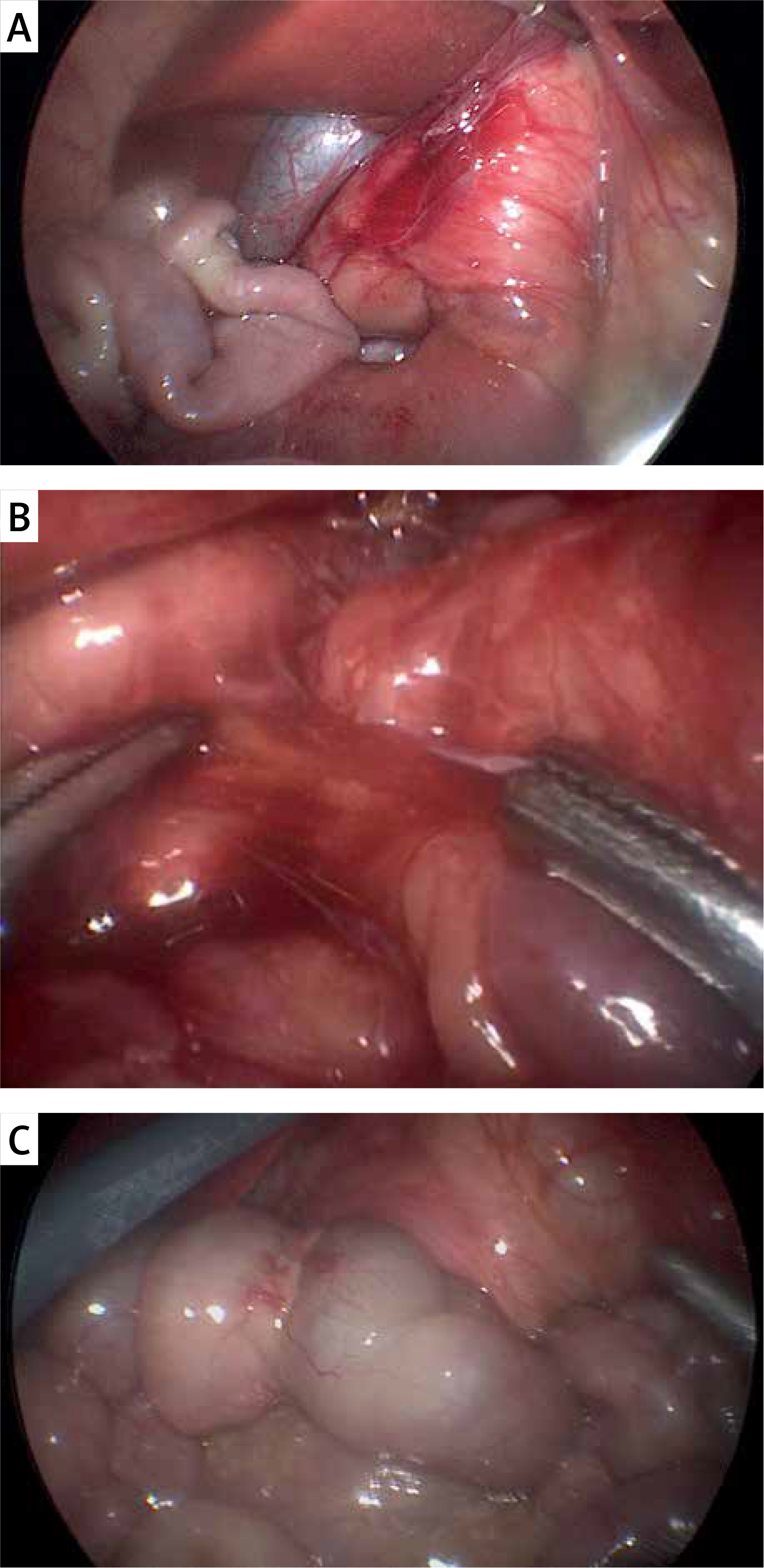
The control group underwent traditional laparotomy. According to the routine operation, the observation group used the laparoscopic-assisted Ladd procedure; that is, all cases were treated with endotracheal intubation and intravenous combined general anesthesia, and the stomach tube and urinary catheter were inserted in the supine position. Routinely disinfect the drape, puncture the lower edge of the umbilicus with a pneumoperitoneum needle, and slowly inject CO2 gas to establish an artificial pneumoperitoneum. The pressure is 6–8 mm Hg. The pneumoperitoneum needle was removed, and a laparoscope with an inner diameter of 5.5 mm was inserted at the same point. The operating forceps and ultrasonic scalpel were inserted into the left and right middle and lower abdomen respectively, and the position of the poke hole was convenient for the operation. During the operation, according to the condition of the bowel disease, the adhesion around the duodenum is first loosened or the torsion of the bowel is rotated and reset, and the Ladd’s cord between the cecum, ascending colon and the right posterior abdominal wall is disconnected with an ultrasonic knife, and the duodenum is released. For all adhesions to the beginning of the empty field, straighten the duodenum and place it in the right abdominal cavity with the small intestine, and place the cecum and colon in the left abdominal cavity. Routinely remove the appendix. Check if there is no bleeding or internal hernia. The pneumoperitoneum is relieved, the CO2 gas in the abdominal cavity is exhausted, the puncture cannula is removed, and the operation is ended (Photo 1).
Follow-up and observation indicators
Surgery indicators: compare the two groups’ operation time (from incision to skin closure), transition to open abdomen, postoperative eating time, discharge time (no vomiting after eating enough), exhaust time, defecation time, bowel sound and recovery time.
Clinical efficacy: According to WHO evaluation, cure: no obvious local tenderness. Significantly effective: clinical symptoms and signs have basically returned to normal.
Effective: The clinical symptoms and signs partially return to normal.
Ineffective: No significant improvement compared with preoperative.
Statistical analysis
All statistical data in this study were entered into the Excel software by the first author and the corresponding author respectively. The included data were tested by the Shapiro-Wilk method. The measurement data conforming to the normal distribution were described by the mean ± standard deviation (x ± SD), and between groups the independent sample or paired sample t test was implemented within the group, and the count data were described in integers or percentages (%), and the χ2 test was used between or within groups. The included data that do not conform to the normal distribution are described by M(QR), using Mann-Whitney-test, and the test level is α = 0.05.
Results
Comparison of general information
There was no statistically significant difference between the two groups of patients in terms of gender, average age, degree of intestinal rotation, birth weight, gestational age, and other general data after testing (p > 0.05) (Table I).
Comparison of surgical indicators and gastrointestinal function
There were statistically significant differences between the two groups of patients in postoperative operation time, hospitalization time, exhaust time, defecation time, postoperative fluid intake time, postoperative general eating time, and bowel sound recovery time (p < 0.05) (Table II).
Table II
Comparison of surgical indicators and gastrointestinal function between the two groups (x ± SD)
Comparison of immune function
There was no significant difference in immune function between the two groups of patients before surgery (p > 0.05), while the comparison of CD8+ and B cells after 1 week of surgery was significantly different. The Observation group was better than the Control group, which was statistically significant (p < 0.05). There was no statistically significant difference in NK cells after 1 week of surgery (p > 0.05) (Table III).
Table III
Comparison of the immune function of the two groups of patients (x ± SD)
Comparison of short-term efficacy
The clinical treatment efficiency of the Observation group was 94.00%, significantly higher than that of the Control group’s 78.00%, and the difference was statistically significant (p < 0.05) (Table IV).
Discussion
The Ladd procedure to relieve obstruction is the first choice for the treatment of congenital malrotation. With the widespread use of laparoscopic surgery and pediatric surgical diseases [10], the laparoscopic Ladd procedure for the treatment of intestinal malrotation has been chosen by more and more surgeons. Compared with traditional open surgery, it has the advantages of a small incision, beautiful appearance, quick postoperative recovery, and small scars. The clinical effect is significantly better than traditional open surgery. Treatment method [11]: the laparoscopic Ladd procedure requires at least 3 puncture holes. There are small scars on both sides of the abdominal wall after the operation. Single-port and single-site laparoscopic technology has been used in pediatric surgery at home and abroad because of its concealed and beautiful characteristics of the scar on the body surface. Various procedures have been developed and satisfactory clinical results have been achieved, but there is no report on the clinical effect of the single-port single-site laparoscopic Ladd procedure [12–14]. Traditional laparotomy is not suitable for newborns because the incision is too large [15]. The promotion of the laparoscopic Ladd procedure is very slow. The main reason is that it is difficult to operate the intestinal tube of laparoscopic reduction and torsion. The safety and effectiveness of laparoscopic surgery have not been recognized by the majority of physicians. There is a lack of confidence in the treatment effect, and the main concern is the occurrence of intestinal volvulus and adhesive intestinal obstruction after malrotation [16].
This study showed that the two groups of patients had statistically significant comparisons between the operation time, hospitalization time, exhaust time, defecation time, postoperative fluid intake time, postoperative general eating time, and bowel sound recovery time after surgery. The difference in CD8+ and B cells after 1 week was obvious and the observation group was better than the control group. The clinical treatment efficiency of the observation group was 94.00% significantly higher than that of the control group 78.00%. The difference was statistically significant. It shows that the effect of the laparoscopic Ladd procedure for congenital malrotation is better, which can effectively improve the gastrointestinal function of patients after surgery and the abdominal incision is hidden after surgery. We performed the laparoscopic Ladd procedure on newborn patients with congenital malrotation, and compared the clinical efficacy of the laparoscopic Ladd procedure between two groups. There was no significant difference between the two groups in the postoperative food intake and postoperative hospital stay [17]. Loosen the grasping forceps after full electrocoagulation. If there is bleeding, use warm salt water to wash and accurately determine the bleeding point before electrocoagulation to stop the bleeding. In addition, when loosening the fascia, keep a certain distance from the intestine to avoid scalding the intestine caused by electric heat conduction. After perforation [18]: the clinical effect of open surgery is positive, but it requires skilled laparoscopic operation technology. Because the operation hole is concentrated in the abdomen, it greatly interferes with the coordination of the left and right hands during the operation and increases the difficulty of the operation [19]. The focus and difficulty of the laparoscopic Ladd procedure is the reduction of intestinal volvulus. We believe that the left operating forceps grasp the transverse colon, and the right operating forceps grasp the left small mesenteric or mesenteric root of the left abdomen and turn counterclockwise to the right abdomen. Reduce the difficulty of resetting, and continuously adjust the angle and position of the endoscope and operating forceps during operation, which can be successfully completed [20]. However, a series of factors such as the application of anesthesia during the operation, the trauma of opening the abdomen, and the stretching of the gastrointestinal tract all inhibit the patient’s gastrointestinal motility, resulting in the patient’s gastrointestinal function movement [21, 22]. In addition, neonates represented by low birth weight infants are unable to convey accurate feelings of fullness or hunger because the nervous system is not fully developed, which leads to relatively short awakening time and they tend to fall asleep or get tired when eating, and cannot tolerate it. Oral feeding method [23]: such patients often have poor recovery of gastrointestinal function after surgical treatment, have feeding difficulties, have relatively long parenteral nutrition, increase the incidence of complications, and generally have a longer total hospital stay.
Conclusions
Although this study is novel to some extent, it also has shortcomings. Laparoscopy-assisted transumbilical single-site surgery has a significant clinical effect on congenital intestinal malrotation, but the specific mechanism has not been studied for a long time. The collected cases came from the same hospital and were poorly represented. Both exclusion and inclusion are subjective, which may lead to biased results. In summary, the comparative study of congenital intestinal malrotation using the laparoscopic Ladd procedure is effective, effectively improving the postoperative gastrointestinal function of patients, and the postoperative abdominal incision is hidden, which provides a certain reference for clinical surgery of congenital intestinal malrotation.