








Introduction
Chronic obstructive submandibular adenitis is a common clinical disease which can cause salivary hypofunction [1]. Sialolithiasis is the most common cause of inflammatory disease of the submandibular glands [2]. Stones with various shapes and sizes can be single or multiple, located proximally or distally in the efferent duct. Stones smaller than 4 mm in diameter can nowadays be successfully removed by sialendoscopy with an 80% success rate [3, 4]. Larger stones may be smashed into pieces in the lumen of the duct, either mechanically or with a laser beam. Despite technological progress, 5–10% of patients with sialolithiasis cannot be treated successfully by sialendoscopy alone [5], especially when a stone is too large or located in the proximal or hilum of the submandibular gland duct. In those cases, complete removal of the submandibular gland may be necessary.
There are limited data evaluating the efficacy and safety of the combined approach to remove posterior sialolithiasis of Wharton’s duct. Here we introduce our experience using the sialendoscopy-assisted intraoral incision approach to treat larger stones located in the proximal or hilum of Wharton’s duct, and the clinical efficacy was evaluated.
Aim
The aim of this study was to evaluate the clinical efficacy of the sialendoscopy-assisted intraoral incision approach to remove large stones located in the proximal or hilum of Wharton’s duct, when sialendoscopy alone has failed.
Material and methods
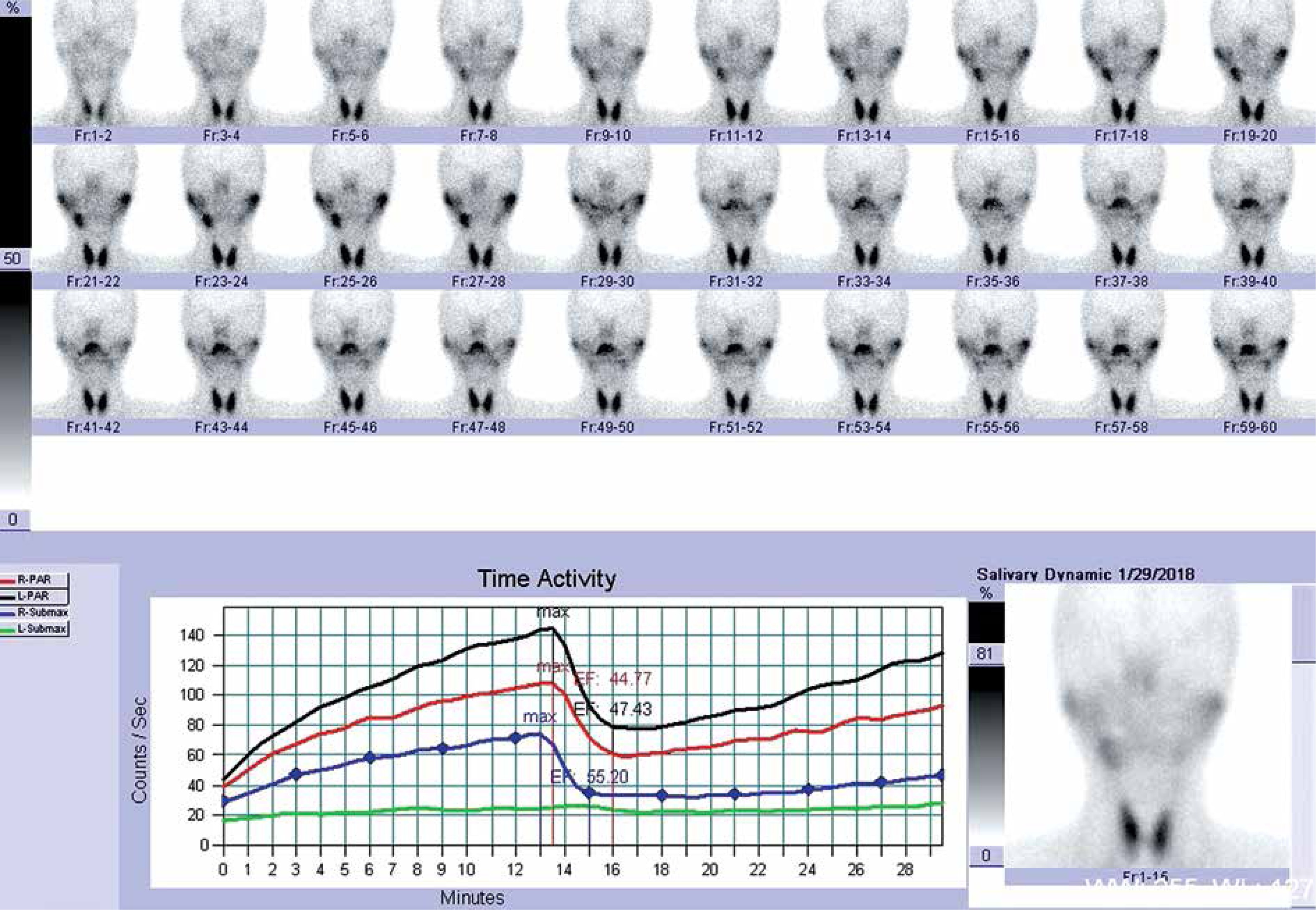
Twenty patients including 12 men and 8 women were included in our study from September 2015 to December 2018. Details of patients are given in Table I. The study was approved by the Ethics Committee of the First People’s Hospital of Foshan, Guangdong province, China. The size of the stones ranged from 4.5 to 10 mm (mean: 5.75). We used a CT scan (Photo 1) for preoperative diagnosis in all patients to ensure the diagnosis. All the stones with a diameter greater than 4 mm were in the proximal part of the submandibular gland duct or hilum. The uptake and excretion function of the involved submandibular glands were quantitatively assessed using technetium-99m pertechnetate salivary gland scintigraphy before and after the operation (Photo 2). Antibiotic should have been used in the acute inflammatory period until the infection was controlled. All patients were admitted to hospital. Routine examinations, including a routine blood test, electrocardiogram and chest roentgenogram, were performed to exclude surgical contraindications. Before surgery, we communicated with patients and their families in detail, informed them of the operation plan and related risks, and signed the consent form for surgery.
Table I
Patient details
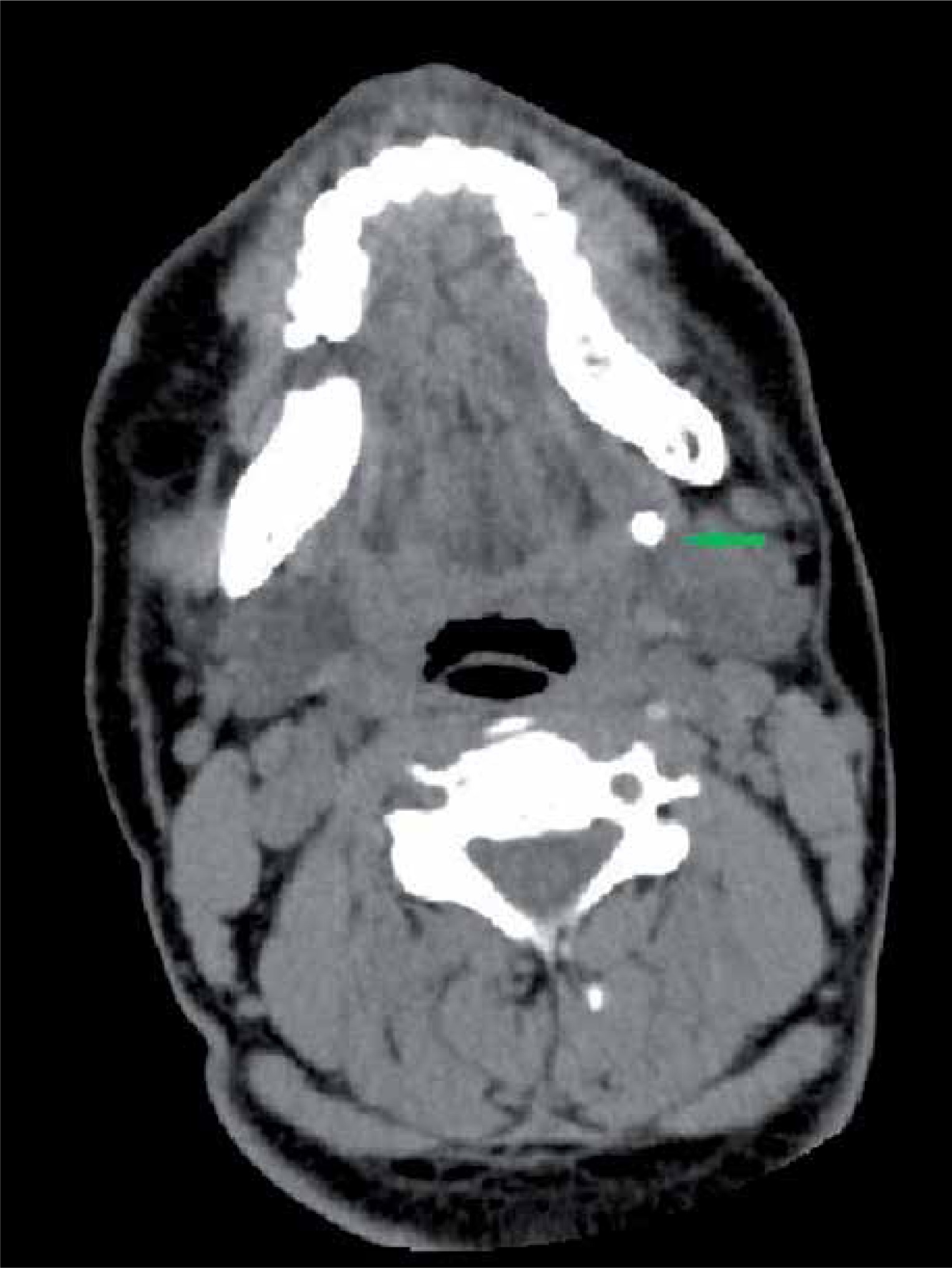
Photo 2
Technetium-99 m pertechnetate salivary gland scintigraphy showing abnormal uptake and excretion of a left submandibular gland before operation
Surgical procedure
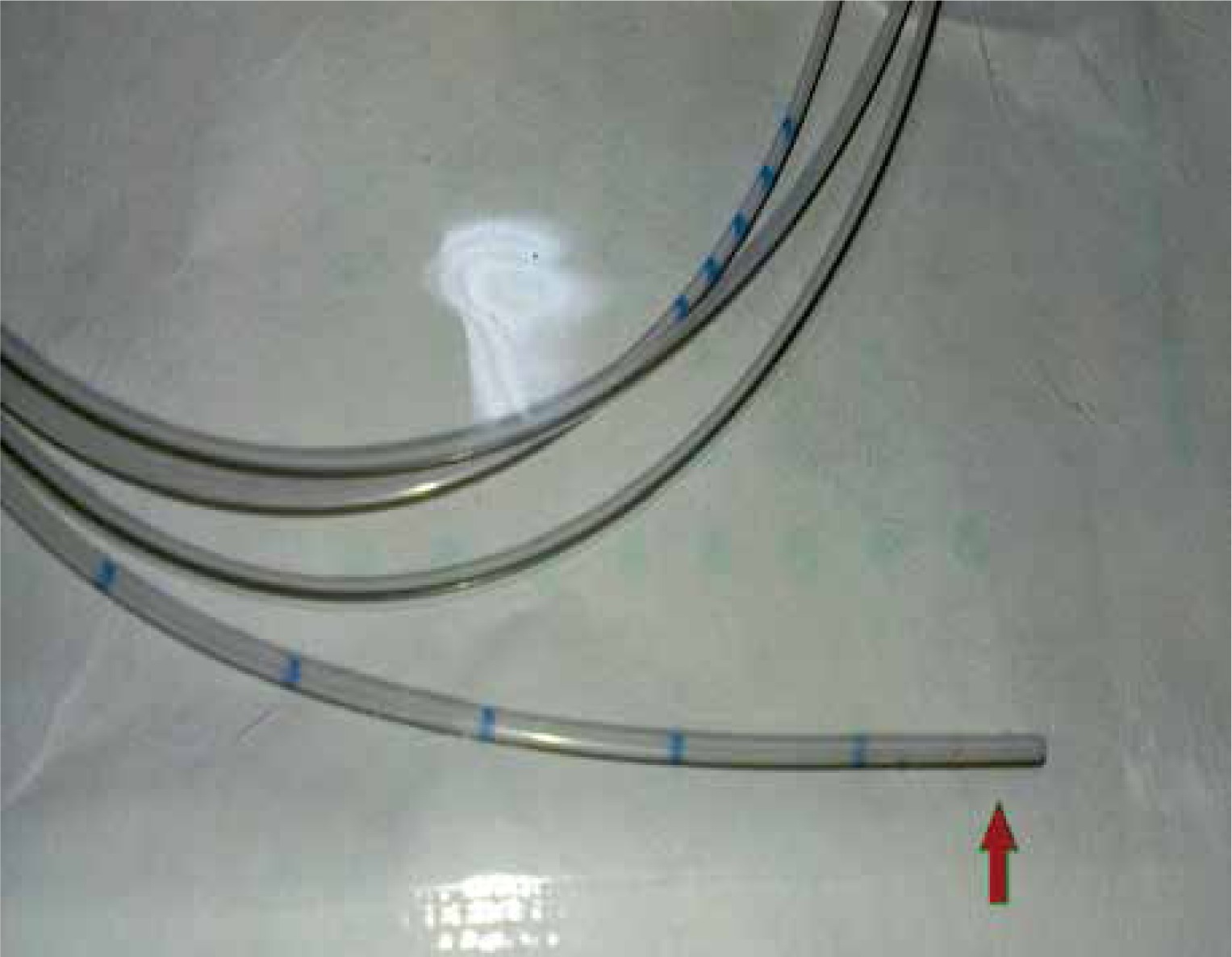
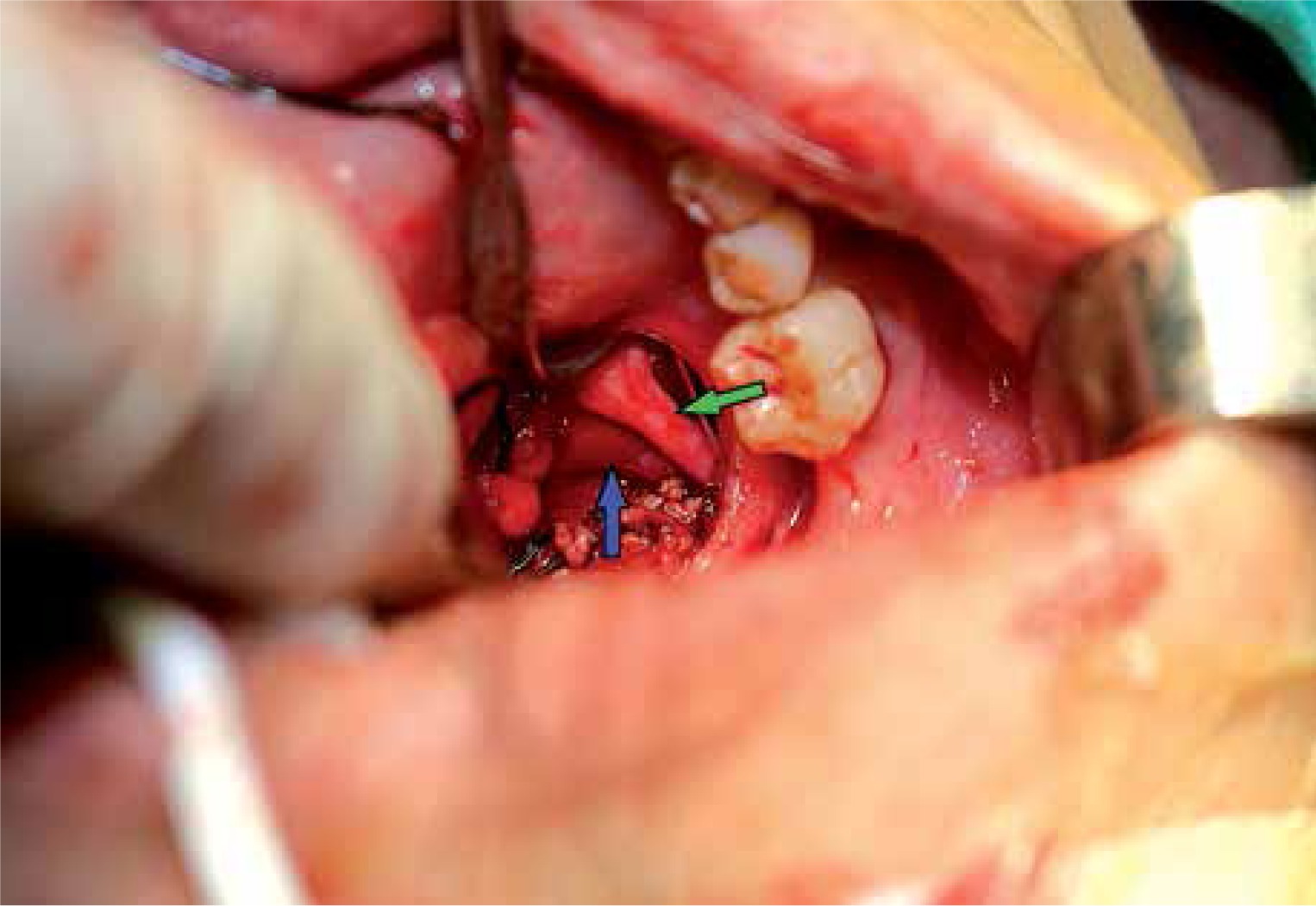
All the operations were performed under general anesthesia. Interventional sialendoscopy was done with a 1.3 mm diameter Examination Sheath and 1.3 mm/1.3 mm diameter Operating Sheath endoscopes (Karl Storz, Tuttlingen, Germany). A salivary duct probe and conical dilator were used to enlarge the submandibular gland duct orifice. Also, an epidural tube (Photo 3) was used as a guide wire for the entrance of the sialendoscopy to the duct [6]. After the sialendoscopy entered into the lumen, an attempt to remove the stone by sialendoscopy alone was made at the first step (Photo 4). If it failed, we changed to the combined approach. A sialendoscopic transillumination light spot was used to localize the stone, and then an intraoral mucosal incision was made over the light spot. During the surgery, the lingual nerve should be identified as it crosses the duct and should not be injured (Photo 5). Under the guidance of sialendoscopy, the duct and stone were easy to find. Then the stone was exposed and removed after incising the wall of the duct. After stone removal, sialendoscopy was used to irrigate the duct with lots of saline in order to clear away the fragments and inflammatory tissue, and at the same time to check the duct to make sure no other stone or fragments remained. Then an epidural tube working as a stent was inserted into the duct through the operation sheath (Photo 6). The duct incision was sutured using 5-0 VICRYL Rapide sutures, then the mucosa incision also was sutured using 5-0 VICRYL Rapide sutures. The stent was sutured in the duct for about 2 weeks to prevent duct stenosis.


Results
By this surgical method, all the stones (Photo 7) were removed successfully, without excision of the submandibular gland in all 20 patients. The success rate was 100%. All patients developed varying degrees of swelling and pain after surgery, which impaired eating and talking. The entire uncomfortable symptom is gradually improved after 1 week of postoperative treatment. No other complications occurred except 2 patients had tongue numbness after the operation, and recovered 3 months later without additional intervention. No swelling or pain appeared during the 3-month to 1-year follow-up. However, during the follow-up period, the clinical examination showed that saliva could be observed from the orifice in 15 patients, with little or no saliva in 5 patients who also were symptom free. Scintigraphy was performed at 6 months after surgery. The results showed that the function of the interventional submandibular glands had been restored to normal in 15 patients (Photo 8), while another 5 had few improvements.


Discussion
Sialolithiasis is the most common cause of submandibular gland sialadenitis, which is a common disease referred to head and neck surgeons. Before sialendoscopy, sialolithotomy and sialadenectomy were the major surgical methods to treat sialolithiasis, while antibiotic drugs were a conservative treatment that may relieve the symptoms. Many complications occurred with sialadenectomy, such as injury to the lingual nerve, facial nerve, hypoglossal nerve, and unaesthetic scars [7, 8]. With a success rate more than 80% if the indication is appropriate [9, 10], sialendoscopy has been proved to be a good choice to treat sialolithiasis, with few complications and gland preservation. But when the stone diameter is larger than 4 mm, and located in the proximal of the submandibular gland duct or hilum, sialendoscopy alone will have a great probability of failure and sialadenectomy is unavoidable. Some techniques may improve the success rate of stone extraction, including extracorporeal and intracorporeal lithotripsy and holmium:YAG laser [11–13]. These techniques can turn the stone into small pieces which can be removed by a wire basket or grasping forceps. It proves to be effective, and allows the treatment of large stones in Stensen’s and Wharton’s ducts with a success rate of 80–90%. But these techniques also have disadvantages, such as being time-consuming and costly, needing special equipment, and being associated with some complications such as ductal wall perforation, and thermal injuries to the duct and the surrounding soft tissue including vessels and nerves [14, 15]. For various reasons special equipment such as the holmium:YAG laser is rarely used in China. So, cases of large stones or impacted/immobile post-hilar submandibular gland stones are still a challenge to surgeons. A sialendoscopy-assisted transcervical incision was made by some surgeons to remove the stones. They believe it is an effective method and also can preserve the submandibular gland [16]. But there also are some disadvantages such as a scar in the skin, and injury to the lingual and facial nerves. Sialendoscopy-assisted trans-oral incision stone retrieval has also been described sparsely in the literature [17]. However, in China, such reports are limited. We have performed sialendoscopy-assisted trans-oral incisions in 20 patients with larger and posterior location of stones in Wharton’s duct in our department. All the stones were removed by this approach, with few complications, gland preservation and no recrudescence of symptoms. So, we believe it is an effective and safe way to remove those larger and posteriorly located stones of Wharton’s duct, and possibly it can serve as an attractive alternative to existing techniques, such as extracorporeal shock wave lithotripsy, for the removal of larger and posteriorly located stones.
Submandibular gland computed tomography, which can evaluate the stone dimensions and locations, is necessary before surgery, and a treatment plan should be developed according to the CT scan. According to our experience, a stone near the papilla or distal from the duct is easier to remove, whether by sialendoscopy or a sialendoscopy-assisted approach, while those that are larger and proximal to the duct seem to be more difficult to remove. Also, it is impossible to remove the stone by sialendoscopy alone if the stone is impacted on the wall of the duct. Of course, the size of the stone is not an absolute standard. Some small stones may not be possible to remove by the endoscope. We failed to remove a posterior calculus with a diameter of about 3 mm by endoscopy alone, because the stone was located in a branch of the duct. However, the stone discharged by itself after the operation, by eating acidic food and massage. The reason is conjectured to be intraoperative mechanical expansion of the duct by sialendoscopy surgery. We also encountered a case of a 6 mm diameter stone in the hilum of the submandibular gland. However, the stone was extracted by sialendoscopy alone. This was a recurring case. Two stones were found by CT scan, one near the papilla, the other with 6 mm diameter located in the hilum of Wharton’s duct. The stones reappeared again after the first surgery with a stone removal 2 years ago. Both stones were removed directly by sialendoscopy alone. The reason is suspected to be that the submandibular duct was dilated during the previous surgery, while repeated obstruction resulted in severer dilation of the duct, which was beneficial to stone removal. We believe that as long as the submandibular gland duct is sufficiently expanded, the stones may be taken out by the endoscope alone, even if the multiple stones are large and located in the hilum.
Some researchers believe that sialolithectomy by a simple transoral mucosal incision approach also can achieve good efficacy [18, 19]. What is the difference between simple transoral mucosal incisions and the endoscopic assisted transoral mucosal incision approach? And which one is better? We believe that stone removal by the simple mucosal incision approach is relatively easy with no special equipment required, and is a good choice for the primary hospital in China, which can also relieve the uncomfortable symptoms of some patients to some extent. Sialendoscopy is a better choice if the conditions permit. In our approach, sialendoscopy was conducted to examine the duct, and then the transillumination light spot was used to localize the stone, while an intraoral mucosal incision was made over the light spot. The combinational approach not only has a certain degree of accuracy compared to the empirical mucosal incision, but also has less tissue isolation and less surgical trauma, and is less time consuming. Also, endoscopy can be used to check the duct to make sure no other stones or fragments have remained, while flushing residuals such as flocs and mucus plugs, to reduce postoperative recurrence after stone removal. According to our experience, a stent may need to be placed in the duct postoperatively to prevent stenosis of the duct and keep it unobstructed. Unlike previous studies, we can also place the stent under the direct view of the endoscope, which is more accurate than the previous experience-based placement in other studies. However, the placement of the stent may cause discomfort to swallow, eat and talk after surgery, which one should be aware of.
The study had some limitations. For example, the number of patients included in this study was limited. Although the function achieved in our study is optimal, the lack of sufficient data for statistical analysis is a limitation of our study. Long-term clinical studies are needed to confirm the clinic effect.
Conclusions
The sialendoscopy-assisted intraoral incision approach to treat large stones located in the proximal or hilum of the submandibular gland duct is effective and safe. The initial clinical outcomes were satisfactory, but the long-term results and functional recovery of the glands need to be investigated later.