
A 69-year-old man with suspected Lyme disease visited an infectious disease specialist in the outpatient clinic. 3 weeks earlier, he felt a painful bite in his left buttock, caused by a tick that was later removed. After several days, significant weakness, drowsiness, chills and muscle pains occurred, followed by a 2 cm red inflammatory infiltration appearing in the location of the bite with crust over the ulceration and enlarged left inguinal lymph nodes (Figure 1 A).
Figure 1
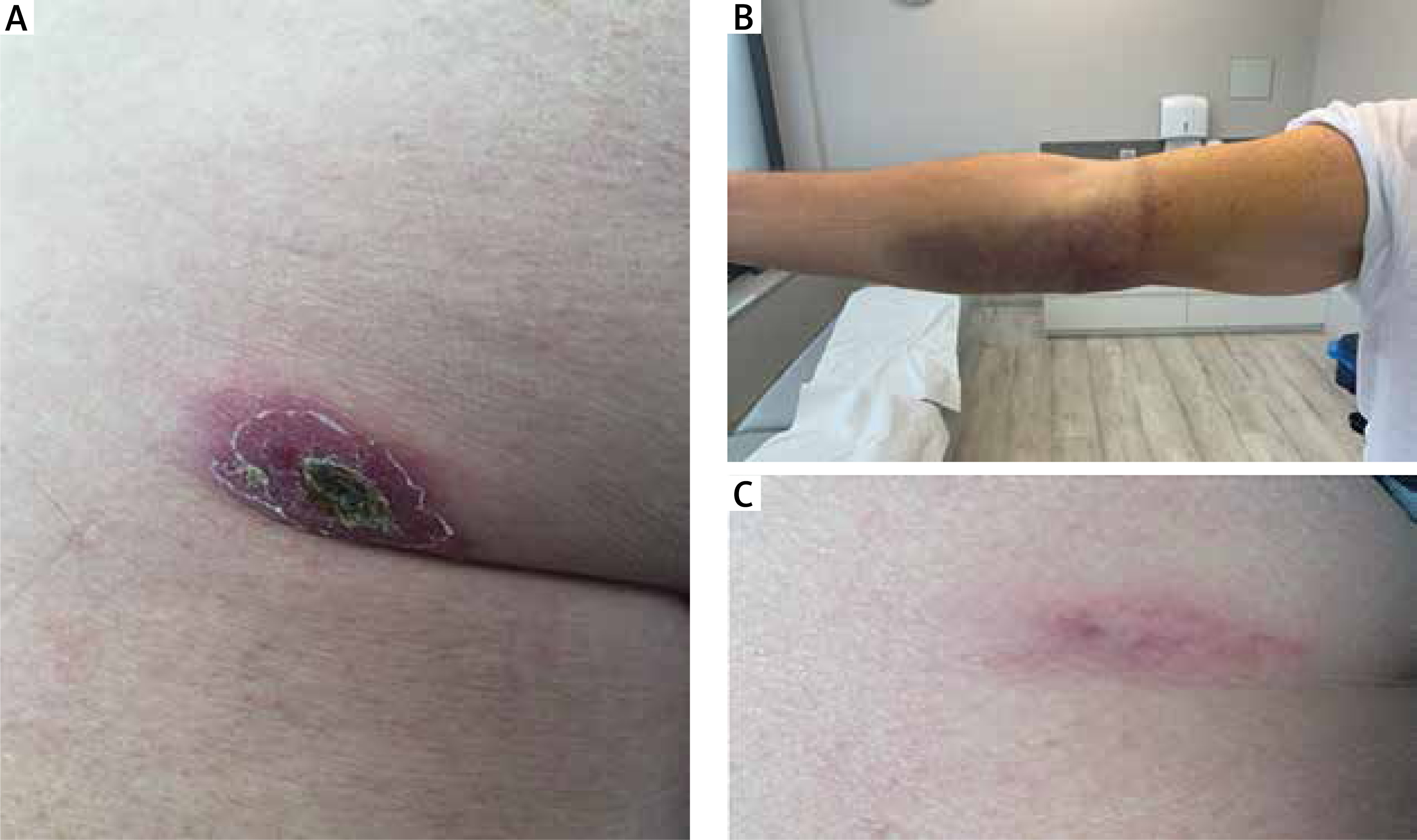
A – Ulceration covered with crust on the left backside. B – Right forearm hematoma. C – Evolution of the skin lesion of the left backside after treatment
The patient was admitted to the Infectious Diseases Ward with suspected tularaemia. Laboratory tests showed deviations of C-reactive protein (CRP) of 37 mg/l, leucocytosis of 12.1 thousand/ql, platelets (PLT) of 449 thousand/ql, creatinine of 1.31 mg/dl. A node enlargement of 32 mm was described in the left groin ultrasound.
Initially, due to the good general condition of the patient and lack of tests confirming tularaemia, the patient was started on doxycycline for 10 days, followed by ciprofloxacin for another 10 days. Differential diagnosis mainly considered proliferation and possible metastases to the nodes due to the patient’s significant history of colorectal cancer 20 years before and a recurrence 15 years before. The carcino-embryonic antigen (CEA) at that time was 3.02 ng/ml; no detectable pathologies were described in abdominal ultrasound. Biopsy or samples from the lymph nodes were not collected for histopathological examination due to an increased risk for laboratory staff working on biological material suspected of tularaemia infection and the need to perform these tests in laboratories with Biosafety Level 2 at the minimum.
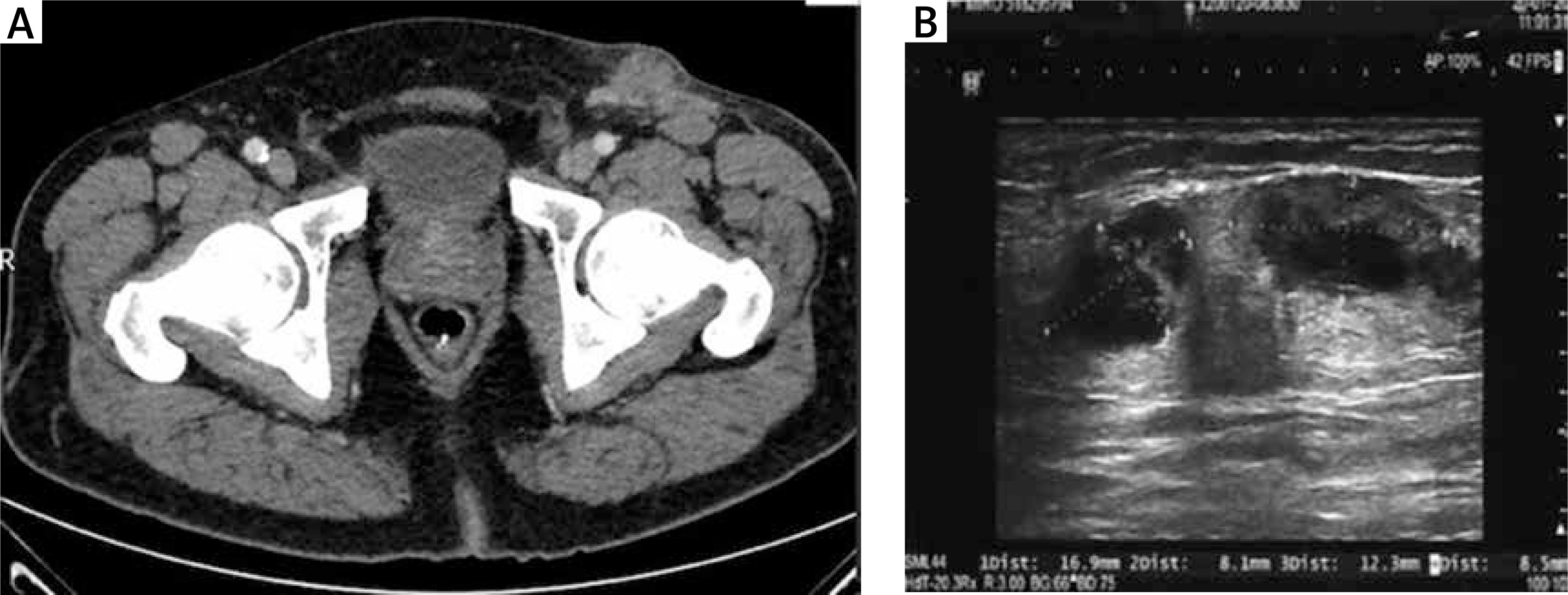
After the National Institute of Public Health of the National Institute of Hygiene (Polish: Narodowy Instytut Zdrowia Państwowy Zakład Higieny – NIZP-PZH) provided positive serological results from blood tests for Francisella tularensis in the classes IgM, IgG and IgA, and following molecular, confirmation of the presence of Francisella tularensis spp. Holoartica, DNA from clinical material collected from the crust covering the skin ulceration, combined with lack of local improvement (persistent left lymphadenopathy with necrosis detected in computer tomography (CT)) (Figure 2 A), intravenous infusion of gentamicin at a daily dose of 4 mg/kg was used in the treatment for 10 days, with no side effects during hospitalization; followed by the recommendation to continue administering ciprofloxacin orally for the next 14 days after being discharged from hospital [1].
Figure 2
A – Lymph node conglomerate in the left groin on CT scan. B – Control left groin ultrasound – regression of the lymph node size after treatment
A few days after discharge from the Ward, the patient returned with extensive hematoma in the right forearm and hard infiltration within the arm (Figure 1 B) – thrombosis was ruled out; coagulation and inflammation parameters were normal – the cause of the hematoma, which eventually subsided in the following days, could not be determined.
In the follow-up visit 2 months later, the patient was feeling well, the skin lesion on the buttock had visibly decreased (Figure 2 C), and so did the inguinal nodes in physical and ultrasound examination (Figure 2 B). Ten months after the end of treatment, the discoloration of the buttock remains.
Tularaemia is a zoonosis which develops in humans after contact with infected mammals (mainly hares), e.g. by skinning the animals, after ingestion of infected food or water, being stung by insect vectors (e.g. flies, ticks, mosquitoes, fleas) or by inhalation into the respiratory tract (bacterium used in bioterrorism). Tularaemia may occur in pneumonic, intestinal, ulceroglandular, oculoglandular, and oropharyngeal form, depending on where the pathogen enters the body. The most common is the ulceroglandular form, also diagnosed in our patient [2, 3]. In general, tularaemia is a relatively rare disease with a potentially severe course (pulmonary form) or a self-limiting disease. Its symptoms can be attributed to other more common diseases, and thus diagnosis of tularaemia is not easy. In Poland, several to 20–30 cases are reported annually [4].
In diagnostics of peripheral lymphadenopathy, we first take into account proliferative and haematological processes, and then infectious diseases. The fact of having been stung by an insect, coupled with the occurrence of an ulcerous skin lesion accompanied by locally enlarged nodes, should raise suspicions of tularaemia.







