
Introduction
Hair loss is reported in 40.3% of the general population (36.86% of men and 43.60% of women) [1]. Alopecia is classified into scarring (with the permanent destruction of hair follicles) or nonscarring [2]. Frontal fibrosing alopecia (FFA) and the classic variant of lichen planopilaris (LPP) are the most common forms of scarring hair loss [3].
Although hair loss may be considered as a cosmetic issue, it is associated with a significant emotional and psychological burden. Patients with hair loss report a loss of confidence, heightened self-consciousness, and low self-esteem [4, 5]. Moreover, psychiatric disorders, such as depression and anxiety, are more common among patients with hair loss compared to the general population [6]. The majority of previously published studies assessed the psychological status in patients with nonscarring forms of hair loss such as alopecia areata or androgenetic alopecia [2, 5, 7]. To date, data concerning the quality of life and psychological status of patients with scarring alopecias have been limited [6].
Aim
The primary aim of the study was to assess: (1) the health-related quality of life, (2) illness perception and (3) psychological distress in patients with LPP and FFA. The secondary aim was to analyse correlations between the above variables and established clinical measures.
Material and methods
All patients over 18 years of age diagnosed with classic LPP or FFA were included in the study. The patients were recruited in several countries between 1 September 2021 and 30 September 2022. The centres were located in Poland, Italy, Mexico, and the South West Nigeria.
The exclusion criteria were as follows: (1) severe comorbidities or chronic diseases which might influence the quality of life; (2) a diagnosis of any psychiatric illness before the diagnosis of LPP or FFA, (3) current treatment with psychotropic drugs; and (4) visual, hearing, language, or cognitive deficits or impairments.
Demographic data such as sex and age as well as the duration of the disease were recorded in all patients. The severity of hair loss in LPP and FFA was assessed with the Severity of Alopecia Tool (SALT) and the Frontal Fibrosing Alopecia Severity Index (FFASI), respectively. The activity of hair loss was evaluated using the Lichen Planopilaris Activity Index (LPPAI). Moreover, hair loss in other hair-bearing areas as well as skin, mucous membrane or nail involvement were assessed. Additionally, in patients with FFA, the presence of facial papules was reported.
Health-related quality of life (HRQoL)
The Dermatology Life Quality Index (DLQI), introduced by Finlay and Khan [8] in 1994, is a self-explanatory survey which measures the impact of skin illnesses on a patient’s life in the previous week. It consists of ten questions regarding the symptoms and feelings, daily activities, leisure, work and school, personal relationships, and treatment as dimensions of life. Each item is scored on a scale of 0 to 3 points. The scale yields the maximum score of 30 [9]. The interpretation of DLQI scores is as follows: 0–1 = no effect; 2–5 = small effect, 6–10 = moderate effect, 11–20 = very large effect, 21–30 = extremely large effect [10].
Disease perception
The Brief Illness Perception Questionnaire (IPQ-B) consists of eight items rated on a scale from 0 to 10. The total score is calculated by summing the scores of all items, with the possible range of 0–80 [11]. In the first five items, cognitive perception regarding the effect on life, duration of illness, control over illness, beliefs about the effectiveness of treatment, and the experience of symptoms are assessed. Items 6 and 8 evaluate emotional aspects including concern about illness and a multifaceted question about mood. In item 7, the degree of understanding of the illness is assessed. The final item includes an open question concerning three most important factors causing the illness. Higher scores indicate poorer illness perception. IPQ-B total scores are further classified as follows: < 42 indicating low experienced threat, 42–49 indicating moderate experienced threat, and ≥ 50 indicating high experienced threat [12].
Psychological distress
The Depression, Anxiety and Stress Scale (DASS-21) is a questionnaire comprising 21 items with 3 subscales in which each item is rated on the 4-point Likert scale (0–3) measuring depression, anxiety and stress [13]. Furthermore, the severities for each dimension of mental health are categorised as normal, mild, moderate, severe and extremely severe [14] (Supplementary Table S1).
Statistical analysis
All statistical analyses were carried out using Statistica 13.1 (StatSoft, Cracow, Poland). The Spearman’s rank correlation coefficient test was used to assess possible linear associations between two continuous variables. The values of p < 0.05 were considered statistically significant.
Results
Patients’ characteristics and detailed results are presented in Table 1.
Table 1
Psychological profile, quality of life and disease perception of patients with classic lichen planopilaris and frontal fibrosing alopecia
In total, 162 women, i.e., 83 women with LPP and 79 women with FFA were enrolled in the study. The mean LPPAI in both groups was 2.32 (0–10). In patients with LPP, the SALT score varied from 5 to 85 (mean: 18). The mean FFASI in patients with FFA was 8.59 (2–17).
In patients with LPP and FFA, the DLQI score ranged from 0 to 18 (mean score: 5) and from 0 to 14 (mean score: 3), respectively. A very or extremely large effect of the disease on the patient’s quality of life was reported in 10% (8/83) of patients with LPP and 4% (3/79) of patients with FFA. In 24% (20/83) of patients with LPP and 15% (12/79) of patients with FFA, the disease had a moderate effect on the patient’s quality of life. In patients with LPP and FFA, positive correlations were observed between the DLQI and LPPAI (r = 0.406, p < 0.001 and r = 0.317, p < 0.01, respectively). Moreover, in patients with LPP, the DLQI positively correlated with the SALT (r = 0.277, p < 0.01) and negatively with the age of the patient (r = –0.228, p < 0.05) (Tables 2, 3).
Table 2
Correlation between DLQI, IPQ-B, DASS-21 and LPPAI, SALT and disease duration in patients with LPP
| DLQI | IPQ-B | DASS-21 depression | DASS-21 anxiety | DASS-21 stress | |
|---|---|---|---|---|---|
| LPPAI | 0.406* | –0.101 | 0.035 | 0.045 | –0.035 |
| SALT | 0.277** | 0.044 | 0.141 | 0.085 | 0.038 |
| Disease duration | –0.009 | 0.115 | 0.061 | 0.138 | 0.185 |
| Age of the patient | –0.228*** | –0.059 | –0.0168 | –0.155 | –0.165 |
Table 3
Correlation between DLQI, IPQ-B, DASS-21 and LPPAI, FFASI, disease duration in patients with FFA
| DLQI | IPQ-B | DASS-21 depression | DASS-21 anxiety | DASS-21 stress | |
|---|---|---|---|---|---|
| LPPAI | 0.317* | –0.296* | 0.105 | 0.098 | –0.094 |
| FFASI | 0.137 | 0.382** | 0.008 | 0.076 | 0.133 |
| Disease duration | –0.017 | 0.115 | 0.176 | 0.260*** | 0.065 |
| Age of the patient | –0.125 | 0.076 | –0.019 | –0.089 | 0.152 |
The mean score of the IPQ-B was 47 and 45 in patients with LPP and FFA, respectively. Specifying, 59% (49/83) of patients with LPP and 61% (48/79) of patients with FFA experienced moderate or high threat. In patients with FFA, positive correlations were found between the IPQ-B and FFASI and eyebrow involvement (r = 0.382; p < 0.001 and r = 0.958; p < 0.001). Conversely, the IPQ-B negatively correlated with the LPPAI (r = –0.296; p < 0.01) (Table 3 and Supplementary Table S3).
A moderate, severe or extremely severe stress level was noted in 42% (35/83) and 30% (24/79) of patients with LPP and FFA, respectively. In 30% (25/83) of patients with LPP and 20% (16/79) of patients with FFA, at least a mild depression level was observed. Only 10% (8/83) of patients with LPP reported a mild or moderate anxiety level. In patients with FFA, the anxiety and stress subscale of the DASS-21 positively correlated with eyebrow involvement (r = 0.320, p < 0.01 and r = 0.360, p < 0.001, respectively) (Supplementary Table S3).
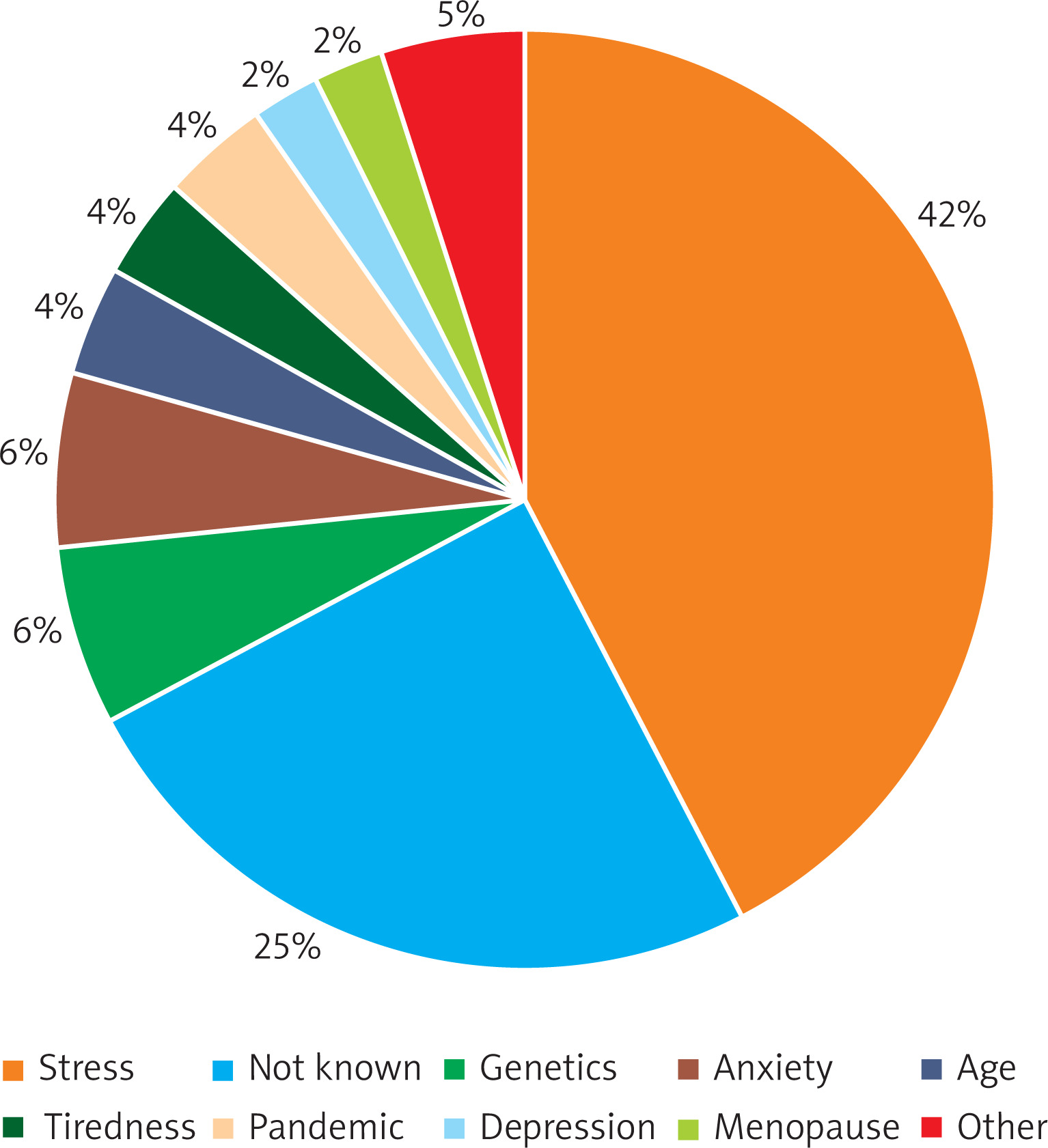
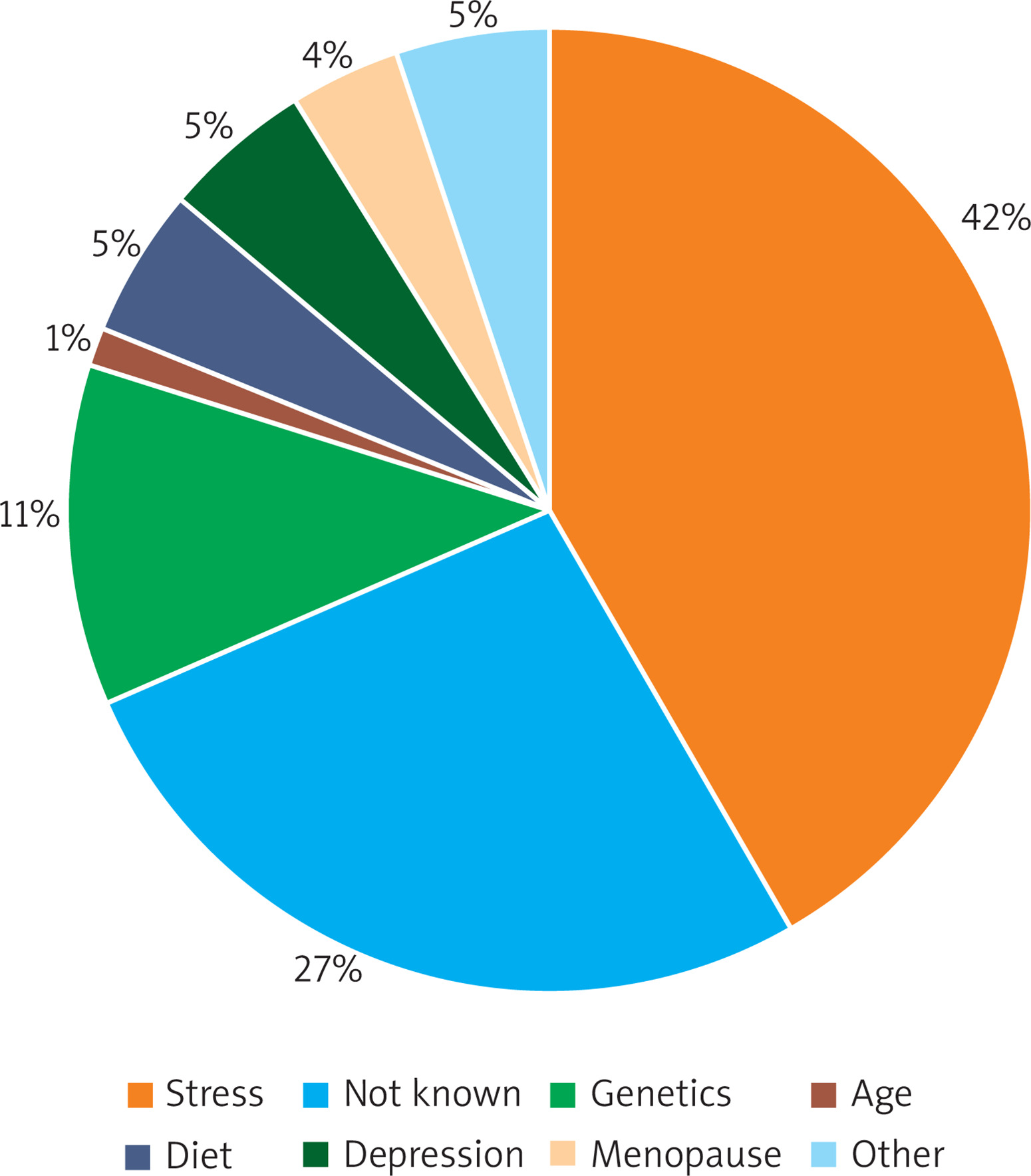
Stress was considered as the most common cause of the disease by 42% (35/83) of patients with LPP and 42% (33/79) of patients with FFA, while a genetic predisposition was reported as a cause of the disease by 6% (5/83) of patients with LPP and 11% (9/79) of patients with FFA. Depression was the third most common reported cause of the disease (2% (2/83) of patients with LPP and 5% (4/79) of patients with FFA) (Figures 1, 2).
No differences were observed in the DLQI, IPQ-B and DASS-21 between patients with or without body hair loss, facial papules, skin, nail or mucous lesions (data not shown).
Discussion
Surprisingly, a limited number of studies analysed the psychological impact of scarring hair loss [15–18]. In the study performed by Katoulis et al. [6], the DLQI was lower in patients with scarring alopecias compared to patients with nonscarring hair loss. This probably resulted from the poorer prognosis of scarring alopecias, their irreversible outcomes, and less effective treatments compared to nonscarring hair loss [15]. The present study showed that LPP and FFA had a negative impact on patients’ QoL. A moderate or very large effect of the disease was reported by 34% of patients with LPP and 19% of patients with FFA. Moreover, 59% of patients with LPP and 61% of patients with FFA experienced a moderate or high threat of hair loss.
Data concerning the relation between the severity or activity of LPP/FFA and the HRQoL or psychological distress are inconsistent. In a study by Alirezaei et al. [19], a higher LPP activity and a higher severity of hair loss were associated with lower HRQoL scores. Chiang et al. [17] described a positive correlation of the LPPAI and depression level. Conversely, Doche et al. [20] and Saceda-Corralo et al. [18] determined no relation between the activity or severity of hair loss and the DLQI or Hospital Anxiety and Depression Score (HADS) in patients with LPP or FFA. In the present study, a negative correlation was found between the HRQoL and the activity of the disease both in patients with LPP and FFA. In patients with LPP, the HRQoL also negatively correlated with the severity of hair loss. Conversely, no correlation was noted between the severity of FFA and the HRQoL. A positive correlation between the activity of hair loss and the HRQoL emphasizes the need of the treatment of LPP and FFA. Effective therapy is essential to stop hair loss but it will also result in improving the QoL.
Similarly to the study of Alirezaei et al. [19], no impact of the duration of the disease on the HRQoL was observed. However, a positive correlation between the duration of the disease and the DASS-Anxiety/DASS-21 was observed.
In a study performed by Nasimi et al. [15] in patients with LPP, age < 45 years was associated with a lower HRQoL. Saceda-Corralo et al. [18] reported a negative correlation between the age of FFA onset and the HADS. In the present study, a negative correlation was observed between the age of the patients and the DLQI in patients with LPP.
Contrary to the studies of Doche et al. [20] and Varghaei et al. [21], we observed no differences in the HRQoL or psychological distress between patients with and without concomitant non-scalp lesions. However, positive correlations occurred between eyebrow involvement and disease perception, anxiety and stress.
It was suggested that scarring hair loss might be a source of significant stress [15]. Indeed, in the present study, at least moderate stress was reported by 42% of patients with LPP and 31% of patients with FFA. Moreover, patients with LPP and FFA considered stress (42%) as the most common cause of the disease. In the study of Saceda-Corralo et al. [18], the patients with FFA also most commonly reported stress as the cause of hair loss. Contrary to stress, the level of anxiety and depression was normal in the majority of patients with LPP and FFA.
The main limitations of the present study are the lack of men with LPP/FFA and no control group.







