








Introduction
Bile duct injury (BDI) is the most serious complication of laparoscopic cholecystectomy (LC), and it is a major unsolved surgical problem. The incidence of BDI is 0.2–0.5% worldwide [1, 2]. Surgeons are constantly trying to find ways and means to reduce the incidence of bile duct and vascular injury. Drawing on the training theories of the aviation and marine industries, many important extrahepatic landmarks have been proposed as intraoperative references [3–9]. Among them, Rouviere’s sulcus (RS) is a classical landmark which is thought to indicate the plane of the common bile duct, and the tip of it points to the cystic duct [4–7]. There are also many landmarks associated with RS [3, 8, 9]. However, there has been much controversy over the definition and classification of RS [10]. Moreover, the plane of Rouviere’s sulcus (RS plane) is an imaginary plane [7], and different surgeons may have different assumptions.
In this department, an extended plane of the hilar plate (hilar plane) was safely used as a landmark and a set of standardized procedures was formulated with reference to the hilar plane during LC and laparoscopic common bile duct exploration (LCBDE) in more than 6000 cases since 2014 [11], including some complex conditions, without bile duct injury.
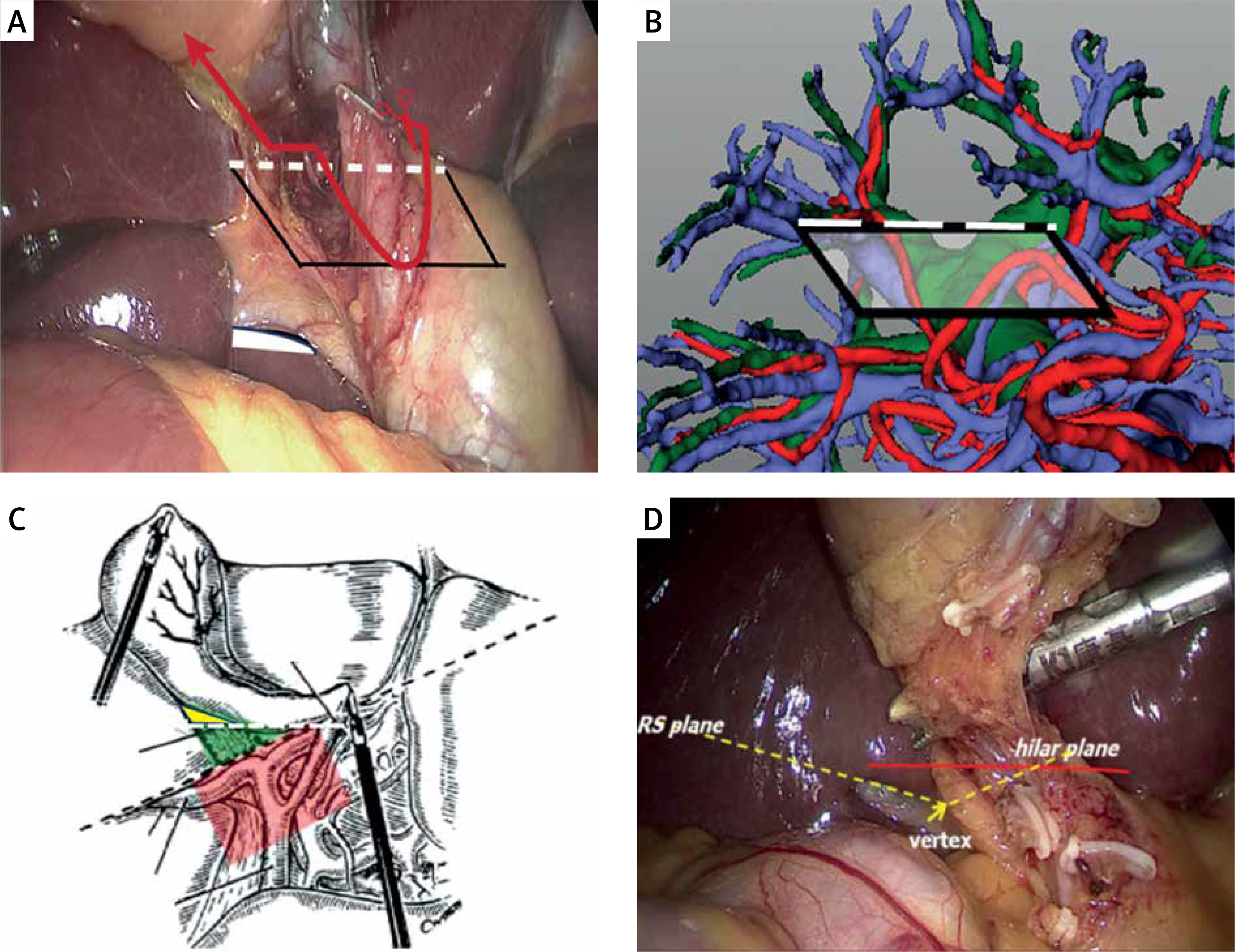
The hilar plane extends from a “start line” which is a horizontally extending line of “the base of segment 4” from left to right across the gallbladder, then down to the hepatocystic triangle (Calot’s triangle) along the peritoneum in front of the common hepatic duct. At the same level, it runs across the gallbladder and intersects the peritoneum of the posterior triangle of the gallbladder. It is a ventral-dorsal plane below the “start line”. The floor of the hilar plane on the left of the gallbladder is the peritoneum of the hilar plate and in front of the common hepatic duct; however, the floor on the right of the gallbladder is imaginary. The plane leaves the “shield” of right hepatic pedicle structures including the aberrant right hepatic artery or ectopic right posterior hepatic duct (Photos 1 A, B).
Photo 1
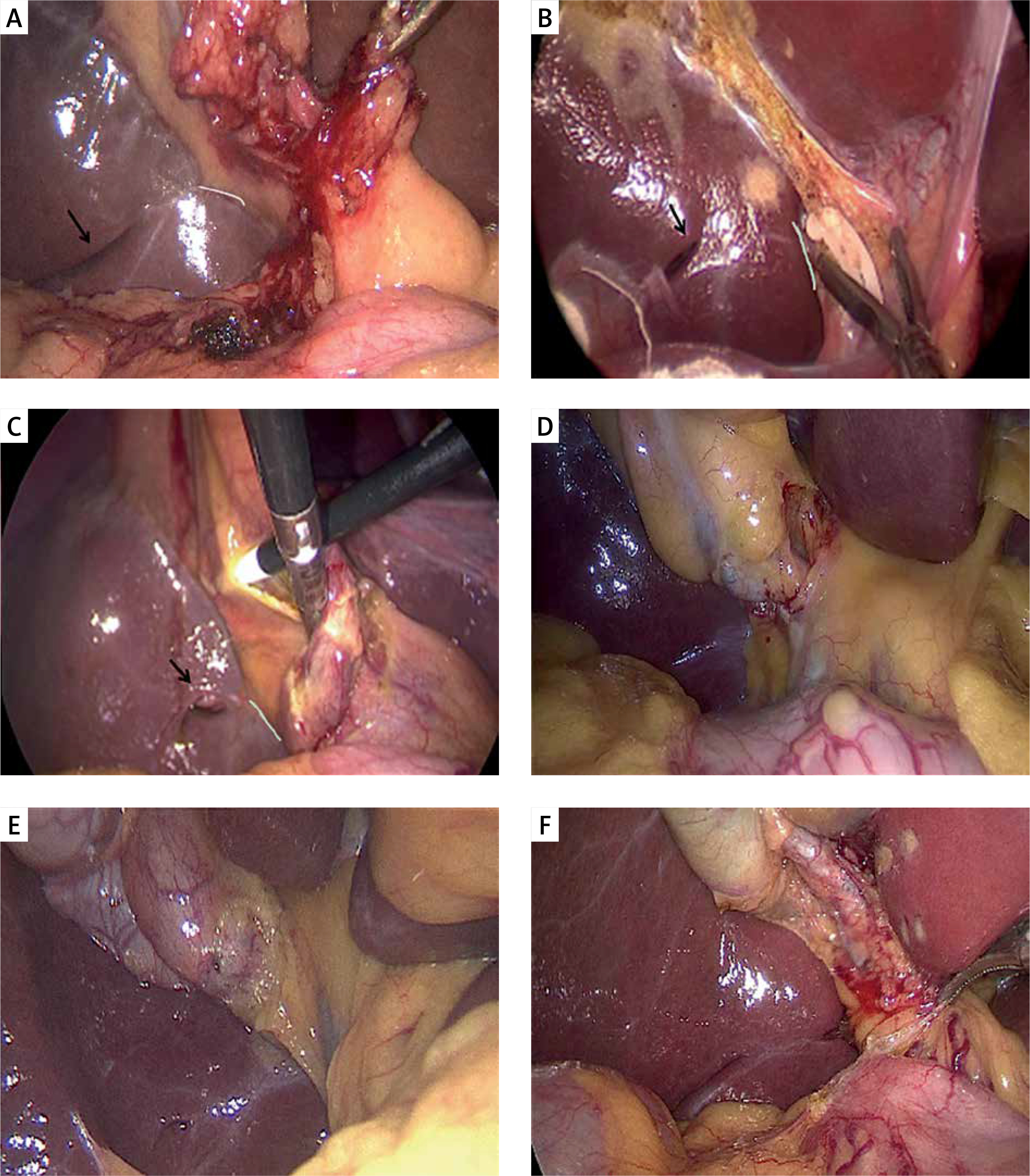
Hilar plane and RS plane. A, B – Diagram of hilar plane. The black arc line marks the arc incisure of the right posterior hepatic pedicle running into the liver; the white dashed line represents the start line, and the black frame shows the hilar plane; the red arc indicates the start of the initial peritoneal dissection of anterior and posterior triangles of the gallbladder in the same plane. C – Classic schematic diagram of RS plane by Hugh and Connor SJ [5], and modified by Wang l. The yellow triangle formed by the start line (white dotted line). D – When the orientation of RS is oblique and pointing superior or the RS roof (yellow dotted line) is significantly lower than the start line (red line), the RS plane should be a curved line rather than a straight line
Aim
In this retrospective observational study, the value of using the hilar plane vs. the RS plane in preventing bile duct and vascular injury was evaluated and analyzed by the intraoperative images of a consecutive series of patients undergoing LC.
Material and methods
Ethical approval
Researchers obtained approval from the ethics board of this hospital (YX2021-144). The study was registered in the Clinical-trials.gov database with this identification number: NCT05002426.
Setting and participants
A consecutive series of patients undergoing elective LC between January 2021 and August 2021 at this hospital was collected. Informed consent was signed by all study participants. These patients were operated on by one surgeon (LW) and all used the hilar plane as a guide in surgical procedures. Landmarks were confirmed and recorded by LW and HL during the operation, then further confirmed and analyzed by LW and HH after the operation. All of them are professional hepatobiliary surgeons. Ultrasonography was the mainstay for the preoperative diagnosis of gallstone disease.
Eligibility criteria
Patients with severe atrophic cirrhosis of the liver were excluded from the statistics to avoid anatomic changes of the first porta hepatis. Patients with unexpected gallbladder carcinoma were also excluded.
Surgical technique
During the operation, the base of segment 4 and the start line should be placed in the horizontal position under the laparoscope. The gallbladder was pulled to the head side, then a separating forceps or an electric coagulation hook was used to slide along the peritoneum, down horizontally from the base of segment 4. It formed a “neck-shoulder” structure when the hilar plane met the tent-like Calot’s triangle. The peritoneum of Calot’s triangle was dissected on the neck area, then the peritoneum of posterior triangle of the gallbladder was also cut at the same extension level (Photos 1 A, 2 C).
Photo 2
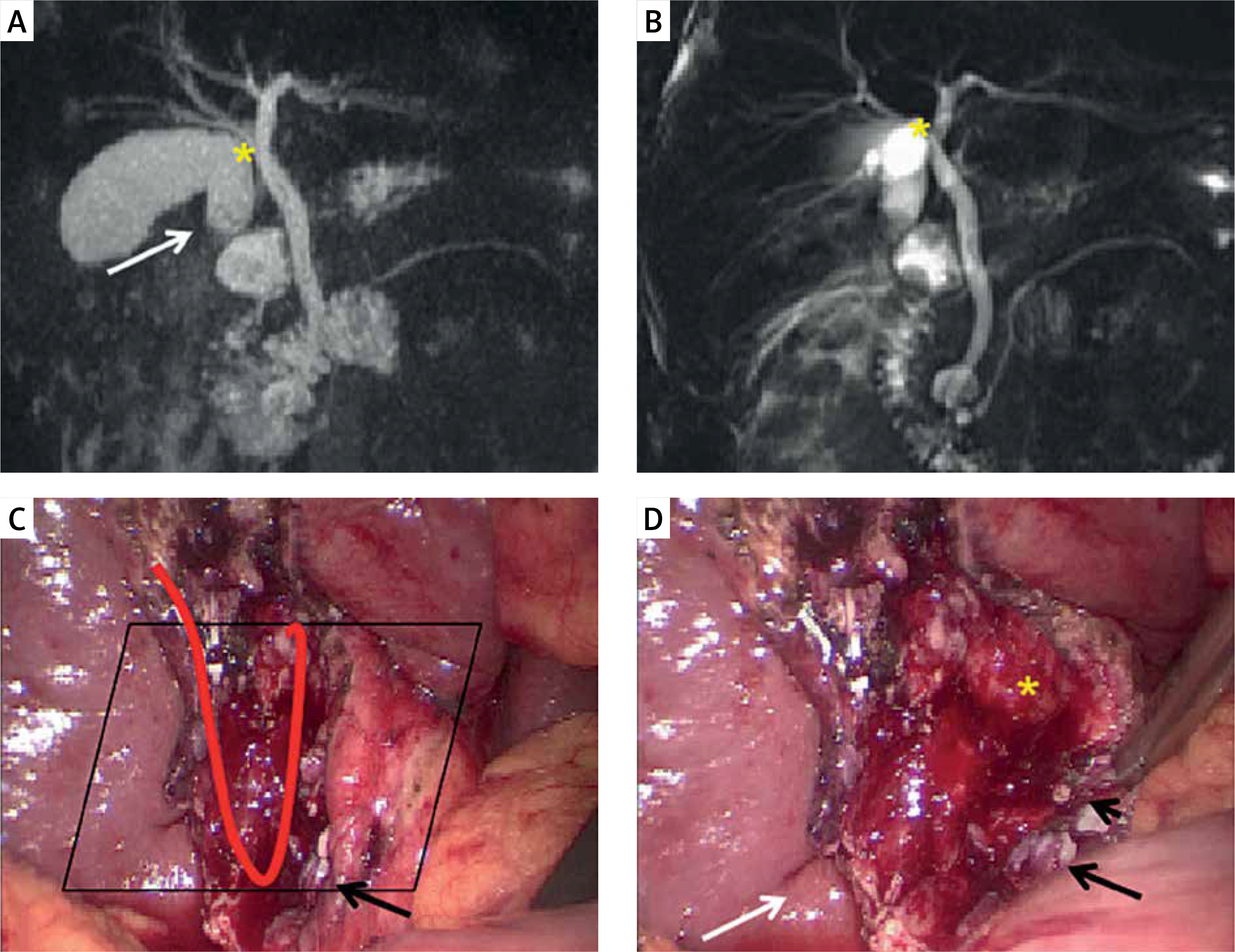
Exposing the ss-i layer at the ventral border of the hilar plane. A case of tissues overlapping caused by calculus incarcerated cholecystitis, the peritoneal under the hilar plane was preserved. The yellow asterisk shows the folded gallbladder body overlapping with the right hepatic duct; the black parallelogram shows the hilar plane and the red arc shows the trajectory of the peritoneum incision. The long black arrow shows the cystic duct, which is of low confluence to the CBD. The white arrow shows RS; its tip is not pointing at the cystic duct but at the neck of the gallbladder
The peritoneum of the posterior gallbladder triangle which is above the start line can be opened close to the gallbladder bed. Then, the bottom 1/3-1/2 of the peritoneum of the cystic plate which is above the start line was required to be opened before further blunt dissection (Photo 1 A). This was done to enlarge the operative space and facilitate the exposure of possible bile duct and artery variations, and facilitate the establishment of a “critical view of safety” [12].
Note that sharp dissection and electrocoagulation could be performed on the ventral side of the hilar plane, but should be avoided on the dorsal side of the plane and under the start line. After the peritoneum of the anterior and posterior triangle of the gallbladder was opened, the “critical view of safety” was used for gaining a sufficient view of Calot’s triangle before transecting the cystic duct. For those cases with highly inflamed gallbladders, the inner layer of the subserosal layer (the ss-i layer) dissection technique [13, 14] was used for dissecting the triangle (Photo 1 A).
Reverse protection theory is used in this dissection process, which means identifying the organizations that we need to protect rather than identifying what we need to remove. What we need to protect include the common hepatic duct, common bile duct, possible presence of the ectopic right hepatic duct, and the right hepatic artery.
Type and orientation of RS were recorded
In this study, the most frequently used classification method was used [15], which included open type, fused type, and absent type. RS was present if a fissure or hole was seen in the liver parenchyma on the right side of the gallbladder, and its tip was pointing to the hilum hepatis or extending from the arc incisure of the right posterior hepatic pedicle [11], whether or not the main or branches of the right posterior hepatic pedicle was visible in the fissure. The key step was to expose the posterior triangle of the gallbladder by retracting the ampulla of gallbladder to the left, or exposing the right and posterior of the hepatoduodenal ligament. However, in severely difficult cases, if the bowel or omentum had tightly adhered to the posterior triangle of the gallbladder, full exposure of RS was not required to avoid the occurrence of intestinal injury.
Comparison between the hilar plane and the RS plane
According to the definition of the RS plane, it is an imaginary line drawn along the RS roof and pointing to the base of segment 4 and forms a “security dissection triangle”. Similarly, the “start line” of the hilar plane also forms a triangle in the posterior triangle of the gallbladder. The areas of these triangles were compared and it was noted whether the ectopic right posterior bile duct existed and which planes had better protection effects.
Results
Clinical findings
A total of 155 consecutive patients were included in the study. The final sample consisted of 58 male and 97 female patients, with a mean age of 47.72 ±14.16 years (range: 13–88 years). Laparoscopic operations were successful in all cases, including complex cases, no cases were transferred to open surgery, and no cases of bile duct and vascular injury were reported. There were 36 severely difficult cases, including acute suppurative cholecystitis, gallbladder gangrene, and Mirizzi’s syndrome (2 cases). The hilar plane presented constant anatomy. All patients were able to successfully reveal the base of segment 4 and construct the hilar planes, although there were 7 patients with mild adhesion in front of the hilar planes and requiring slight dissection. Twelve cases of caterpillar right hepatic artery and 2 cases of atopic right posterior hepatic bile duct (aPHD), which lay just beneath the hilar plane (Photo 3), were found.
Photo 3
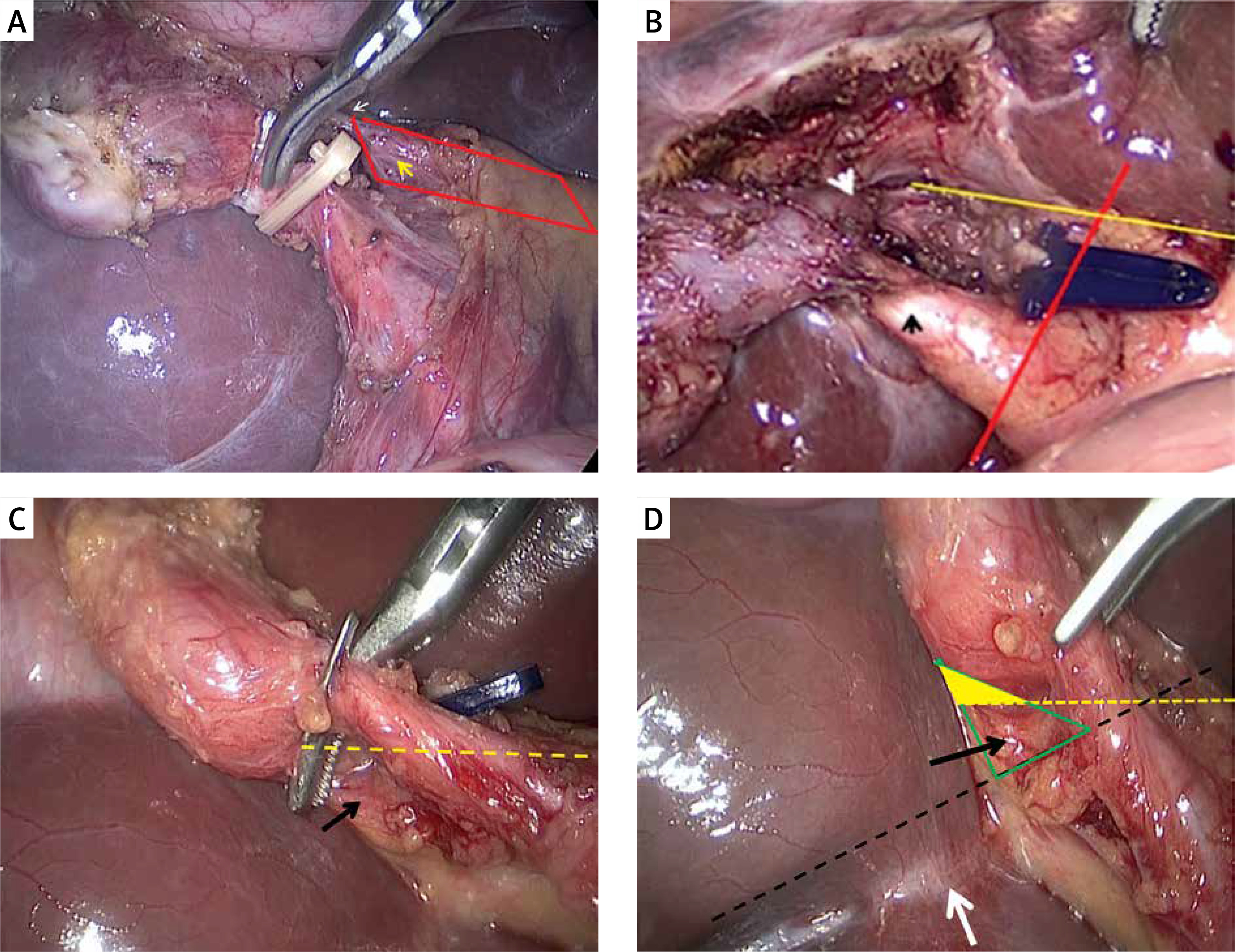
A – The yellow arrow marks the “caterpillar hump” like right hepatic artery which is on the dorsal side of the hilar plane (red frame), while the white arrow denotes the cystic artery. Blindly clamped on the dorsal side of hilar plane, it is dangerous and might injure the right hepatic artery. B – BDI can be avoided by referring to the hilar plane in a case of type V aPHD (Classification of the confluence types of the aPHD by Hisatsugu [31]). The yellow line marks the hilar plane, the red line indicates the RS plane, the white arrow denotes the aPHD, and the black arrow shows the cystic duct. C, D – In another case, the hilar plane shows a better protective effect than the RS plane. The aPHD was in the green triangle area but not in the yellow triangle area. The green area shows the “security dissection triangle” formed by the RS roof (dotted black line) of the RS plane, and the yellow area shows the triangle area formed by the start line (dotted yellow line) of the hilar plane. The black arrow shows an ectopic hepatic duct joining the cystic duct. Red arrows show the cystic duct, and the white arrow shows a fused type RS
Type and orientation of RS
Rouviere’s sulci failed to be identified clearly in 9 cases due to severe adhesion around the right posterior hepatic pedicle. The open type RS which met the above definition was present in 72% (105/146) of the patients, while fused type and absent type accounted for 11.6% (17/146) and 16.4% (24/146) (Photos 4, 5). Some cases were hard to categorize (Photos 4 F–I, 5 D–F). In 74.3% (78/105) of open type cases, Rouviere’s sulci presented a larger angle like an opened mouth and the hepatic pedicle could be seen directly or by spreading the upper and lower lips; while in 25.7% (27/105) of open type cases, Rouviere’s sulci presented a smaller angle like a closed mouth with thick upper and lower lips making the hepatic pedicles difficult to see clearly.
Photo 4
Open type of RS. A, B – The hepatic pedicle can be seen directly or by separating the upper and lower lips (like an open mouth). B – The distal part of RS has been partially fused (scar). C – Further fusion at the distal part, which is difficult to distinguish from the absent type without careful identification. D, E – Another common open type RS. It is difficult to see the hepatic pedicle, as RS has thick upper and lower lips (like a closed mouth). E, F – A further fusion of thick lips. G–I – With further thickening of upper and lower lips, the floor of the sulcus healed earlier than the opening (basal first fusion)
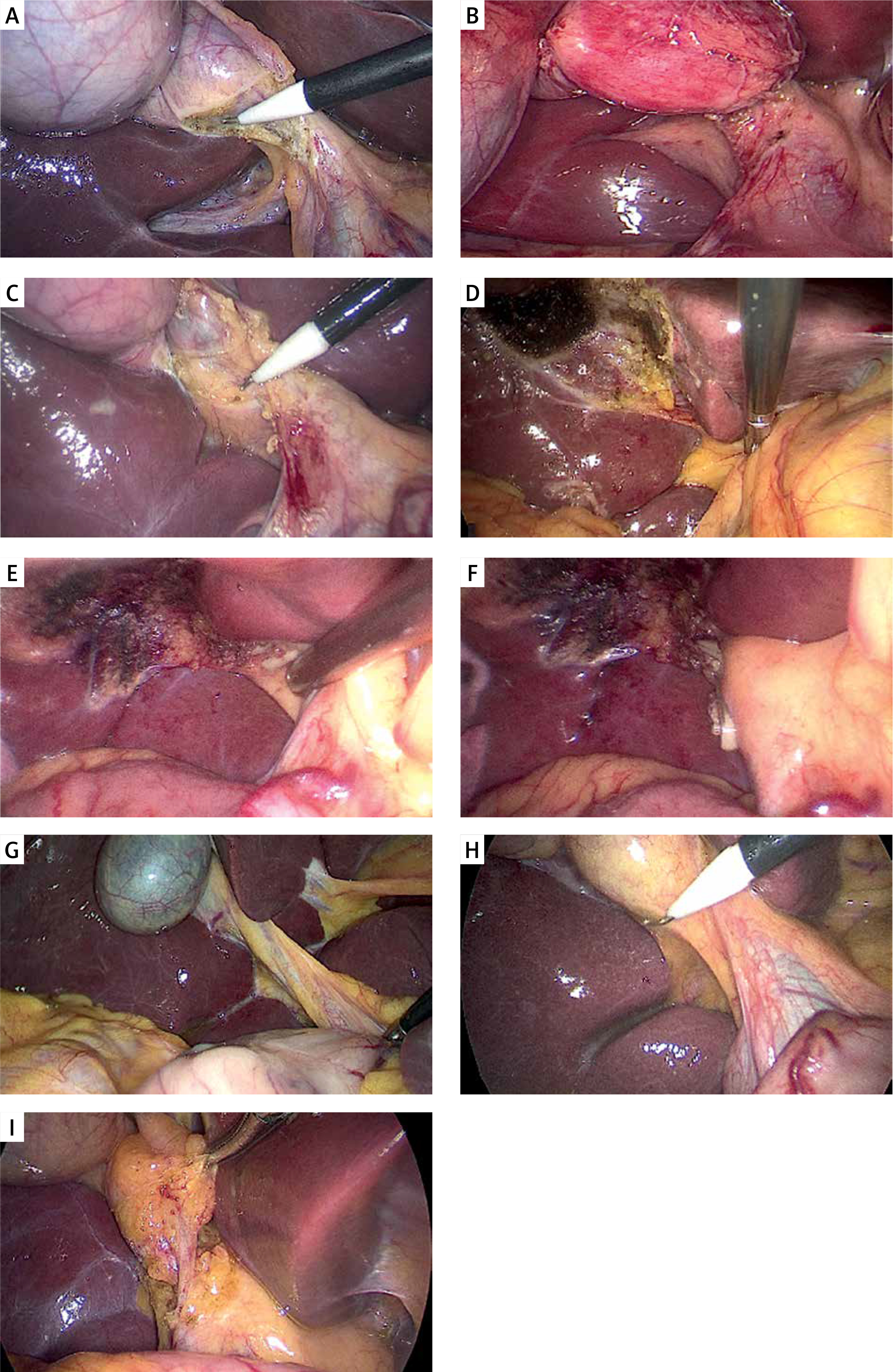
Photo 5
Fused type of RS. A–C – Three kinds of fused type of RS. A hole or slit extends from the arc incisure of the right posterior hepatic pedicle (white lines), far or near, regardless of whether the hepatic pedicle is visible in the RS. D, E – A very shallow notch or hole that is hard to categorize as the fused type but seems in line with the arc incisure of the right posterior hepatic pedicle. F – The presence of both proximal and distal fissures may make it difficult to classify it as an open type or a fused type
A kind of isolated fissure was found on the right side of the gallbladder bed and all obviously elevated above the start line; it looked like a fused type RS but did not meet the RS standard as its tip was not pointing to the hilum hepatis or extending from the right posterior hepatic pedicle. They were found in 14 patients. It was an accessory fissure but it could have led to operator misjudgment due to the fissure being near the gallbladder bed (Supplementary Photos S1).
For the orientation of RS, the vast majority of cases were oblique to the anterior, inferior, and external edge of the liver (oblique). However, unlike in autopsy specimens, the orientation of RS could be affected by the traction force on the gallbladder during surgery, from oblique to horizontal, or even from oblique inferior (oblique) to superior (vertical). In this group, 2 cases of open type RS were photographed with the orientation obviously oblique to the anterior and superior (vertical) (Table I).
Comparison between the hilar plane and the RS plane
Theoretically, the triangle formed by the hilar plane should be smaller than the “dissection triangle” formed by the RS plane, as the baselines of the two triangles were different: one is a horizontal line (start line) and from left to right; the other, however, in most cases is an oblique line and from right to left (RS roof) (Photos 1 C, 3 D).
The hilar planes and the RS planes formed a similar triangle in 73 cases of open type Rouviere’s sulci (all were open mouth) which had noticeable “upper lips” (RS roofs) and the vertex of the RS roofs on the start line. In them, 5 cases of RS roof with horizontal orientation formed the same triangle. In other cases, the start lines formed smaller dissection triangles than the RS roofs due to higher spatial positions. The hilar plane had a better protection effect for avoiding ectopic hepatic duct or ectopic right hepatic artery injury (Photos 3; Supplementary Photos S2).
Discussion
Many methods and strategies have been adopted to reduce the incidence of BDI [4, 7–9, 11, 16–21]. Intraoperative ultrasound, fluorescence cholangiography with indocyanine green (ICG), and intraoperative cholangiography (IOC) can help to identify the common bile duct and reduce the risk of BDI and all belong to the surgeon’s armamentarium [17–21]. The operational skill and the ability to judge the anatomical level are the most basic requisites for a qualified hepatobiliary surgeon.
The overlap of tissues seems to be an important cause of bile duct damage (Photos 2 A, B, D). The causes of this overlap include congenital (anatomical variation) and acquired (inflammatory adhesion). It is necessary to choose a safe plane to cut the peritoneum and separate the overlapping tissue bluntly below the plane.
RS is a hepatic fissure that runs to the right side of the hepatic hilum and usually contains the right portal triad or its branches [6, 7]. It is seen posterior to the fossa of the gallbladder and has been of interest to anatomists for several years considering its significance in gallbladder surgery. Hugh et al. first raised concerns about its importance in LC and further presented the concepts of the plane of RS, which was an imaginary line drawn between the sulcus and the base of segment 4 and formed a “security dissection triangle” bounded by the liver surface, the neck of the gallbladder, and the plane of the sulcus [5–7].
Some problems exist in RS and the plane of RS
It is believed that the hilar dissection may be safely initiated by division of the peritoneum immediately ventral to the RS sulcus [5–7]. Data from several studies indicated that the prevalence of RS was in the range 73–90.4% [10, 22, 23].
However, there are some flaws in these considerations regarding RS. Firstly, in addition to the existence of the absent type, RS would also be covered by extensive dense adhesion in complicated cases [9, 23]. RS failed to be identified clearly in 9 cases due to severe adhesion in this study. Secondly, the descriptions and the classifications of RS by naked eye were very variable and confusing in the literature. Initially, RS was divided into open type, fused type, and absent type. The open type of sulcus was defined as a cleft in which the sulcus was opening throughout its length. The fused type was defined as the sulcus with its proximal partial fusion [15, 22]. A cadaveric study from Dahmane et al. emphasized that the right hepatic pedicle or the branches of the right hepatic pedicle should be visible in the RS sulcus, no matter whether the RS was of the open type or the fused type [15]. However, Singh et al. found that the incidence rates of visible right hepatic pedicle structures in the floor of RS were only 9–75% in laparoscopy, then he expanded the classification of RS and divided it into deep sulcus – open or closed, slit and scar. For a small, superficial, and narrow sulcus, they described it as a slit; if the sulcus was seen only as a white scar near the porta hepatis, they described it as a scar [20].
Based on the research of cadaver specimens [15] and our previous CT image findings, the inner structure in the RS was mostly the right posterior hepatic pedicle or its branch (Supplementary Photos S3–5). We recommend our definition of RS, which is a fissure or a hole on the extending line of the arc incisure of the right posterior aspect of the hepatic pedicle, regardless of whether the main right hepatic pedicle or branches of the right hepatic pedicle are visible in the floor of the sulcus. This definition highlights that the RS should extend from the arc incisure of the right posterior hepatic pedicle, which can help to identify some small, superficial, or narrow RS when the right hepatic pedicle is invisible in the floor of the sulcus. In addition, it is common to find one or several cracks (accessory fissures) on the visceral facies of the right liver [23]. Srimani et al. reported the incidence of accessory fissures in the inferior surface of the right lobe as 27.3% [24]. If an accessory fissure is close to the gallbladder bed, it may lead to operator misjudgment (faked RS). So, our definition can also help surgeons distinguish fused type RS from “faked RS” during the operation.
In this series, the percentages of the three types were 72%, 11.6% and 16.4% respectively. We also included some atypical cases which had not been documented before. By comparing diversity in the types of Rouviere’s sulci with CT images and liver development [25–27], we believe that the RS is the result of the right portal triad incompletely enclosed by liver parenchyma during the embryonic stage of the liver. We propose that this process is similar to a peninsula (portal triad) being inundated by the rising tide (liver parenchyma). The fusions were irregular and created diverse types of Rouviere’s sulci. A similar phenomenon can also be seen in the umbilical fissure, where some umbilical fissures have liver bridge-like structures (Supplementary Photo S6). Based on this theory and according to fusion order, we propose to classify the RS into five types: distal first fusion type (Type I), middle first fusion type (Type II), proximal first fusion type (Type III), basal first fusion type (Type IV), and completely fusion type (Type V). Table II shows the differences between the three different classification methods.
Table II
Differences in three classifications
| Singh M (2017) | Dahamn R (2013) | Our proposal | |
|---|---|---|---|
| Deep sulcus | Open type | Open type(open mouth) | Distal first fusion |
| Close type | Open type(closed mouth) | Middle first fusion | |
| Scar | Open type | Distal first fusion | |
| Absent? | Absent? | Basal first fusion* | |
| Slit | Fused type | Proximal first fusion | |
| Absent | Absent | Completely fusion type | |
A cadaveric investigation found that the orientation of the RS roof is oblique to the anterior, inferior, and external edge of the liver (oblique) in 97% of the cadavers and horizontal in 3% of the cases [15]. But in laparoscopy, Singh and Prasad found that the direction of the sulcus in its various forms was mostly horizontal, sometimes oblique, and rarely vertical [22]. Kumar et al. found that it was oblique in 59.1% of cases, and transverse (horizontal) in 40.9% of cases [28]. In this group, we found that the direction of the sulcus was mostly oblique, rarely horizontal or vertical. It was probably due to the fact that the operation can be completed without excessively pulling the gallbladder to the cephalic side in most cases.
In the literature, the plane of RS was marked by a straight line extending from the upper edge of an open type sulcus (RS roof) and pointing to the base of segment 4 [3, 7]. For the most part, the schematic drawing corresponded with the actual needs, as in most cases, the type of RS is open, and the orientation is oblique. However, when the orientation of RS is vertical or the upper edge of RS is significantly lower than the base of segment 4, it should be a curved line rather than a straight line (as shown in Photo 1 D). Also, the orientation of RS could be affected by the traction force on the gallbladder during surgery. Therefore, the RS plane does not have constant anatomy, and different surgeons may have different judgments.
Advantages of the hilar plane
The base of segment 4 or the inferior surface of the quadrate lobe has received a lot of attention in previous studies. The 2018 Tokyo Guidelines proposed imaging of a connecting line between the base of segment 4 of the liver and the roof of RS during LC [3]. The “inferior boundary of dissection” [8] and the “R4U line” [9] were two landmarks somewhat similar to the hilar plane, but they both still needed to set a plane, which connects the hilar plate and RS or the RS roof. Fujioka et al. [29] used the “segment 4” approach for difficult laparoscopic cholecystectomy, which was a line connecting the right dorsal and left ventral corners of segment 4. However, the line of “segment 4” may be variable due to the different shapes of the quadrate lobe [30].
In this study, the hilar plane alone can provide a safe anatomic plane in some cases when it is difficult to reveal or identify RS. The hilar plane is simpler, more intuitive, and needs less dissection than the RS plane. The common bile duct, right hepatic artery, and (if present) the ectopic right posterior hepatic duct all lie under the hilar plane (Photo 1 B). In this group, there were 12 cases of caterpillar right hepatic artery, all of which were located on the dorsal side of the hilar plane. We did not find any ectopic right hepatic artery running on the ventral side of the hilar plane in our previous surgical data.
In most cases, the hilar plane forms a smaller dissection triangle than the RS plane due to a higher spatial position of the “start line” than the RS roof. Kurata et al. [31] found that about 6.8% of the patients presented an atopic posterior hepatic duct (aPHD), and 0.8% of the aPHD was released from the cystic duct. In this group, there were 2 cases of patients who had aPHD in the ‘dissection triangle’ marked by the RS plane rather than the hilar plane. Our previous studies found more cases with aPHD, and no aPHD injury occurred by referring to the hilar plane rather than the RS plane. Also, when the CBD is loosened or improperly released in advance (such as severe adhesion or when there is a history of surgery in the upper abdomen), the CBD may be pulled on the ventral side of the RS plane. At this time, it is not safe to rely solely on the RS plane as a reference (Supplementary Photo S7).
Limitations: Neither the hilar plane nor the RS plane can prevent a rare kind of atopic bile duct (Luschka duct) injury because it always lies above the start line. It is believed that precise surgical procedures and diagnosis of bile leakage on the gallbladder bed during the operation were effective in preventing bile leakage after the operation [32].
Conclusions
Essentially, RS is a special accessory fissure, which contributes to its diversity. We recommend our definition and classification method of RS based on the fusion concept. The hilar plane has the features of constant location, large coverage area, and higher location, thus being further away from the critical structures. We regard all landmark-based approaches as complementary. If possible, multiple landmarks should be used intraoperatively for preventing bile duct injury that we cannot afford.