








Introduction
Surgical resection is the most important stage of treatment in gastric cancer, which is the fourth leading cause of cancer-related death [1, 2]. Postoperative morbidity in gastric cancer surgery, which is high-risk surgery, varies between 9% and 46% and mortality varies between 0 and 16% [3, 4]. Although operative techniques and surgical stapling devices have recently been improved, anastomotic leaks remain a major problem for surgeons [5, 6]. Late diagnoses of anastomotic leaks can lead to increases in mortality and morbidity, such as local recurrence, sepsis, prolonged stay in the hospital, and increased costs [7, 8]. Early diagnosis and intervention have crucial roles in reducing mortality and morbidity rates. There is currently no “best” diagnostic method that can diagnose anastomotic leaks early, and the neurologic state of the patient, fever, abdominal distention, and abdominal hypersensitivity in the postoperative period can cause misdiagnoses [9, 10]. In addition to the surgical techniques developed to reduce postoperative morbidity and mortality, Bardram et al. defined the Enhanced Recovery After Surgery (ERAS) multidisciplinary protocol in 1995, which aimed to reduce the surgical stress response and reduce the occurrence of complications [11]. The relationship between inflammatory markers and the ERAS protocol in the detection of major complications in patients with gastric cancer is not fully defined today. It is necessary to reveal the relationship between the inflammatory process and the ERAS protocol, including tumor necrosis factor-α (TNF-α), in order to better inform clinicians [12].
Aim
In this prospective study, we aimed to understand the role of inflammatory substances in the detection of postoperative major complications after gastric cancer operations performed under the ERAS protocol.
Material and methods
The study took place in Clinics of General Surgery. Records of patients who underwent elective laparoscopic total/subtotal gastrectomy with the ERAS protocol for gastric cancer between January 2018 and December 2019 were evaluated prospectively. 120 consecutive patients who were treated surgically for gastric cancer in accordance with the ERAS protocol between January 2018 and December 2019 were included in this prospective study. Venous blood samples were taken at the 3rd and 5th post-operative day (POD) and blood values of interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α), C-reactive protein (CRP), procalcitonin (PCT) and white blood cell (WBC) were evaluated from these serum samples stored at –80°C after centrifugation for diagnosing major complications.
Patients older than 18 years of age and whose written informed consent for laparoscopic gastric cancer surgery was obtained within the ERAS program were included in the study. In addition to patients who did not meet the inclusion criteria, patients who received hemodialysis treatment due to chronic renal failure, those with esophagogastric junction or pyloric level obstruction, and those with psychiatric problems that could not comply with the ERAS program were excluded from the study.
After resection and lymph node dissection in accordance with the standard technique, the anastomosis stage was started. In patients who underwent subtotal gastrectomy with laparoscopic method, the defect formed after creating the common lumen with a endoscopic linear stapler was closed with absorbable and non-absorbable double-layer sutures and anastomosis was completed as Billroth II gastrojejunostomy. In total gastrectomy operations, the Roux-en-Y esophagojejunostomy method was used for anastomoses. Jejunojejunostomy anastomoses were performed in the same way as described for gastrojejunostomy anastomoses above. For esophagojejunostomy anastomoses the Orvil and 25 mm circular stapler were used. The circular stapler body was placed into the abdominal space by widening the trocar site in the left upper quadrant, and the esophagojejunostomy anastomosis was completed in this way. After general control hemostatic fascial defects larger than 10 mm that occurred secondary to trocar insertion were closed in an appropriate way. Thus, operations were completed.
Enhanced Recovery After Surgery protocol
By informing patients about the operation with a comprehensive and multidisciplinary approach, patients were persuaded to stop smoking and consuming alcohol before the operation. In the preoperative period, enteral nutritional support for 10 days and prophylactic 6000 IU enoxaparin sodium (subcutaneous) 1 × 1 were administered. Three hours before the operation, those without diabetes were given 300 ml of clear liquid rich in carbohydrates. The patients were evaluated by the anesthesia team experienced in the ERAS protocol and were applied epidural and general anesthesia by the same anesthesiologists. Epidural analgesia was administered with 10 ml of 0.25% bupivacaine. Analgesia was provided from the epidural catheter until the end of the postoperative 2nd day, and the epidural catheter was removed on the 3rd day. A nasogastric tube was not used. Body temperature was maintained intraoperatively with warm air support. Perioperative hourly urine outputs were monitored. A urinary catheter was removed in patients with urine output above 30 ml/h after the operation. No intraabdominal drain was placed. At the postoperative 6th hour, the patients were mobilized and shown respiratory exercises by the same team. Oral intake was started at the postoperative 10th hour initially limited to 1 l of water and 300 ml of pulp-free fruit juice for the first 24 h. Oral fluid intake was continually increased until the postoperative 3rd day and 20–40 ml/h of parenteral fluid support was given according to oral fluid intake. In addition to adequate fluid therapy, dexketoprofen 50 mg (IV) 3 × 1 for pain control, 50 mg (IV) of ranitidine hydrochloride 1 × 1, and prophylactic 6000 IU of enoxaparin sodium (subcutaneous) 1 × 1 were administered in patients with subtotal gastrectomy. From the third postoperative day on, the patient’s oral feeding was managed with semi-solid food and 1 l of water, continued medical treatment, and parenteral fluid support until discharge. Patients who did not need intravenous or oral analgesic-anti-inflammatory drugs, had a Visual Analogue Scale (VAS) score < 4, had sufficient skills for mobilization and self-care, took more than 2/3 of the oral food given, and had normal physical examination and laboratory test results were discharged with enteral nutrition support, vitamin prophylaxis and prophylactic enoxaparin sodium 6000 IU 1 × 1 (subcutaneous) per day.
Variables
The data of patients for age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) scores, comorbidities, habitual status for smoking and alcohol consumption of patients, type of the surgical procedures performed, duration of surgery, length of hospital stay, mortality, and complications that developed in the postoperative 30-day period were recorded. The main purpose was to detect major complications in the postoperative period. For this purpose, levels of CRP, PCT, TNF-α, IL-1β, and WBC from blood samples on postoperative 3rd (POD 3) and 5th days (POD 5) were measured. Units were determined as mg/l, ng/dl, pg/ml, pg/ml, 10–3/μl respectively. Pathological staging was done according to criteria listed in the AJCC Cancer Staging Manual 8th edition.
Definitions
Complications occurring within 30 days postoperatively were categorized according to the Clavien-Dindo classification [13]. Superficial surgical site infections, urinary tract infections, pneumonia, and postoperative ileus were designated as minor complications. Anastomosis leakage, intraabdominal hemorrhage, and intraabdominal abscess were designated as major complications. For daily follow-up posteroanterior chest X-ray (PA), ultrasonography (USG), and computed tomography (CT) were not used. These imaging methods were used in patients who were thought to have developed complications. Developing intraabdominal collections were drained by an interventional radiologist. Pneumonia was diagnosed by pulmonary infiltration on a chest CT scan or PA accompanied by clinical symptoms of lower respiratory tract infection, physical examination, or laboratory tests. Urinary tract infections were identified with a positive urine sediment test with leukocytosis and/or fever.
Anastomotic leak (AL) was defined by the presence of abnormal abdominal examination and extravasation of contrast in abdominal CT (with IV-oral contrast) or presence of air or fluid in the anastomosis area [14]. Bleeding was defined as postoperative hematemesis, melena or a sustained decrease in hemoglobin levels in postoperative blood samples. USG and abdominal CT were used to define intraabdominal hemorrhage. Ileus was defined as situations with nausea, vomiting, abdominal distention, abdominal tenderness or a temporary delay in gastrointestinal motility [15].
Ethical considerations
This study was approved by the local ethics committee (2020/188). All patients signed an informed consent form for the ERAS program and for inclusion in the study.
Statistical analysis
The NCSS (Number Cruncher Statistical System) 2007 (Kaysville, Utah, USA) program was used for statistical analysis. Descriptive statistical methods (mean, standard deviation, median, frequency, ratio, minimum, maximum) were used when evaluating the study data. The conformity of the quantitative data to normal distribution was tested by the Shapiro-Wilk test and graphical evaluations. The Mann-Whitney U test was used for two group comparisons of variables that did not show normal distribution. The Wilcoxon signed ranks test was used for intragroup comparisons of variables that did not show normal distribution. ROC analysis and diagnostic screening tests were used to determine the cut-off point according to the complications. Significance was evaluated at the p < 0.05 level.
Results
A total of 120 patients were included in the study. The study included 43 female and 77 male patients. Demographic data and ASA score, and comorbidities are shown in Table I. Subtotal gastrectomy were performed in 47 (39.1%) patients and 73 (60.8%) patients had undergone total gastrectomy. Surgical data and postoperative complications are shown in Table II. Major complications were observed in 12 (10%) patients. Anastomotic leak occurred in 6 (5%) patients. All of the anastomotic leaks that developed in total gastrectomy were in the esophagojejunostomy line. These leaks were managed by placing a covered stent and draining the intraabdominal collections percutaneously. The collections occurred after the leaks which were prepared for drainage were percutaneously drained. Appropriate antibiotic treatment was initiated for patients who underwent percutaneous drainage after a culture antibiogram. Intraabdominal hemorrhages were detected on POD 2 and POD 4 in 2 patients and needed surgical intervention. On POD 5, pneumonia developed in 2 patients. In the total gastrectomy group 2 patients with anastomotic leak and 1 patient with hemorrhage died. In the subtotal gastrectomy group 1 patient died because of anastomotic leak.
Table I
Patients’ characteristics and comorbidities
Table II
Surgical data and postoperative complications
A statistically significant difference was found between the groups in terms of the changes in CRP, PCT, TNF-α, and IL-1β measurements (p = 0.001; p < 0.01). The change in the group with major complications was greater than in the group without complications. There was no statistically significant difference between the groups in terms of changes in WBC measurements (p = 0.765; p > 0.05). In the group with major complications, the 3rd day (p = 0.001) and the 5th day (p = 0.001) CRP, PCT, TNF-α, IL-1β and WBC measurements were found to be statistically significantly higher than in the group without complications (p < 0.01). In the non-complicated group, the change in the 5th day measurements of CRP and WBC relative to the 3rd day measurements were not statistically significant (p = 0.790; p > 0.05) (p = 0.251; p > 0.05), but the reduction in PCT, TNF-α and IL-1β measurements was found to be statistically significant (p = 0.001; p < 0.01). In the group with major complications, the increases from day 3 to day 5 measurements of CRP, PCT, TNF-α, IL-1β were statistically significant (p = 0.004; p < 0.01) (p = 0.001; p < 0.01) (p = 0.001; p < 0.01) (p = 0.008; p < 0.01), but the changes in WBC measurements were not significant (p = 0.638; p > 0.05) (Table III). The measurements of CRP, PCT, TNF-α, IL-1β, and WBC on the 3rd day were statistically significantly higher in the group with complications (p < 0.01).
Table III
Evaluation of CRP, PCT, TNF-α, IL-1β and WBC results according to complication state
| Variable | Complication state | aP-value | ||
|---|---|---|---|---|
| Complication (–) (n = 108) | Complication (+) (n = 12) | |||
| Day 3 CRP | Min.–max. (median) | 55–997 (142.5) | 193–386 (277) | 0.001** |
| Mean ± SD | 151.66 ±94.14 | 275.79 ±50.38 | ||
| Day 5 CRP | Min.–max. (median) | 41–287 (141) | 233–453 (364.5) | 0.001** |
| Mean ± SD | 139.97 ±40.36 | 353.00 ±67.79 | ||
| bp | 0.790 | 0.004** | ||
| Difference (Day 5 – Day 3) | Min.–max. (median) | 854–113 (8.5) | 35–156 (86) | 0.001** |
| Mean ± SD | 11.69 ±98.03 | 77.21 ±65.79 | ||
| Day 3 PCT | Min.–max. (median) | 0.1–6.3 (1.5) | 7.3–17.4 (11.7) | 0.001** |
| Mean ± SD | 1.86 ±1.27 | 12.35 ±3.08 | ||
| Day 5 PCT | Min.–max. (median) | 0.1–8 (0.7) | 15.4–32.3 (23.5) | 0.001** |
| Mean ± SD | 1.15 ±1.14 | 24.08 ±5.11 | ||
| bp | 0.001** | 0.001** | ||
| Difference (Day 5 – Day 3) | Min.–max. (median) | 3.7–6.7 (–0.7) | 4.3–18.1 (11.8) | 0.001** |
| Mean ± SD | 0.70 ±1.25 | 11.73 ±4.85 | ||
| Day 3 TNF-α | Min.–max. (median) | 4.1–14.6 (6.3) | 10.1–37.7 (14.3) | 0.001** |
| Mean ± SD | 6.75 ±2.05 | 18.84 ±8.51 | ||
| Day 5 TNF-α | Min.–max. (median) | 1.6–22 (10.1) | 15–57 (32.3) | 0.001** |
| Mean ± SD | 11.15 ±4.10 | 34.27 ±10.98 | ||
| bp | 0.001** | 0.001** | ||
| Difference (Day 5 – Day 3) | Min.–max. (median) | 6.7–16.3 (4.5) | 2.5–43.3 (12.6) | 0.001** |
| Mean ± SD | 4.40 ±4.67 | 15.44 ±11.22 | ||
| Day 3 IL-1β | Min.–max. (median) | 1.2–19.6 (4.3) | 0.3–38 (23.4) | 0.001** |
| Mean ± SD | 5.00 ±2.84 | 22.02 ±10.19 | ||
| Day 5 IL-1β | Min.–max. (median) | 2.8–134.8 (7.7) | 13–64.6 (32) | 0.001** |
| Mean ± SD | 12.50 ±17.05 | 32.34 ±12.13 | ||
| bp | 0.001** | 0.008** | ||
| Difference (Day 5 – Day 3) | Min.–max. (median) | 3.5–126.5 (3.2) | 15.6–26.7 (10.9) | 0.001** |
| Mean ± SD | 7.51 ±16.54 | 10.32 ±9.51 | ||
| Day 3 WBC | Min.–max. (median) | 5.9–19 (10.7) | 9.2–22.8 (14.9) | 0.001** |
| Mean ± SD | 10.71 ±2.30 | 15.07 ±3.45 | ||
| Day 5 WBC | Min.–max. (median) | 6.5–16.2 (10.9) | 8–19.9 (15.3) | 0.001** |
| Mean ± SD | 10.98 ±1.76 | 14.50 ±3.54 | ||
| bp | 0.251 | 0.638 | ||
| Difference (Day 5 – Day 3) | Min.–max. (median) | 8–6.1 (0.8) | 9.4–4.9 (0.1) | 0.765 |
| Mean ± SD | 0.27 ±2.94 | 0.58 ±4.08 | ||
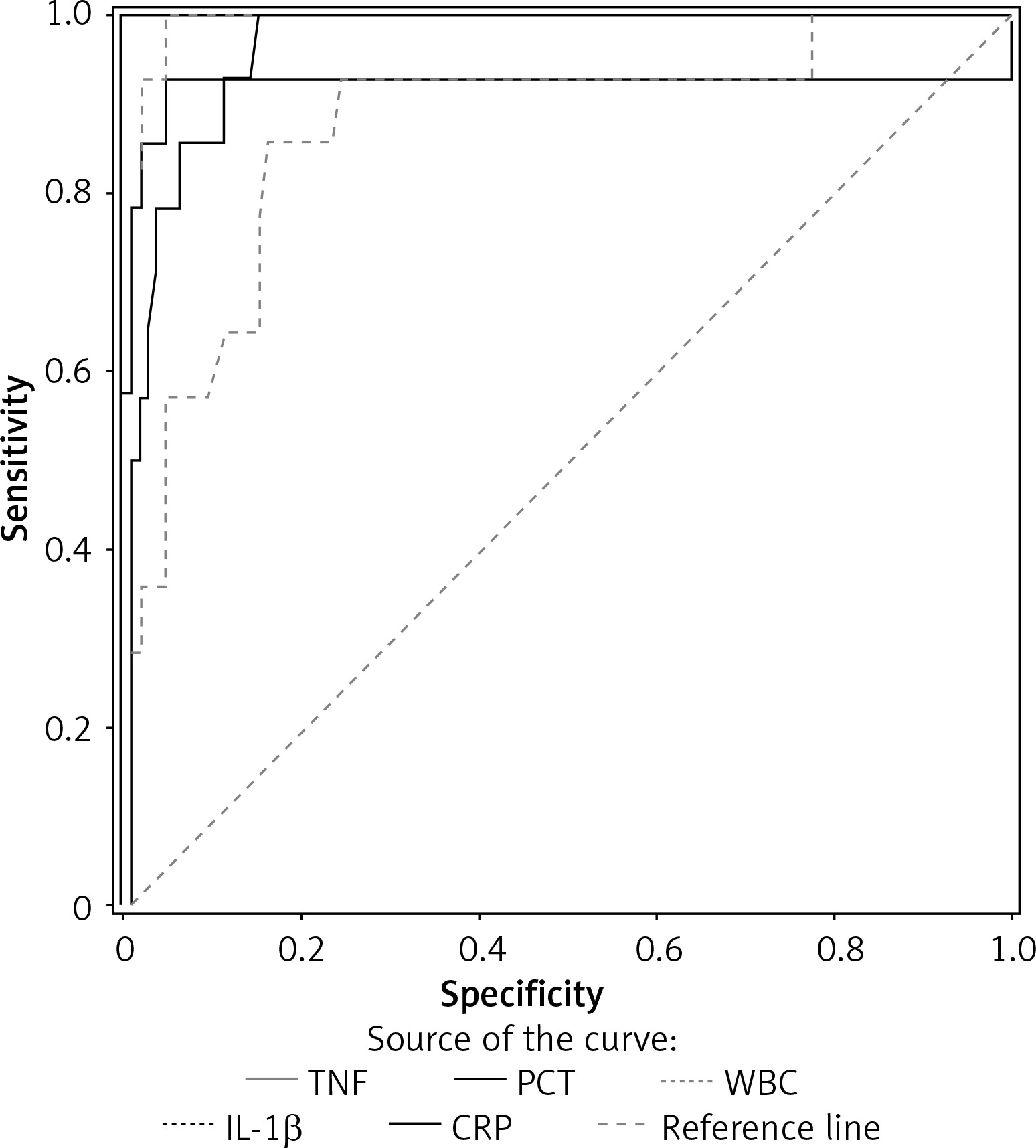
ROC analysis and diagnostic screening tests were used to determine the cut-off point according to the groups. A cut-off point was calculated for PCT, TNF-α, IL-1β, and WBC measurements. The cut-off point for the CRP measurements was determined as 193 and above, with a sensitivity of 100%, specificity of 84.91%, the positive predictive value of 46.67%, the negative predictive value of 100%, and the accuracy of 86.67%. The area under the ROC curve obtained was determined as 96.4%, standard error 1.7%. The cut-off point for PCT measurements was determined as 7.34 and above with a sensitivity of 100%, specificity of 100%, positive predictive value of 100%, negative predictive value of 100%, and accuracy of 100%. The area under the ROC curve obtained was determined as 100%, standard error 0%. The cut-off point for TNF-α measurements was determined as 10 and above with a sensitivity of 100%, specificity of 95.28%, positive predictive value of 73.68%, negative predictive value of 100%, and accuracy of 95.83%. The area under the ROC curve obtained was determined as 99.1%, standard error 0.7%. The cut-off point for IL-1β measurements was determined as 9.2 and above, with a sensitivity of 92.86%, specificity of 95.28%, positive predictive value of 72.22%, negative predictive value of 99.02%, and accuracy of 95.00%. The area under the ROC curve obtained was determined as 92.2%, standard error 6.9%. The cut-off point for WBC measurements was determined as 12.55 and above with a sensitivity of 85.71%, specificity of 83.96%, positive predictive value of 41.38%, negative predictive value of 97.80%, and accuracy of 84.17%. The area under the ROC curve obtained was determined as 87.4%, standard error 5.5% (Figures 1, 2, Table IV).
Table IV
Diagnostic scan tests and ROC curve results
| Parameter | Diagnostic Scan | ROC Curve | P-value | |||||
|---|---|---|---|---|---|---|---|---|
| Cut off | Sensitivity | Specificity | Positive predictive value | Negative predictive value | Area | 95% confidence interval | ||
| CRP [mg/l] | ≥ 193 | 100 | 84.91 | 46.67 | 100 | 0.964 | 0.931–0.997 | 0.001** |
| PCT [ng/dl] | ≥ 7.34 | 100 | 100 | 100 | 100 | 1.000 | 1.000–1.000 | 0.001** |
| TNF-α [pg/ml] | ≥ 10 | 100 | 95.28 | 73.68 | 100 | 0.991 | 0.978–1.000 | 0.001** |
| IL-1β [pg/ml] | ≥ 9.2 | 92.86 | 95.28 | 72.22 | 99.02 | 0.922 | 0.787–1.000 | 0.001** |
| WBC [10-3/μl] | ≥ 12.55 | 85.71 | 83.96 | 41.38 | 97.80 | 0.874 | 0.767–0.981 | 0.001** |
Discussion
The value and clinical results of ERAS protocols in colorectal and gastric cancer surgery have been accepted gradually [16–19]. As a result of optimized multimodal strategies, there is a common consensus that the ERAS protocol results in significantly accelerated intestinal functions, unaffected mortality rates, anastomotic leaks, surgical site infection, urinary tract infection, and lung infection; hence medical costs are reduced due to accelerated recovery and reduced surgical stress [20]. The ERAS protocol, which is reported to make a significant contribution to improving nutritional status in the postoperative period, but is also reported to cause an increase in the rate of re-hospitalization, should be evaluated with high-quality, large-sampled, long-term multi-center studies [21].
In recent years, when laparoscopy has become widespread, the use of laparoscopy also for gastrectomy has become increasingly common. As a matter of fact, in the meta-analysis conducted by Zhang et al., it was concluded that the laparoscopic method is an effective alternative [22]. Laparoscopy is strongly recommended for distal gastric cancers in the ERAS guidelines. However, although some positive results were mentioned for total gastrectomy in the same guideline, the recommendation for use of laparoscopy was not strong [23]. However, laparoscopy is preferred for total gastrectomy operations in many centers that have highly experienced surgeons. In this context, studies related to the ERAS protocol in total gastrectomy operations are published [24].
The shortening of the length of stay has paved the way for further research on predicting complications and safe discharge. In this respect, the number of studies on which biomarker is appropriate to predict complications in patients undergoing the ERAS protocol is increasing [25]. One of the most frequently researched markers in such studies is undoubtedly CRP. As mentioned in the study conducted by Wierdak et al., research on CRP values is mostly based on values on postoperative 4th and 5th days. However, considering that the duration of hospitalization is shortened after the ERAS protocol, there is a need to evaluate the levels of this marker on earlier days [26].
CRP, which is secreted from the liver with a half-life of 19 h, is one of the most commonly used acute phase reactants in the diagnosis of complications after abdominal surgery [27, 28]. CRP has been shown to exhibit sensitivity and specificity of 70% to 80% 2 to 4 days after the operation [29]. In our study, the increase in CRP on the basis of postoperative days is more significant in the group with major complications than in the group without complications. The 5th day values are statistically significantly higher than the 3rd day values in the group with major complications. The sensitivity was 100% and the specificity was 84.6% for CRP values of 193 mg/dl and above in detecting major complications.
PCT, which is produced only in thyroid C cells and normally detected at extremely low levels in healthy individuals, is frequently used in the diagnosis of major complications such as anastomotic leak and development of an intraabdominal abscess in the postoperative period [30]. PCT is a polypeptide produced in thyroid C cells released in response to microbial toxins and proinflammatory mediators such as IL-1β, TNF-α, and IL-6 [31, 32]. The rate of increase of this inflammatory substance, which we evaluated to determine the postoperative major complications, was found to be higher on the 3rd and 5th days in the group with major complications. The 5th day values were statistically significantly higher than the 3rd day values. Sensitivity and specificity were 100% for PCT values of 7.34 ng/dl and above in detecting major complications.
IL-1β can be released by many cells including monocytes, B-cells, keratinocytes, mesangial cells, and endothelium, but is not used in practice for the diagnosis of major postoperative complications. IL-1 is demonstrated in laboratory animals to cause sepsis, fever, increase in the release of colony-stimulating factors (CSF), neutrophilia, loss of appetite, and tendency to sleep, and leads to the synthesis of acute-phase proteins [33, 34]. IL-1β is a proinflammatory cytokine that stimulates the human liver to produce acute-phase proteins such as CRP and fibrinogen [35]. It has been suggested that the inflammatory response may be higher in humans [36]. In our study, even in measurements performed without any genetic evaluation, the rate of increase in IL-1 measurements was found to be higher in the group with major complications on the 3rd and 5th days. Also, in the group with major complications, the 5th day values are statistically significantly higher than the 3rd day values. IL-1β measurements for detecting postoperative complication detection show a sensitivity of 92.86% and specificity of 95.28% for values of 9.2 pg/ml and above.
TNF-α, which is similar to IL-1β in terms of clinical application and is a chemotactic agent for monocytes and leukocytes, also has antibacterial-antiviral effects. IL-1, platelet activating factor (PAF), and interferons, which increase mortality in septic shock, show synergistic effects with TNF-α [37–43]. TNF-α measurements on the 3rd and 5th days for the major complication group, both due to these features and because it increased the release of PCT, were found to be statistically higher than in the non-complicated group, which we included in the scope of the evaluation. For the TNF-α values of 10 pg/ml and above in detecting major complications, sensitivity was 100% and specificity was 95.28%. One of the frequently used markers in the diagnosis of major complications after gastrointestinal system surgery is WBC. A study by Wysocki et al. on bariatric surgery patients showed that WBC can be used safely even in the early period to predict postoperative complications [38]. However, surprisingly, the change of WBC levels on the basis of postoperative days in our study was not found to be statistically significant. For the 12.55 cut-off value of WBC in detecting major complications, sensitivity was 85.71% and specificity was 83.96%.
Multimodal rehabilitation programs and laparoscopic surgery reduce the patient’s systemic inflammatory response to surgery [40–42]. Early detection of a major complication that may lead to a septic picture after gastric surgery gives important clues about whether to undertake further investigations and when to discharge the patient from the hospital. Early and accurate detection of major complications becomes even more important in relation to early discharge, which is a part of the ERAS protocol [44–49].
It has been determined that CRP and PCT are significant in the early detection of anastomotic leaks in colorectal surgery using the ERAS protocol [50–53]. Our results showed that this fact is valid for gastric cancer surgery performed in line with the ERAS protocol. It has been previously determined that IL-1β and TNF-α have synergistic effects on both each other and the release of CRP and PCT in the inflammatory process. Therefore, it was observed that IL-1β and TNF-α, which we included in the study, increased significantly during periods of major complications similar to CRP and PCT, and can be used in the early diagnosis of major complications. Postoperative day 3 and day 5 measurements of IL-1β, TNF-α, CRP, and PCT, which are significant in terms of safe patient follow-up and early discharge, are shown to be significant in the evaluation of gastric cancer patients managed in line with the ERAS protocol. Regardless of the presence of significant examination findings, patients whose IL-1β, TNF-α, CRP, and PCT values are high should be evaluated with additional imaging such as USG and CT (oral-IV contrast). The ERAS protocol should be conducted with a multidisciplinary approach and optimally trained healthcare personnel. It is important to have an experienced interventional radiology team in the diagnosis and treatment of major complications.
In the ERAS protocol we applied, our patient group had high ASA scores, more advanced gastric cancer patients based on the TNM classification, and the morbidity (10%) and mortality (3.3%) rates were acceptable. These findings showed that the ERAS protocol in gastric cancer surgery can be safely applied even in advanced gastric cancer with high ASA scores. In addition, it has been determined that the ERAS protocol can also be safely applied in daily surgical practice in patients who have been operated on for gastric cancer.
Including patients treated in a single center is a limitation of the study. Prospective data collection must be considered as an advantage of the study. In addition to comparing the levels of biomarkers for both groups, evaluating the change of the parameters between the 3rd and 5th days is a strong point of this study, because many studies have focused only blood levels of markers directly and not recorded changes of parameters.
Considering the success of monitoring inflammatory agents in determining major complications, it is thought that the teams performing this surgical procedure will be able to follow their patients safely in the postoperative period and detect a major complication that may occur at an early stage. Multi-center studies with more patient groups are needed to better evaluate our hypothesis.