Introduction
The tentorium cerebelli comprises dural appendages containing the transverse sinus that lie on the cerebellum and divide the intracranial space into supratentorial and infratentorial compartments [1,2]. The tent shape of tentorium cerebelli helps preserve brain anatomy by providing cerebellum protection against pressure caused by the brain’s gravity effect. In the absence of the support structure of the tentorium, sagging (herniation) occurs in the brain [1-3].
Tentorial defects have a spectrum that can be seen together with severe central nervous system malformations, such as Dandy-Walker, Arnold-Chiari, and Gorlin syndrome, or as isolated minor defects. Isolated tentorial hypoplasia (TH) is extremely rare [4-11].
The current study aims to determine the prevalence of TH, which comprises very few cases in the literature, and increase awareness.
Material and methods
The decision number and approval date for this IRBapproved study are 2021-11/7 and 11/11/2021, respectively. MRI images of 5163 patients who applied to the training and research hospital for various reasons between 1 September 2020, and 31 August 2021, who underwent brain MRI, were reviewed retrospectively. TH distribution rates were determined according to the gender of the patients, the side of the hypoplasia, and the reasons for applying to the clinic.
Exclusion criteria included intracranial mass lesion, intracranial haemorrhage, intracranial operation, intracranial stab wound and radiotherapy history, diagnosed congenital syndrome-malformation, and hydrocephalus.
Patients were examined in 1.5 Tesla (Signa Explorer, GE, Healthcare, USA) and 3 Tesla (Magnetom Skyra, Siemens, Healthcare, Germany) MR systems. The protocol included at least axial T1- and T2-weighted images (WI), sagittal T2-WI, and axial fluid-attenuated inversion recovery (FLAIR) images.
A radiology research assistant (H.İ.Ş; 3 years of experience) analysed all MRI scans. MRI images of patients with TH were re-evaluated and confirmed by an experienced radiologist (Ö.Ü; 20 years of neuroradiology experience).
Results
Brain MRI examinations of 5163 patients included in the study were reviewed. As a result of the exclusion criteria, 939 patients were excluded from the study because of hydrocephalus, history of RT, intracranial mass, intracranial operation, intracranial haemorrhage, and congenital anomaly. TH was observed in 94 of the 4224 patients who met the inclusion criteria. Accordingly, the prevalence of TH among patients screened over one year was calculated as 2.22%. Of these, 76.59% were female (n = 72) and 23.41% were male (n = 22).
The rates of presentation complaints of TH patients were 60.63% headache, 17.02% vertigo, 4.25% seizures, 3.19% tremor, 3.19% syncope, 7.44% forgetfulness, and 2.12% visual impairment. Five patients (11.76%) were admitted for metastasis investigation due to their primary malignancy; they did not have any complaints (Table 1).
Table 1
Rates of presentation of complaints of tentorial hypoplasia patients
According to the localization of TH, 18.08% (n = 17) were observed on the right side (Figure 1), 28.72% (n = 27) on the left side (Figure 2), and 53.19% (n = 50) on the bilateral tentorium leaf (Figure 3) (Table 2).
Figure 1
A 52-year-old female patient who applied with the complaint of vertigo. A) Axial T2-WI shows herniation of the medial occipitotemporal gyrus into the quadrigeminal cistern (arrow) because of right-sided tentorium cerebelli hypoplasia. B) On coronal T2-WI, the continuity of the tentorium is observed as a hypointense line on the left, while the interruption of this hypointense line is clearly seen on the right (arrows). The arrowhead shows gyrus herniation into the quadrigeminal cistern. C) On sagittal T2-WI, the gyrus, which is herniated into the quadrigeminal cistern (arrow), is clearly observed
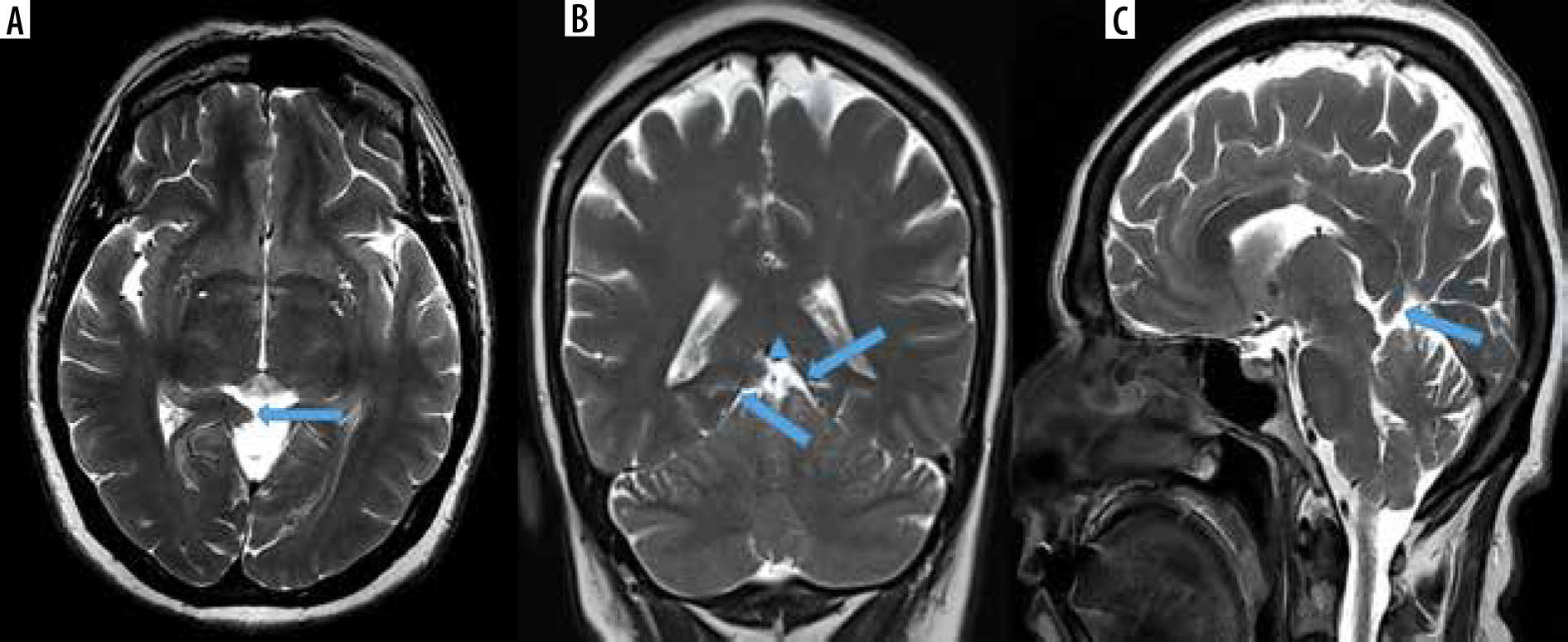
Figure 2
Magnetic resonance images of a 22-year-old male patient who presented with headache and seizure. A) Axial T2-WI shows herniation of gyrus to the quadrigeminal cistern (arrow) as a result of left sided tentorium cerebelli hypoplasia. B) On coronal T2-WI, the continuity of the tentorium on the right is observed as a hypointense line (arrow) and there is no sign of herniation. On the left, it is clearly seen that this hypointense line (arrow) has been interrupted. The arrowhead shows gyrus herniating into the quadrigeminal cistern. C) On sagittal T2-WI, the gyrus, which is herniated into the quadrigeminal cistern (arrow), is observed
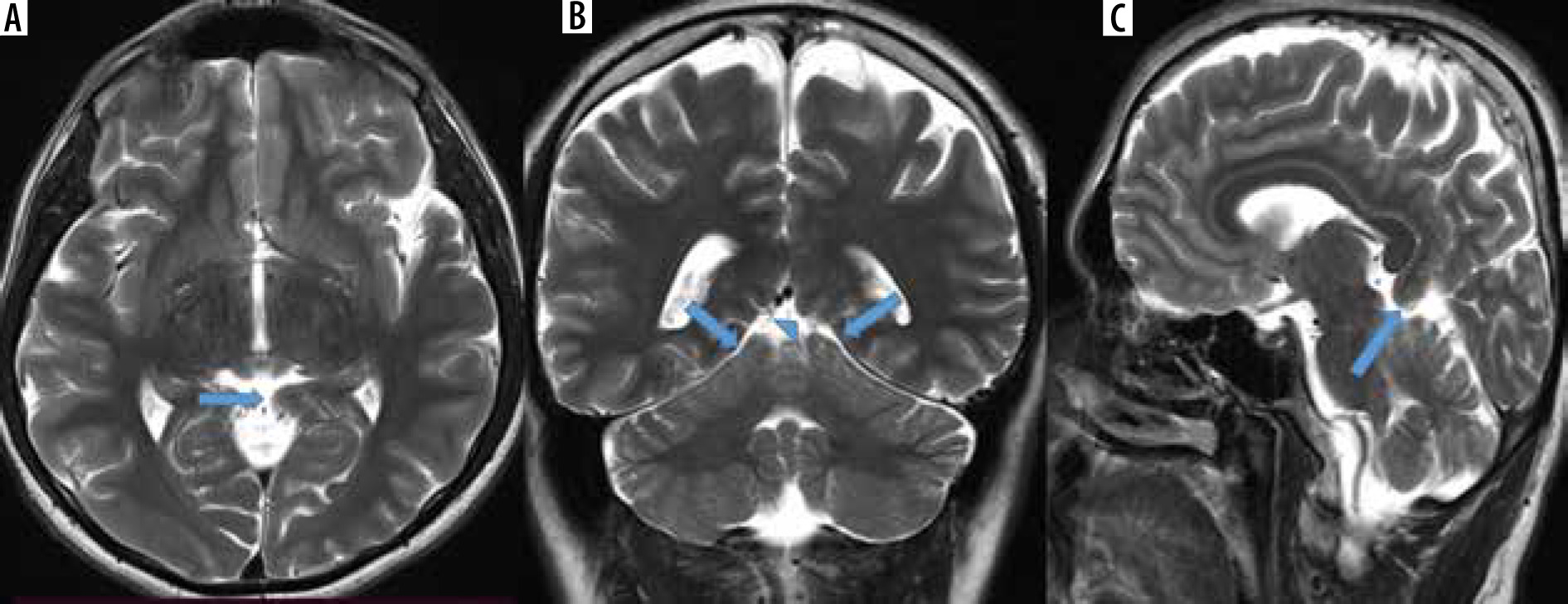
Figure 3
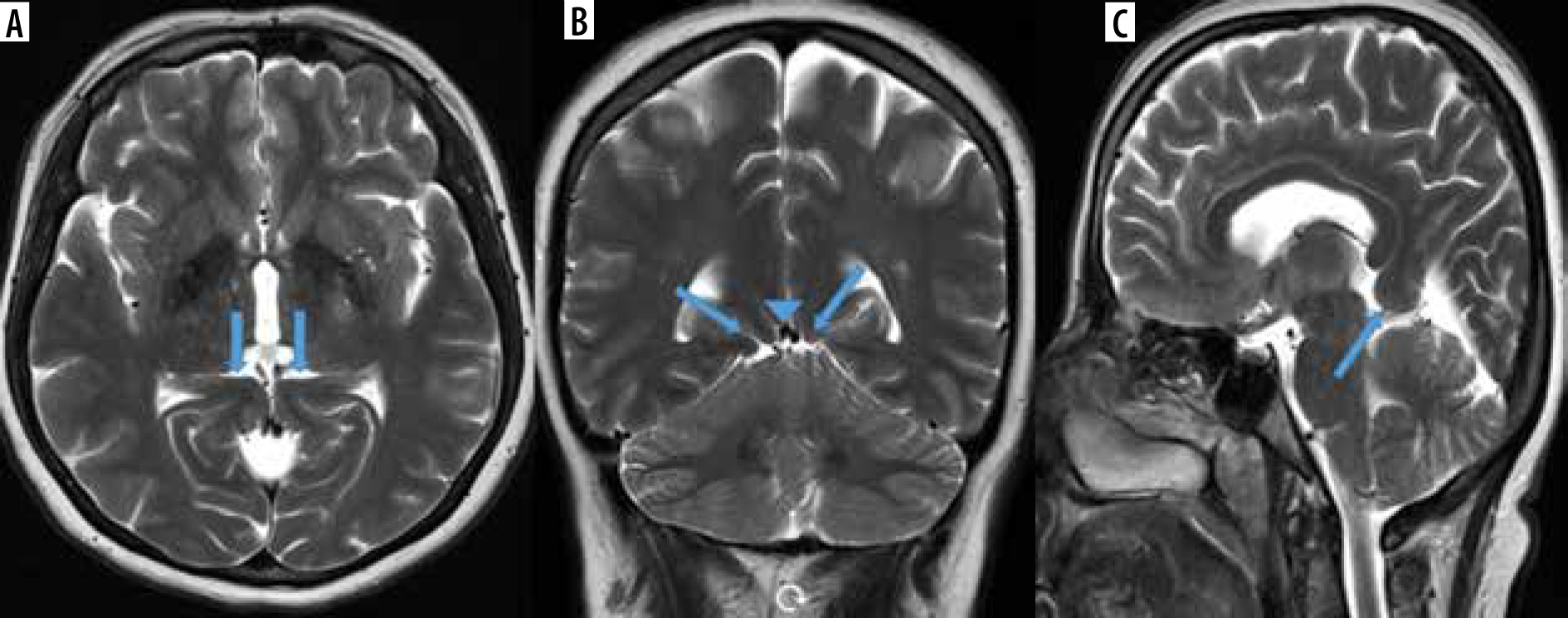
Magnetic resonance images of a 52-year-old female patient with a headache. A) Axial T2-WI shows bilateral gyri herniation into the quadrigeminal cistern (arrows) due to hypoplasia in both leaves of the tentorium cerebelli. B) Herniations of the gyri to the quadrigeminal cistern (arrows) and partial compression effect on the internal cerebral veins (arrowhead) are remarkable on coronal T2-WI. C) The size of the herniation is seen more clearly on sagittal T2-WI
Discussion
TH is an entity that can be seen isolated or together with some malformations and there is insufficient information about it. The cause of TH is not known exactly. Although various factors such as perinatal events and birth trauma have been suggested, the most accepted hypothesis is the abnormal fusion of the tentorium when it develops from the notochord. The first case of isolated TH was reported by Gund in 1985 in an 8-year-old girl who was evaluated for an occipital mass [6]. Few cases have been reported in the literature since this study [4,5,7-10]. Although its clinical significance is not fully known, cases with this anomaly have been reported in the literature to present with various symptoms such as headache, vertigo, syncope, and precocious puberty. Clinical symptoms may occur in varying degrees depending on the amount and localization of the defect [4-11]. In the articles we selected as a result of the literature review, we saw that the most common complaint of the patients was a headache, and our results were similar to the literature. In addition, while “seizure” was not previously mentioned as a complaint in the literature, we found that the complaint of 4 patients (4.25%) in our study was seizure. Visual impairment is one of the serious symptoms rarely reported in the literature and proven by diffusion tensor imaging [8].
In the articles we selected from the literature review, it was seen that the majority of the cases were female. Similarly, in our current study, 76.84% of the cases were female. These articles were examined, and it was noted that TH tended to be seen on the right side [4-11]. However, unlike in the literature, we found that TH was more likely to be seen in both tentorium leaves (53.19%) in the results we obtained.
This current literature review has insufficient and unclear evidence about TH rates. In the literature it was stated that the variations of tentorium are investigated and that these variations are associated with herniations and injuries [12,13]. In a study by Adler et al., a classification system was developed by examining 100 cadavers and making morphometric analysis of the tentorial aperture. Based on these analyses, MR images of 10 patients were used for tentorium evaluation. They determined some anatomical landmarks that can be easily seen on MRI and made 4 different measurements, and reported that these measurements can help characterize the neuroanatomical variations in this region [12]. In another study by Bisaria conducted on cadavers, it was reported that 16 of 90 patients had various developmental anomalies and variations in the tentorium, like tentorial dural bands, holes, and transverse ridges [14]. However, in these 2 studies, as in other studies, no information was given about the prevalence of TH. In addition, in the articles we retrieved as a result of the literature review, we did not find a classification related to the width of TH or the size hernia developing secondary to TH. We did not make any classification because the main aim in this study was to determine the prevalence of TH.
Tentorium is observed as hypointense linear structures on T1- and T2-weighted MR images. In a study in which the automatic segmentation method of the falx cerebri and tentorium was examined, it was mentioned that the tentorium was seen more prominently on T1-weighted images with contrast [15]. According to our experience, we think that T2-weighted images are the most useful sequences in evaluating TH cases that are large enough to cause a hernia, due to the contrast difference between CSF and tentorium.
The current study is the most comprehensive and the only retrospective study on this subject, to the best of our knowledge. We calculated the prevalence of TH as 2.22%. This ratio showed that TH was not well known enough and it was seen more frequently than previously thought.
The most important limitation of this study is the patient population because it was a single-centre study.
Conclusions
In this study, the prevalence of TH was determined by scanning brain MRI examinations in one year retrospectively, and it was determined as 2.22%. Being aware of TH during brain MRI evaluation will also prevent possible misdiagnoses. We hope that this study with a large number of patients will increase awareness about TH, because there are no studies other than cadaver studies and a few case reports.