








Introduction
Central lymph node metastasis sometimes occurs in papillary thyroid microcarcinoma (PTMC) in young and middle-aged women [1–4]. These patients are often concerned about the cosmetic appearance of the surgical scar, and this concern has led to increased interest in transoral vestibular endoscopic thyroidectomy (TOET) among clinicians and patients [5–7]. TOET offers a magnified operative field, higher resolution vision, and clearer exposure of the operation site when compared to traditional open surgery, but identification of lymph nodes and parathyroid glands (PGs) is still difficult [8–10]. Carbon nanoparticles (CNs) are novel lymph node tracers that have been widely used in open thyroid surgery [11, 12]. The goal of this study was to retrospectively evaluate the use of CNs in TOET in patients with unilateral PTMC.
Aim
To evaluate the efficacy of CNs for identifying lymph nodes (LNs) and preserving parathyroid glands in TOET with central neck dissection (CND).
Material and methods
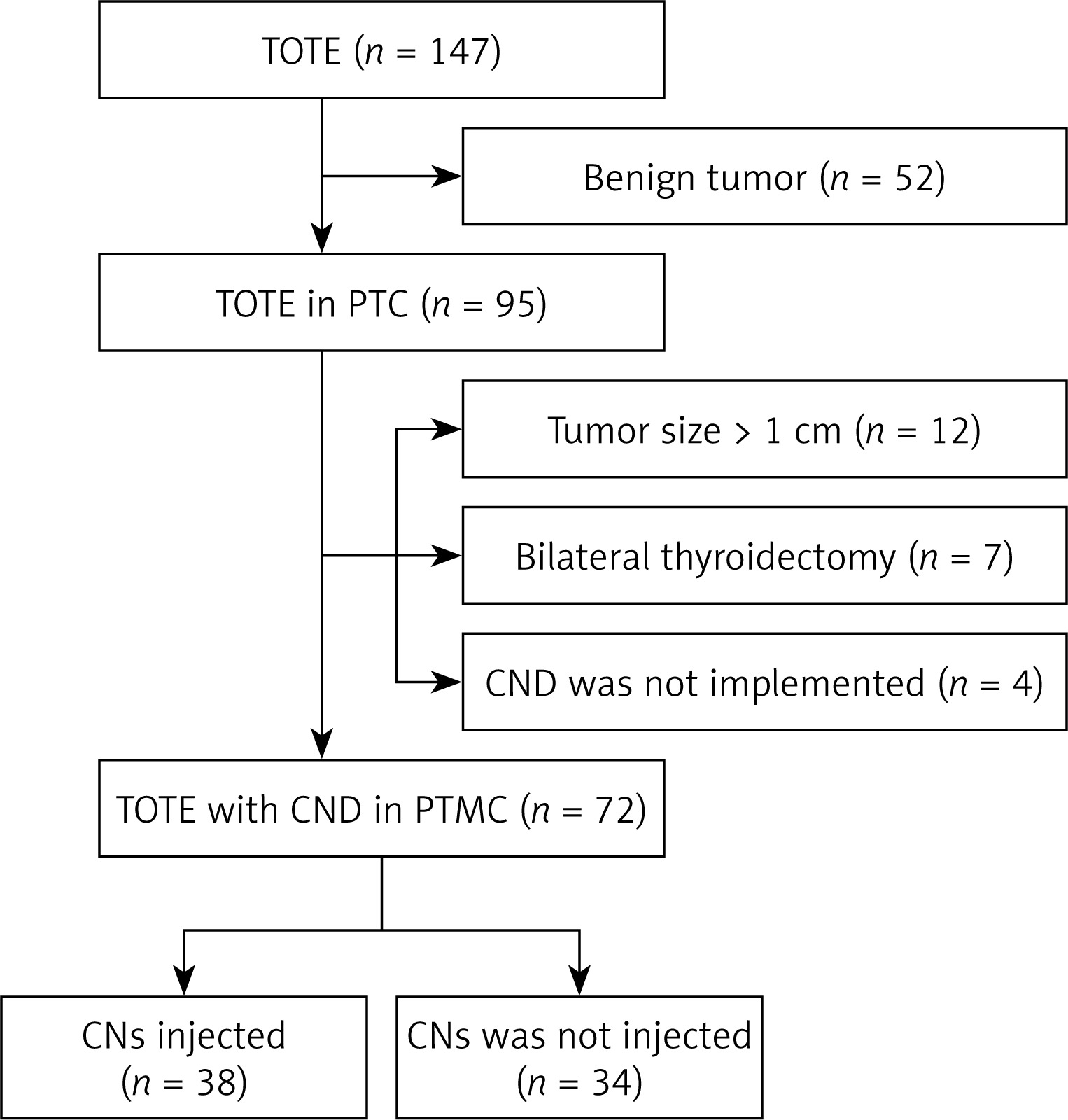
A retrospective review was performed using the records of 72 consecutive PTMC patients who underwent transoral vestibular unilateral thyroidectomy with CND in the Breast and Thyroid Surgery Department of Wuhan University from January 2017 to January 2019. Patients were preoperatively diagnosed with PTMC based on ultrasound guided fine needle aspiration cytology and were retrospectively divided into two groups: a CN group (n = 38) and a control group (n = 34). Patients were excluded if they met one or more of the following criteria: (1) contraindications for anesthesia, such as pregnancy, multiple organ failure, or mental disease; (2) history of neck surgery or radiotherapy; (3) concomitant Graves’ disease or a huge benign nodule; (4) evidence of local invasion or involvement of the recurrent laryngeal nerve (RLN); (5) preoperative imaging revealing enlarged and fused LNs; and (6) preoperative hypoparathyroidism or hypocalcemia.
All patients were informed in detail regarding the use of CN and that the cost of the drug would not be reimbursed. The intraoperative use of the drug was according to each patient’s own wishes. The technique used is standardized and reported in the literature [6, 12]. Approval from the Ethics Committee was not necessary.
Tracer
CNs (LUMMY Pharmaceutical Co., Chongqing, China) were injected as a suspension (50 mg suspended in 1 ml of 0.9% physiological saline) as the tracer (0.5 ml per ampoule). The dose for each patient was 0.15 ml.
Surgical technique
The TOET was performed under general anesthesia and in a supine position with neck extension. Following establishment of the working space, a dissection was made at the strap muscles with a Harmonic scalpel, and the strap muscles were pulled laterally with a retractor to exposure the thyroid gland. The CNs were then injected (Photo 1 A). Because of the endoscopic surgery, the CNs could not be injected under direct vision. A percutaneous puncture was made by locating the CN puncture site on the ceiling skin of the working space. A 22-gauge spinal needle was inserted and passed through the skin, subcutaneous fascia, and platysma until reaching the working space cavity and endoscopic view. The needle was then inserted into the thyroid parenchyma, and the CNs were injected into the thyroid gland as a 1.5 ml volume administered to the tumor lobe. After the injection, the syringe was pumped back to avoid injection into blood vessels, while taking care to avoid damage to the thyroid capsule and injection into the tumor. A slow injection speed was needed, and gentle pressure with gauze or absorbable gelatin sponge was applied at the needle puncture site to prevent solution leakage. The lymph vessels and the LNs were stained black. The PGs remained unchanged and were more easily identified and preserved during surgery.
Photo 1
Surgical procedure for transoral vestibular endoscopic thyroidectomy (TOET). 1 – Thyroid gland, 2 – sternocleidomastoid, 3 – superior parathyroid, 4 – inferior parathyroid, 5 – recurrent laryngeal nerve, 6 – black stained lymph node, 7 – unstained lymph node, 8 – trachea
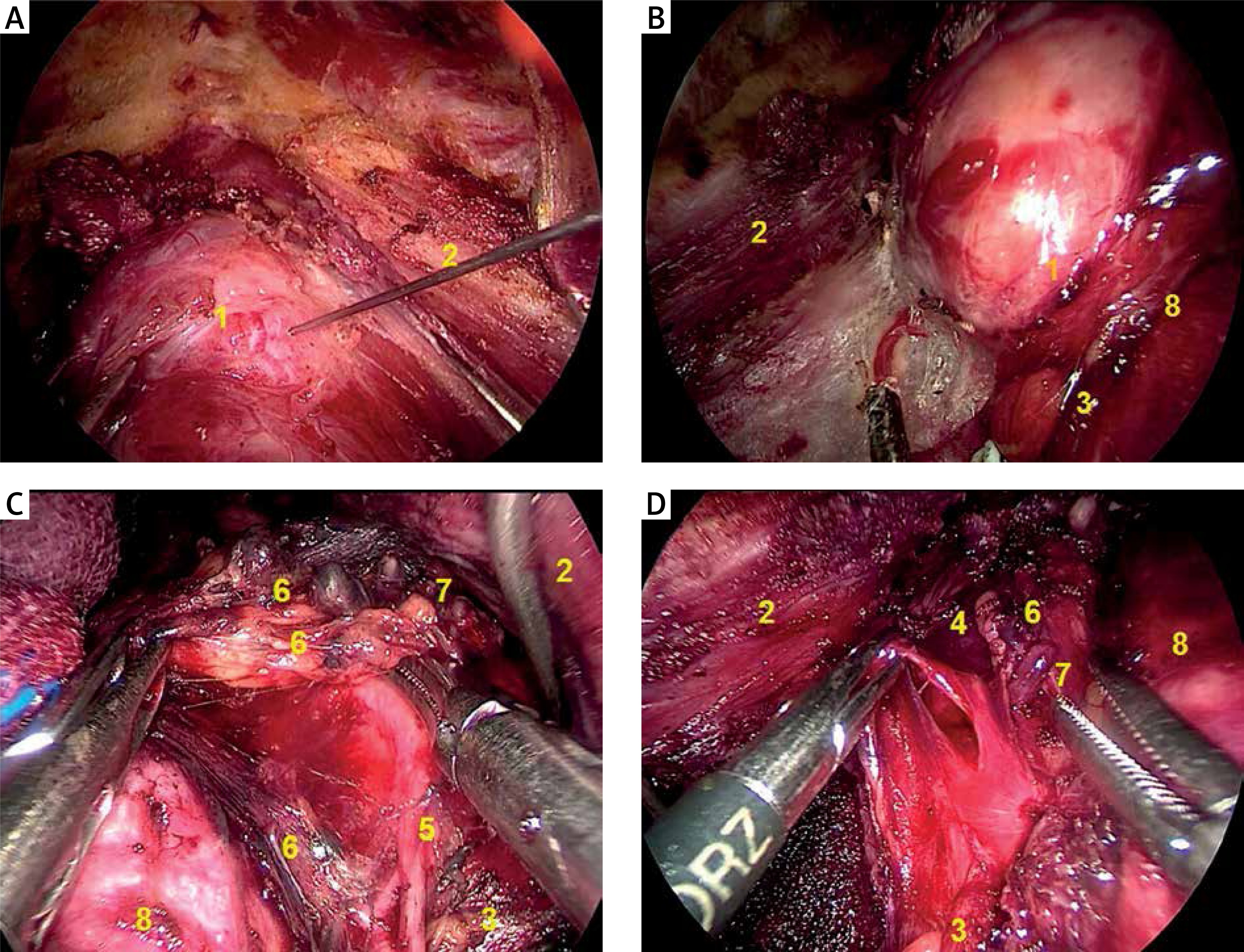
Part of the sternothyroid muscle was transected to expose the upper pole of the thyroid, and the superior PG could easily be seen by lifting the upper pole (Photo 1 B). The recurrent laryngeal nerve, which remained in its original position, was exposed by blunt dissection with endoscopic forceps (Photo 1 C). Once the inferior PG was found, it was released to the outside. The thyroid gland, including the nodule, was then removed. The CND, which included the prelaryngeal, pretracheal, and paratracheal lymph nodes, was then carried out. The resected LNs in the CN group were carefully checked and labeled as black-staining or unstained (Photo 1 D). Specimens were also checked for the presence of parathyroid tissue. Once the removal of parathyroid tissue was confirmed, the remainder of the specimen was autotransplanted into the sternocleidomastoid muscle [13, 14].
Study design
All patients underwent preoperative direct laryngoscopy to assess vocal cord motility. Ca2+ and PTH levels were also tested preoperatively. Pathological characteristics (e.g., number of LNs less than 5 mm removed, total number of LNs removed) and surgery-related indicators (e.g., operative time, blood loss, postoperative drainage, postoperative complications, and in situ preservation of the superior parathyroid and inferior parathyroid) were evaluated. The postoperative follow-up was performed by outpatient visits, telephone calls, and written correspondence. Data, including the serum Ca2+ and PTH levels, were gathered at postoperative day 1, week 1, month 1, and month 3. All patients received calcium gluconate (2.0 g/day) for 3 days, regardless of whether they showed a decline in serum or presented signs of hypocalcemia. After 3 days, the patients who still showed a decline in serum Ca2+ and presented signs of hypocalcemia continued taking these drugs.
Results
A total of 72 patients (68 female and 6 male) were selected over the period from January 2017 to January 2019, and all patients underwent endoscopic unilateral thyroidectomy with CND (level VI) (Figure 1). The clinical characteristics of the patients in both the CN and control groups are summarized in Table I. The patients ranged in age from 19 to 49 years, with a median age of 31 years. No significant differences were found in age, tumor side, sex, primary tumor size, operative time, blood loss, or postoperative drainage (all p > 0.05). No significant differences were noted in operative complications, including neuromuscular symptoms, transient recurrent laryngeal nerve palsy, and swallowing discomfort (all p > 0.05).
Table I
Characteristics and postoperative complications of patients in the CN and control groups
The dissected central neck lymph nodes and PGs preserved in situ in the CN and control groups are compared in Table II. A total of 340 LNs were detected in the CN group and 233 LNs in the control group. The mean number of detected LNs was significantly higher in the CN group than in the control group (8.9 ±3.8 vs. 6.9 ±2.7, p = 0.021). The resected number of dissected LNs < 5 mm was greater in the CN group than in the control group (3.2 ±1.4 vs. 1.8 ±0.8, p < 0.01).
Table II
Comparison of dissected central neck lymph nodes and parathyroid glands preserved in situ between the CN group and control group
| Characteristics | CN group N = 38 n (%) or mean ± SD | Control group N = 34 n (%) or mean ± SD | P-value |
|---|---|---|---|
| No. of dissected LNs (mean ± SD, per patient) | 8.9 ±3.8 | 6.9 ±2.7 | 0.021* |
| No. of dissected LNs < 5 mm | 3.2 ±1.4 | 1.8 ±0.8 | < 0.01* |
| Superior parathyroid glands preserved in situ | 34 (89.5) | 29 (85.3) | 0.592 |
| Inferior parathyroid glands preserved in situ | 29 (76.3) | 18 (52.9) | 0.038* |
| Parathyroid glands found in the central group of lymph nodes and autotransplanted | 6 (15.8) | 8 (23.5) | 0.407 |
No significant difference was found in the number of superior PGs preserved in situ (34 vs. 29, p = 0.592), but the number of superior PGs preserved in situ was greater in the CN group than in the control group (29 vs. 18, p = 0.038). No significant difference was found in the number of PGs found in the central group of lymph nodes and autotransplanted (6 vs. 8, p = 0.407).
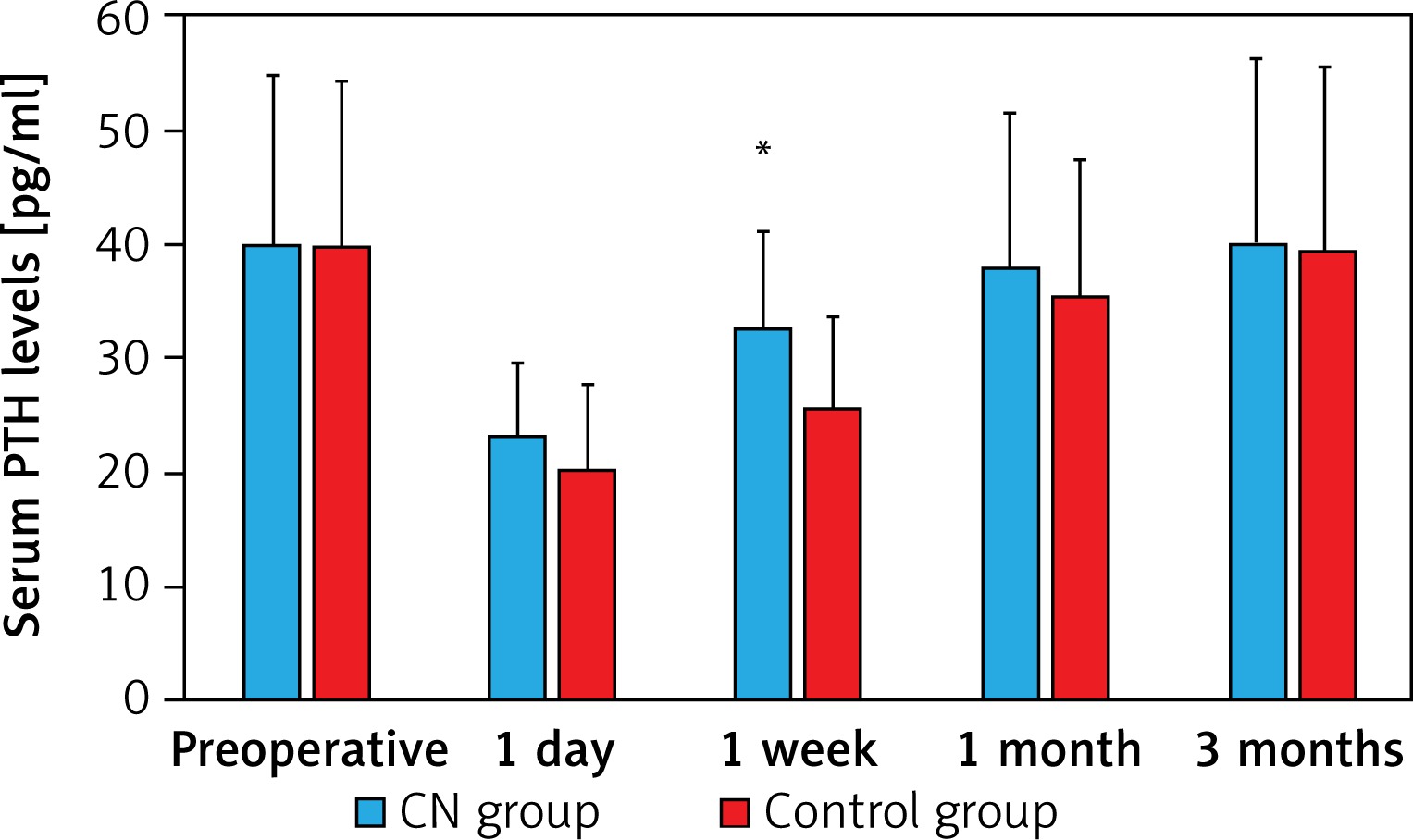
The serum PTH levels dropped markedly in each group on postoperative day 1 and week 1 (Figure 2). However, the PTH levels on postoperative day 1 were similar in both the CN and the control group (day 1, p = 0.946). These levels at postoperative week 1 were significantly lower in the control group than in the CN group (week 1, p = 0.014). The long-term results revealed similar PTH levels in both the CN group and the control group at postoperative month 1 and month 3 (month 1, p = 0.385; month 3, p = 0.827).
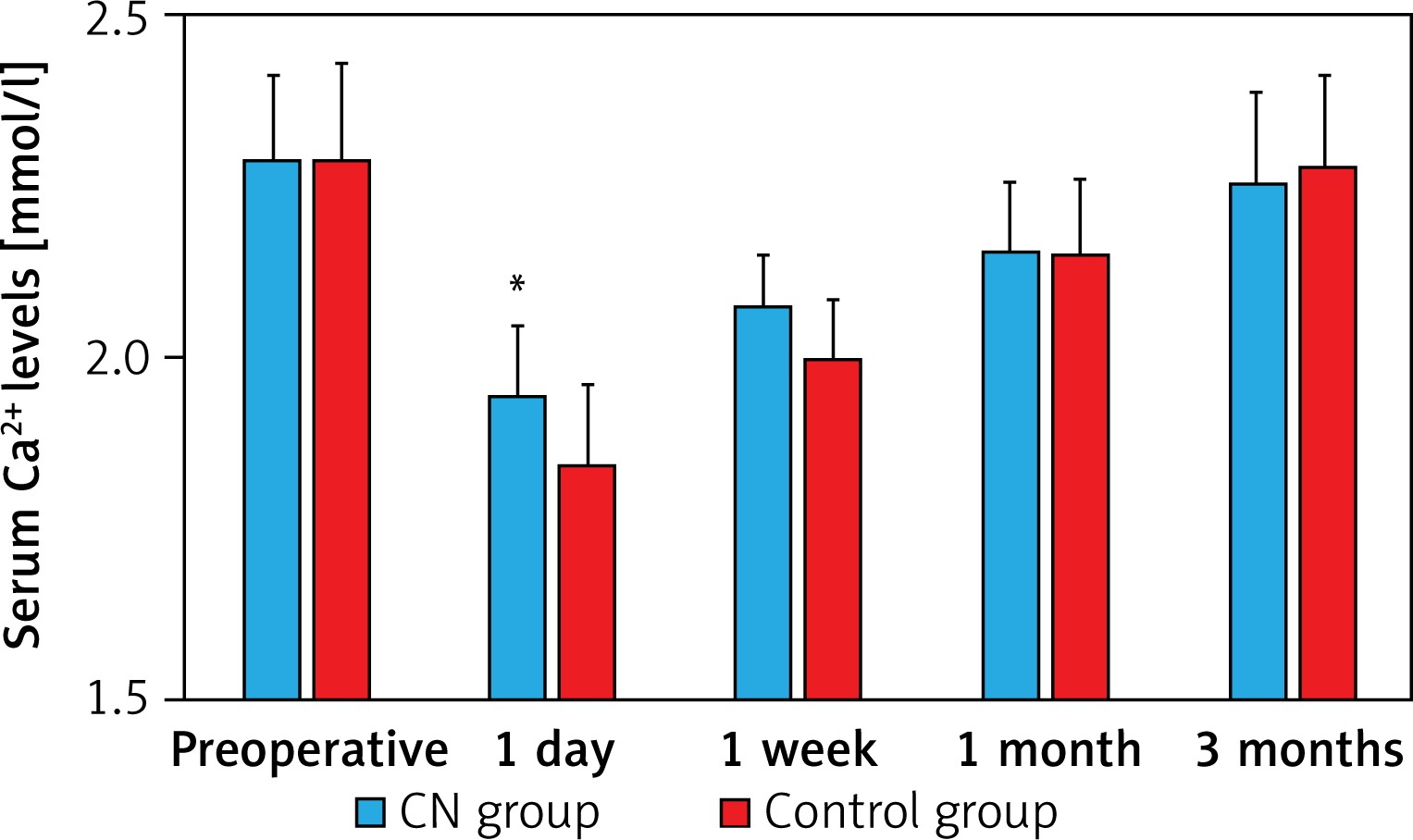
The serum Ca2+ levels at each detection point after surgery are shown in Figure 3. The levels on postoperative day 1 and at week 1 were significantly lower in the control group than in the CN group (day 1, p = 0.001; week 1, p < 0.01). The levels at postoperative month 1 and month 3 were similar in both groups (month 1, p = 0.829; month 3, p = 0.522).
Discussion
The development of endoscopic thyroid surgery techniques has led to the wide use of TOET for aesthetically conscious patients with PTMC. Under the magnified and high-resolution vision offered by endoscopy, TOET has advantages over traditional open surgery with respect to central lymph node dissection and protection of the PG blood supply. Our goal in the present study was to determine whether the use of CNs in TOET might further optimize the surgical effects.
The most popular tracer for LNs is methylene blue. However, it has poor specificity, the possibility of postoperative toxic metabolic encephalopathy, and the potential to mask the surrounding tissues and make anatomical structures unclear. Therefore, the utility of methylene blue is not widely accepted by thyroid surgeons. A variety of other techniques, including SPECT images, methoxyisobutylisonitrile scintigraphy using a gamma probe, 5-aminolevulinic acid, and optical coherence tomography, have also been reported but are without clinical effectiveness in terms of protection of the PGs [15, 16].
Recently, CN suspensions have been used to aid in the identification of lymph nodes in traditional open thyroid surgery. The product used is a stable suspension of CNs 150 nm in diameter, a size that ensures that the particles can pass through the lymphatic vessels rather than the blood capillaries. Following injection into the thyroid glands around a thyroid tumor, these CNs are rapidly captured by macrophages. The particles then enter the lymphatic vessels and accumulate in the lymph nodes, causing the thyroid and draining lymph nodes to darken. By contrast, the color of the PG remains unchanged and is more easily identified and preserved during surgery [17, 18].
The steps required for injection of the CN suspension are as follows: (1) the dose of CN suspension should be just 0.15 ml for each lobe, (2) a special needle, long enough for percutaneous injection of the CNs, is needed, and the front end of the needle is bent to help control the depth of the injection, (3) injection into blood vessels and tumors is avoided, (4) an ultrasonic knife is used for closing.
Temporary and permanent hypoparathyroidism occurring after surgery are mainly due to parathyroid contusions or a mistakenly cut or damaged blood supply [19, 20]. Marked drops in the serum Ca2+ and PTH after surgery imply that PG injury may be inevitable during thyroidectomy with central lymph node dissection. The location of the superior parathyroid gland is relatively constant, and no significant difference was found in discovery of the superior parathyroid preserved in situ (p = 0.592), Destruction of the inferior PGs may occur more frequently than destruction of the superior PGs because the inferior PGs are adjacent to the inferior pole of the thyroid and the region VI lymph nodes and because the inferior PGs are often obscured by the thyroid lobe in TOET. However, the use of CNs makes the inferior PGs and lymph nodes easier to identify, and the number of superior PGs preserved discovered in situ was greater in the CN group than in the control group (p = 0.038).
In this study, the number of LNs dissected was higher in the CN group than in the control group (p = 0.021). This may be due to the application of CNs, which enhanced certain smaller LNs or those located in the occult position, and the resected number of dissected LNs < 5 mm was larger in the CN group than in the control group (p < 0.01). However, we did not observe any significant differences in lymph node metastasis rates (28.2% vs. 27.0%) between the two groups. Our results also revealed no differences in the number of metastatic lymph nodes between the black-stained and unstained lymph nodes (28.8% vs. 26.5%), suggesting that the distribution of the CN lymph node tracer was not associated with lymph node metastasis.
The patients in both groups showed significantly lower serum Ca2+ and PTH levels than the preoperative levels at postoperative day 1 and week 1, and the changes in PTH levels were closely related to those of the Ca2+ levels. We found that patients who received the CN injection demonstrated small changes in the trends of PTH and Ca2+ levels postoperatively following surgery. The parathyroid function was also restored in a shorter time in the CN group.
This study had some limitations. Selection bias may have existed regarding which procedure was chosen, as this study is a retrospective study and not a blind randomized study. The follow-up period was also very short. The effect of CN use on the long-term outcomes of TOET is also unclear, and the sample size was too small.