
Introduction
Malignant skin neoplasms constitute a group of diseases that attract attention of physicians across multiple specialties, from general practitioners, oncologists, and dermatologists to general, oncologic, and plastic surgeons. The most common malignancies include keratinocyte carcinomas (KCs) and cutaneous melanoma (CM). KCs include basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). Other malignant skin neoplasms are significantly less common.
One of the most important risk factors for both CM and KC is excessive exposure to ultraviolet (UV) radiation. Therefore, year-round application of sunscreen is the primary protective recommendation. From a public health perspective, early detection and prompt surgical excision are crucial in the management of CM and KC. Any patient with a suspicious skin lesion should undergo a dermatoscopic examination, as it provides the highest diagnostic sensitivity and specificity [1].
According to data from the Polish National Cancer Registry (PNCR), in 2022, CM (ICD-10 code C43) and other malignant skin neoplasms (ICD-10 code C44) collectively constituted 10.9% of all registered malignant neoplasms in Poland [2]. Despite ongoing public education efforts, the incidence of skin malignancies has shown an increasing trend. An exception to this pattern was observed during the COVID-19 pandemic, when the number of diagnosed cases declined, primarily due to the limited access to healthcare facilities and increased mortality associated with comorbid conditions. In 2021, an unprecedented 24% decrease in malignant skin neoplasm diagnoses was noted compared to the previous year. However, in 2022, the number of registered cases reached 19,744, which was the highest figure recorded in the history of the PNCR since data collection began in 1999 [3].
In our previous study, we analysed cases of patients with malignant skin neoplasms treated at the Department of Plastic, Reconstructive, and Aesthetic Surgery in Lodz between 2020 and 2022 [4]. The obtained results were compared with those from a corresponding patient group from 2017–2019 [5]. A decline in the number of KC and CM cases was observed, from 387 in 2017–2019 to 241 in 2020–2022 (–37.7%). Further detailed analysis included demographic data, histopathological findings, as well as tumour size and location.
Aim
The aim of this study is to present the topographic trends in head skin cancers treated at our Department during the period of 8 years with the analysis of correlations between the type of cancer and its location. Due to the functional and aesthetic aspects of the face, detailed knowledge of the occurrence of facial malignancies seems to be particularly important.
Material and methods
This study is an epidemiological, descriptive, and retrospective analysis based on histopathological records from the Department of Plastic and Reconstructive Surgery in Lodz. Located in central Poland, as well as central Europe, the city has a temperate climate. The population is predominantly composed of white Europeans, forming a relatively homogeneous group. Data were collected over an 8-year period, from January 2017 to December 2024.
The following variables were selected for detailed evaluation: patient sex, age, type of skin cancer, BCC subtype, SCC grading, and anatomical location of the lesions on the head. The examined regions included the forehead, ear, nose, eye region, perioral area, cheek, scalp, and temple. The orbital region was further subdivided into four subregions: upper eyelid, lower eyelid, medial canthus, and lateral canthus.
Statistical analysis
Quantitative variables were characterized using the mean value ± standard deviation (SD). Qualitative variables were presented as frequencies and percentages. Comparisons of qualitative variables were performed using the χ2 test for proportions (two-sided). The Shapiro-Wilk test was used to assess the normality of the distribution of quantitative variables. A p-value of < 0.05 was considered statistically significant. Data were organised using Microsoft Excel spreadsheets and analysed with Statistica v.13.1 (StatSoft Inc., Tulsa, OK, USA) for Windows.
Results
A total of 649 patients were included in the study (n = 420, 64.7% women; n = 229, 35.3% men), resulting in 786 head skin cancers diagnosed over an 8-year period. Both sexes had a similar age distribution. The average age of the study group was 71.8 ±11.3 years; the mean age of men was 71.7 ±11.1 years, and the mean age of women was 71.9 ±11.4 years.
The nasal area was the most frequently affected anatomical site for skin cancer occurrence (n = 205, 26.1%), followed by the orbital area (n = 175, 22.3%) and the cheek area (n = 154, 19.6%) (Table 1). These three areas accounted for approximately 68% of all head skin cancer cases.
Table 1
Study group characteristics
| Feature/variable | n | %, SD |
|---|---|---|
| Sex | ||
| Men | 229 | 35.3 |
| Women | 420 | 64.7 |
| Total cancers | 786 | |
| Area | ||
| Frontal | 73 | 9.3 |
| Auricular | 46 | 5.9 |
| Nasal | 205 | 26.1 |
| Orbital | 175 | 22.3 |
| Perioral | 26 | 3.3 |
| Cheek | 154 | 19.6 |
| Scalp | 41 | 5.2 |
| Temporal | 66 | 8.4 |
The BCC was the most common skin cancer observed in this study (n = 664, 84.5%). The subtypes of BCC are presented in Table 2. The nodular subtype was identified in 503 cases, representing approximately 75% of all BCCs. The second most common malignancy was SCC, diagnosed in 111 (14.1%) cases. Among SCCs, grade 1 was the most frequent (n = 42, 37.8%). Melanoma was identified in 6 (0.8%) cases, ranking third in frequency. The least common types, classified as “other” (n = 5), included eccrine carcinoma, trichoblastic carcinoma (2 cases), angiosarcoma G2, and hidradenocarcinoma.
Table 2
Number of skin cancers and their subtypes
| Cancer | n | % | Subtype | n | % |
|---|---|---|---|---|---|
| BCC | 664 | 84.5 | |||
| Cysticus | 10 | 1.5 | |||
| Exulcerans | 39 | 5.9 | |||
| Infiltrativus | 67 | 10.1 | |||
| Nodularis | 503 | 75.8 | |||
| Superficial | 25 | 3.8 | |||
| Basospinocellulare | 20 | 3.0 | |||
| SCC | 111 | 14.1 | |||
| In situ | 39 | 35.1 | |||
| G1 | 42 | 37.8 | |||
| G2 | 26 | 23.4 | |||
| G3 | 4 | 3.6 | |||
| Melanoma | 6 | 0.8 | |||
| Other | 5 | 0.6 | |||
Analysis of the anatomical distribution of skin cancers revealed statistically significant differences in lesion prevalence between BCC and SCC across several regions (Table 3) and was illustrated in Figure 1. In the auricular area, SCC was significantly more frequent than BCC (19.8% vs. 3.6%; p < 0.0001). Conversely, in the nasal region, BCC predominated markedly over SCC (29.1% vs. 9.0%; p < 0.0001). A similar trend was observed in the orbital area, where BCC was more common than SCC (24.2% vs. 9.9%; p = 0.0008). In the cheek area, SCC was more frequent (27.0%) compared to BCC (18.1%), with the difference being statistically significant (p = 0.0282). On the scalp, SCC also exceeded BCC in frequency (9.9% vs. 4.2%; p = 0.0109). No statistically significant differences were observed in the frontal (p = 0.8411), perioral (p = 0.0670), and temporal (p = 0.8615) regions.
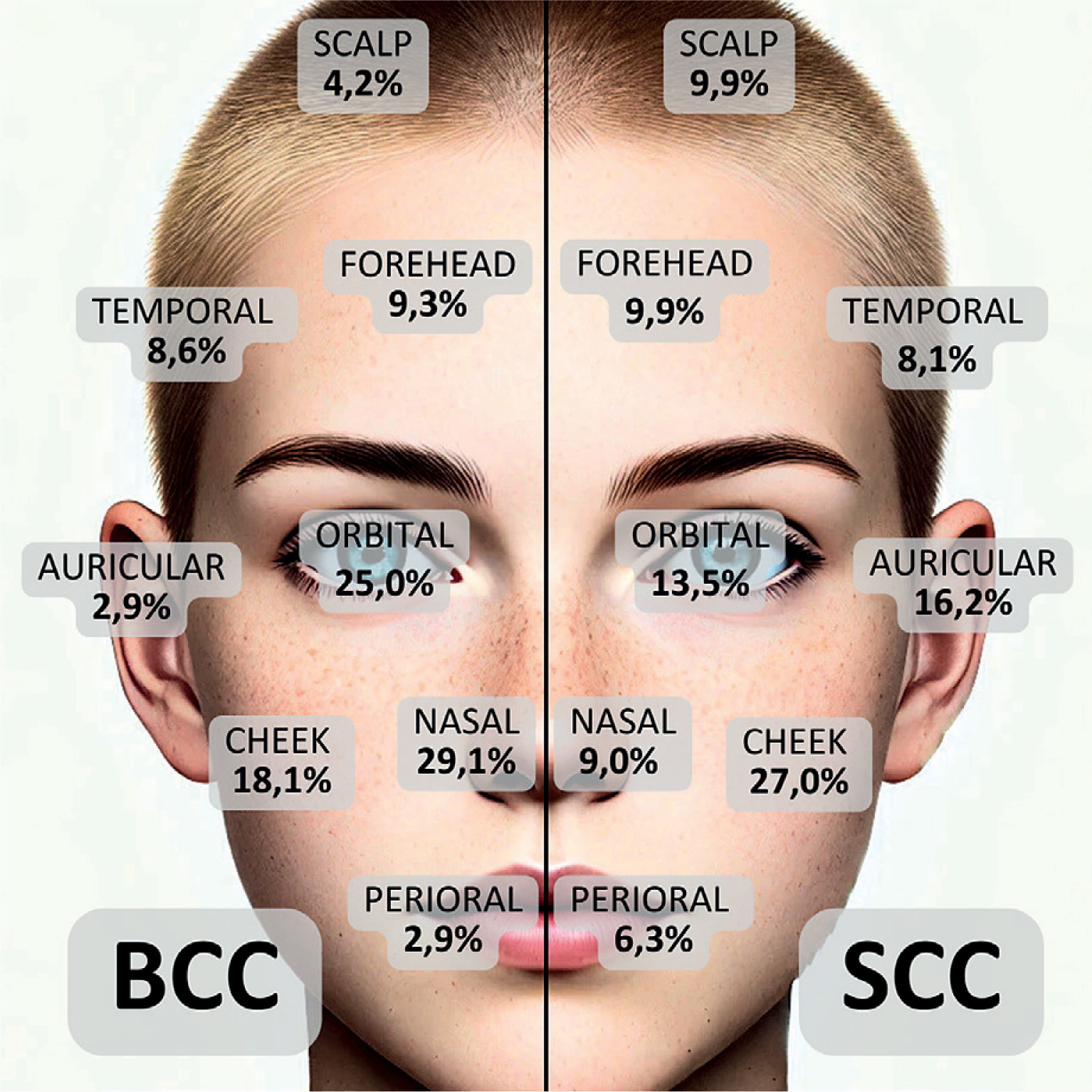
Table 3
Occurrence of keratinocyte carcinomas depending on the anatomical area
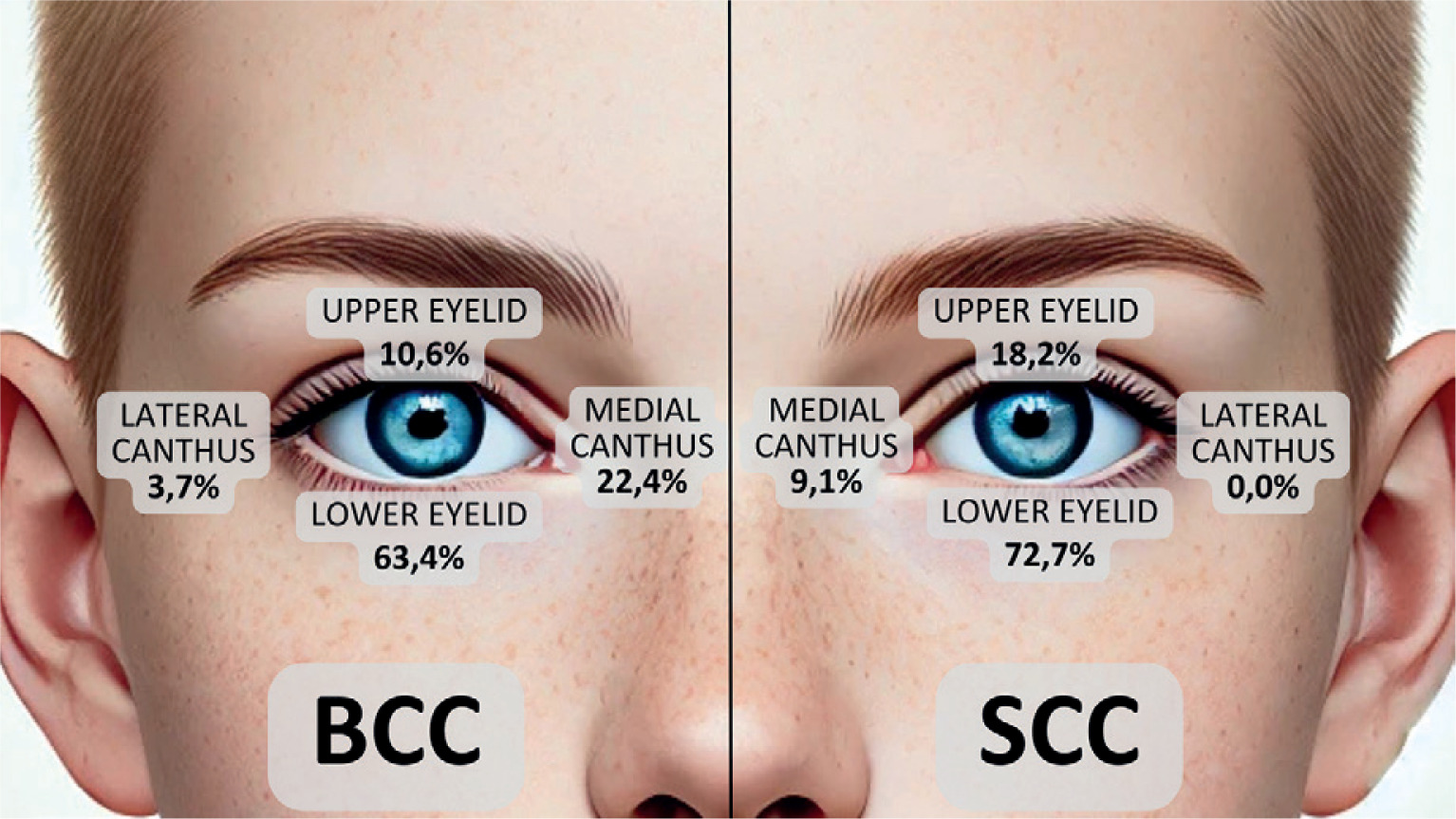
In the orbital region, the lower eyelid was the most frequently affected subregion (Table 4, Figure 2), accounting for 63.4% of BCCs and 72.7% of SCCs. This was followed by the medial canthus (22.4% of BCCs; 9.1% of SCCs), the upper eyelid (10.6% of BCCs; 18.2% of SCCs), and the lateral canthus, which was the least affected area (3.7% of BCCs; 0% of SCCs).
Discussion
The head and neck region is the most prominent location for skin malignancies with a ratio up to 90% [6]. Skin cancers usually develop in sun-exposed areas and locations like nasal, nasolabial, periorbital, auricular and temporal are recognized as high-risk locations of the face [6]. These regions are sometimes called as “mask area” or “H-zone” due to their aesthetic and functional importance [6].
What is also characteristic, skin cancers usually occur in elderly people. In a study performed by González et al. [7] the mean age at diagnosis of skin cancer was 74 years. Slightly older patients were observed by Beecher et al. [8], a total of 245 primary cutaneous cancers of the ear were described with the average age at diagnosis of 75 years. The opposite trend was presented by Donaldson et al. [9]; the mean age of patients in their series was 65.2 years, with males being older than females (66.8 vs. 63.0 years). In a retrospective analysis performed by Özgür et al. [6] the mean age of patients was 71.4 ±11.05 years. Similar results were shown in our study – the average age of patients was 71.8 ±11.3 years and both sexes had a similar age distribution (males: 71.7 ±11.1 years and females: 71.9 ±11.4 years). Taking into account the fact of an aging society, it must be borne in mind that the number of skin cancer cases in the elderly will increase.
The strength of our study, first of all, is the fact that it was based on a large population of patients with facial skin malignancies. Second of all, a detailed topographic map of face tumours divided into anatomical regions is presented. The dominance of BCC was observed in the nasal and orbital face regions, while SCC was significantly more frequent on the ear, scalp and cheek. Wu et al. [10] presented a large series of periocular BCC, where most cases affected the lower eyelid, followed by medial canthus, lateral canthus and upper eyelid. In our study we also showed that the lower eyelid was mostly affected, this is probably due to UV exposure and the fact that the lower eyelid is not as mobile as the upper one. However, contrary to the aforementioned authors, in our group BCC was rarely located on the lateral canthus. This may be due to the fact that the studies concerned different populations (Europeans versus Australians) or it may be a consequence of the factor that the area of the lateral canthus seems less demanding from the surgical perspective and patients visit specialists other than plastic surgeons (dermatologists, oncologists, ophthalmologists, general surgeons).
In the literature we can also find articles confirming that auricular location is predominant for SCC and not BCC [6–8]. Beecher et al. [8] believe that this is due to the different behaviour of the skin of the ear. Overall, it is thought that thin skin, lack of subcutaneous adipose tissue, and close underlying cartilage contribute to a wider subclinical extension and horizontal growth along the dermis and perichondrium, often making initial adequate resection difficult by conventional methods. Additionally, Chopra et al. [11] concluded that the greatest epidermal, dermal and total skin thickness were found in the upper lip, right and left lower nasal sidewall and the least epidermal skin thickness was in the posterior auricular skin. However, the least dermal skin thickness, and the least total skin thickness, are both in the upper medial eyelid [11].
Immunological and microenvironmental factors may also play a role. UV radiation not only damages DNA, but also locally reduces skin immunosurveillance – leading to Langerhans cell atrophy and production of immunosuppressive cytokines (e.g. IL-10) [12]. The skin of the auricle, permanently exposed to the sun, may have an impaired local immune response, which facilitates the survival of cells with mutations and the development of cancer. This phenomenon is clearly visible in patients after organ transplantation on immunosuppression – the frequency of SCC increases dramatically in them (SCC then dominates over BCC), which emphasizes the importance of immunosurveillance in controlling squamous cell carcinogenesis. One can speculate that the poorly vascularized cartilage underlying the skin of the ear does not favour the influx of immune cells, which creates a microenvironment that allows SCC to grow more easily.
It is also worth mentioning the differences in receptor expression: SCC often shows high expression of epidermal growth factor receptors (EGFR) and increased activity of proinflammatory pathways (COX-2, proinflammatory cytokines), which is associated with its more aggressive growth and is a target for therapy (e.g. cetuximab – an anti-EGFR antibody – is sometimes used in advanced SCC) [13, 14]. In BCC, on the other hand, similar EGFR overexpression is not typically observed, and the dominant Hedgehog pathway makes it sensitive to inhibitors of this pathway (vismodegib, sonidegib) [15]. It is possible that in the ear skin – chronically exposed to UV – cytokines and EGFR ligands are induced, supporting the development of SCC at the expense of BCC. Although these relationships are not yet fully understood, studies on skin photoaging suggest certain mechanisms: men more often experience so-called atrophic photoaging (thin, wrinkled, sensitive skin with telangiectasia), which is associated with a tendency to develop invasive skin cancers; women have a predominant hypertrophic photoaging (thicker, more elastic skin with a tendency to deep wrinkles, but a lower incidence of cancers) [16]. The skin of the ears of older men is a textbook example of atrophic sun-damaged skin – this may explain the predisposition to the multiplication of SCC cancer cell clones in this particular location.
UV radiation is the most important environmental factor explaining the prevalence of SCC on the ear [6–8, 13]. The auricles are often exposed to direct sunlight – especially in people with short hair or balding. Studies show that almost all cases of SCC of the ear occur in men, which is explained by shorter hair and lack of sun protection for the ears. In men, the ears are exposed and regularly exposed to UV rays, while women are more likely to be protected by hairstyles or head coverings [6–8]. Furthermore, men are more likely to work or spend time outdoors and are less likely to use sunscreen on their ears and scalp. In consequence this leads to cumulative sun damage to the skin of the ear. The sun has a doubly damaging effect here: it causes DNA mutations in skin cells and causes local immunosuppression, which was discussed above. As a result, the ears – along with the lower lip, nose, cheeks and scalp in balding people – are among the areas most likely to develop SCC.
It is worth noting that BCC is also associated with the sun, but with a slightly different type of exposure. BCC appears more often on areas of the face that have experienced intense sun exposure (e.g. nose, forehead) – however, on the ear, despite high exposure, BCC is relatively rare [17]. This may be due to the fact that the skin of the ear is exposed to other environmental factors in addition to the sun: mechanical injuries (e.g. in people wearing helmets, headphones, earphones), irritation (abrasion by glasses or clothes), as well as extreme conditions (wind, cold causing frostbite). Each of these factors can act as a promoter of squamous cell carcinogenesis – e.g. chronic irritation or healing of minor wounds promotes the development of SCC (a phenomenon similar to the development of SCC in scars or chronic ulcers, the so-called Marjolin ulcer) [18]. BCC does not show such a strong connection with chronic injuries – it more often develops de novo [17]. In turn, the microenvironment of the skin on the ear – relatively dry, devoid of sweat glands (outside the auditory canal) and sebaceous glands in large numbers – may promote keratinization and drying of the epidermis. Dry, keratinized skin, in turn, is more susceptible to actinic damage (solar keratosis) leading to SCC. Additionally, the auricles protrude from the head profile, which is why they often “catch” perpendicular UV rays (e.g. the tip of the ear is positioned horizontally upwards, exposing itself to full sun in the summer). There is no natural shade or protection – even baseball caps protect the face, but the ears remain uncovered. This constant local exposure translates into a field of dermatosis – the entire field of the ear skin can be covered with precancerous changes, from which SCC can develop in multiple foci.
It seems that SCC is more common in the auricle than BCC due to the overlap of many anatomical, molecular and environmental factors. The thin, poorly protected skin of the ear, lacking a thick subcutaneous layer and directly exposed to UV radiation, provides a fertile ground for neoplastic transformation of keratinocytes. UV radiation induces numerous DNA damages (especially p53 mutations) and precancerous changes (actinic keratosis) in the cells of the spinous layer of the epidermis – leading to the formation of SCC [19–21]. At the same time, UV impairs local immunosurveillance, allowing these mutated cells to survive. In turn, BCC, although also associated with the sun, requires transformation of the basal cell layer (often within the hair follicle) – there are fewer such cells in the ear, and the molecular mechanisms driving BCC (Hedgehog pathway mutations) seem to be less frequently initiated or sustained in this environment [15, 17, 22]. In addition, demographic factors play a role: the auricle is more exposed in men (short haircut, omitting the ears during photoprotection) and it is mainly in them that the predominance of SCC on the ear is observed.
Conclusions
Our study provides an accurate mapping of facial skin cancers over an 8-year period, highlighting nodular BCC as the predominant subtype. We confirmed a statistically higher incidence of BCC in the nasal and periorbital areas, and SCC in the auricular and scalp regions. These findings underscore the importance of the anatomical site in the clinical assessment and diagnosis of skin cancers and may guide more targeted preventive and therapeutic strategies.







